


Abstract
Background: Physical activity is known to prevent frailty and reduce its consequences; however, it remains unclear which interventions are optimal for older adults with frailty. We conducted a systematic review and meta-analysis to identify effective physical activity interventions in improving outcomes related to frailty.
Methods: We searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials and CINAHL (inception to July 2019) for English-language randomized controlled trials (RCTs) of physical activity interventions in adults aged 65 years or more who were prefrail or frail; we included observational and cohort studies when there were no RCT data. Outcomes of interest were frailty, mobility, physical function, cognitive function, use of health care services and quality of life. After data extraction, we assessed the risk of bias using the Cochrane Collaboration risk of bias tool for RCTs and the Newcastle–Ottawa Scale for observational studies, rated the certainty of evidence with the Grading of Recommendation, Assessment, Development and Evaluations (GRADE) approach, and assessed statistical and methodologic heterogeneity.
Results: We identified 26 studies (24 RCTs [1 of which did not have any relevant outcomes for extraction] and 2 observational studies) involving 8022 prefrail or frail older adults. Nine studies had low risk of bias, 2 had high risk of bias, and for 13 the risk of bias was unclear. The trials included mixed (aerobic and muscle-strengthening) (n = 13), muscle-strengthening (n = 8), mobilization and rehabilitation (n = 4) or aerobic (n = 1) activities. Significant effects were found for mobility (standardized mean difference [SMD] 0.60, 95% confidence interval [CI] 0.37 to 0.83), activities of daily living (SMD 0.50, 95% CI 0.15 to 0.84), cognitive function (SMD 0.35, 95% CI 0.09 to 0.61), quality of life (SMD 0.60, 95% CI 0.13 to 1.07) and frailty (SMD −1.29, 95% CI −2.22 to −0.36; risk ratio 0.58, 95% CI 0.36 to 0.93), with moderate certainty of evidence.
Interpretation: There is low-to moderate-level evidence that various physical activity interventions are beneficial for prefrail and frail older adults. Studies need to better define frailty to ensure the identification and implementation of such interventions into clinical practice.
PROSPERO registration: CRD42020144556
Frailty is a leading contributor to functional decline and premature mortality in older adults.1 More than 1.5 million Canadians are currently diagnosed as medically frail, and this number is expected to rise to more than 2 million in the next 10 years.2 Frailty is a syndrome resulting from multiple factors and impairments that can reduce a person’s functional ability. One of the major components of frailty is decline in physiologic domains such as loss of muscle mass and strength, flexibility, balance, coordination and performance.3 Older adults with frailty are at increased risk for falls, decline in mobility, hospital admission and death,4,5 which results in high consumption of health care resources,6 an increased burden on caregivers and adverse health outcomes.7
With the increase in older adults with frailty and the social and economic impact of this syndrome, research has focused on ways to prevent, delay and treat frailty, but proper identification and measurement of frailty is necessary to measure these changes and optimize care and treatment.2 Evidence shows a link between regular physical activity and improved muscle strength, aerobic capacity and balance in older adults in general8 and in those with frailty.9–11 However, much of this research has been conducted in populations in which frailty has not been clearly defined or measured. This has led to a gap in the literature: recommended physical activity12,13 may be too advanced or too intense for a frailer population, putting them at risk for falls and injuries.
Previous reviews looking at physical activity interventions for frail older adults have given mixed results,4,9,14–16 so it is still unclear what the best interventions are to support these people, especially in a population that has been clearly identified as frail. Such a defined population is important to support the creation of guidelines to enable evidence-based clinical practice.
We conducted a systematic review and meta-analysis focused on physical activity interventions in older adults with prefrailty or frailty (as identified by a tool or assessment) to assess the effectiveness of the interventions in improving outcomes including frailty, mobility, physical function (e.g., activities of daily living [ADLs], fatigue level, falls), cognitive function, use of health care services (e.g., hospital admissions) and quality of life. The results of this review, along with those of a methodologically similar review focused on nutrition and combined nutrition plus physical activity interventions,17 will provide the scientific evidence for the clinical practice guidelines of the Canadian Frailty Network.
Methods
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.18 The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO-CRD42020144556). There were minor variations from the published protocol. These included application of the English-only language restriction on screening rather than as part of the search, and reporting on only the outcomes listed in the protocol that were ranked critical based on the voting of a guideline panel committee. Our methods followed the Cochrane Handbook for Systematic Reviews of Interventions.19
Key question
What is the effectiveness of physical activity interventions in older adults (aged ≥ 65 yr) with frailty or prefrailty on clinical outcomes, outcomes that are important to the patient and outcomes related to use of health care services?
Search strategy
We developed the search terms, databases and strategy in consultation with a research librarian; they were informed by previous systematic reviews14–16 (Appendix 1, available at www.cmajopen.ca/content/9/3/E728/suppl/DC1). We searched MEDLINE (1948 to July 2019), Embase (1974 to July 2019), the Cochrane Central Register of Controlled Trials (2019, Issue 6) and CINAHL (1937 to July 2019) and manually searched reference lists of relevant reviews and included studies not captured in our search. The search results were deduplicated, and citations were uploaded to a secure Internet-based platform for screening (DistillerSR, Evidence Partners).
Eligibility criteria
The PICO (population, intervention, comparator, outcomes) inclusion and exclusion criteria are provided in Box 1.
Population, intervention, comparator, outcomes (PICO) eligibility criteria
Population
Adults aged ≥ 65 yr clearly identified as prefrail or frail with any frailty assessment tool, assessment of frailty or other explicit author-established criteria (including studies with subanalyses involving a portion of prefrail or frail participants)
To make this review relevant to the general frail population, studies that targeted clinical populations, such as patients with obesity or cancer, were excluded
Intervention
Physical activity interventions
Comparator
True control group defined as having received usual care, routine care or minimal contact that did not include any intervention or treatment group components
Any head-to-head interventions were excluded
Outcomes
Frailty (measured with a valid tool)
Mobility (e.g., gait speed, Timed Up and Go test, Sit-to-Stand test, balance test and Short Physical Performance Battery)
Physical function (e.g., activities of daily living, energy and fatigue levels, falls, fall rate, fall incidence)
Cognitive function (e.g., Loewenstein Occupational Therapy Cognitive Assessment, Mini-Mental State Examination)
Use of health care services (e.g., hospital admission, emergency department visits)
Quality of life (measured with a standardized tool)
We included English-language peer-reviewed studies primarily from randomized controlled trials (RCTs); we included observational and cohort studies only when there were no RCT data. There was no exclusion based on intervention or participant setting.
Outcomes of interest were selected by an interdisciplinary steering committee (L.G., H.K., J.H-L., A.G., A.T., D.R.B., J.M.) through a voting process that involved gathering a comprehensive list of outcomes from clinical and research expertise as well as existing relevant systematic reviews. The committee identified any missing outcomes and then anonymously rated the importance of the incomes on a scale from 1 to 9 (1–3: not important; 4–6: important; 7–9: critical). Authors not involved in the ranking process (D.S., D.F-L., M.R.) averaged the scores for each outcome and provided the list of outcomes to the committee for final discussion and agreement.
Study selection, data extraction and quality assessment
A series of team members were involved in the screening process, which resulted in different combinations of reviewers and team members. At all levels of screening, all articles required a minimum of 2 reviews. Multiple publications for the same primary intervention were merged; all data from all publications from a single study were extracted for relevant outcomes, but we describe the study and its characteristics only once in our review.
We developed, piloted and deployed standardized forms for data extraction. These forms were templated based on our experience and expertise as methodologists and included details such as outcome type, tool used, and intervention and control group data. The forms were then tested independently by 2 researchers to ensure there were no errors or misinterpretation. Two team members then completed full data extraction (unadjusted, intention-to-treat data) and an assessment of risk of bias using the Cochrane Collaboration risk of bias tool20 for RCTs and the Newcastle–Ottawa Scale21 for observational studies. If interventions had multiple treatment arms, only the interventions that met our inclusion criteria were extracted. Conflicts were resolved by the lead researcher of this review (M.R.), and all data extraction was verified independently by the statistician (M.U.A.).
Data on harms or adverse events were extracted narratively.
Certainty of evidence
We independently evaluated the certainty of the body of evidence using the Grading of Recommendation, Assessment, Development and Evaluations (GRADE) approach22 with GRADEpro software. With this approach, the certainty of a body of evidence is rated as high, moderate, low or very low based on assessment of 5 conditions: methodologic quality; consistency across effect estimates and statistical heterogeneity; directness of the body of evidence to the populations, interventions, comparators or outcomes of interest; precision of results; and indications of reporting bias.
Statistical analysis
The physical activity components and intensities extracted from the search are shown in Appendix 2 (available at www.cmajopen.ca/content/9/3/E728/suppl/DC1). All data analyses were planned a priori. We used a meta-analysis to combine the results across all studies by outcome using the published data from included studies (full methods presented in Appendix 3, available at www.cmajopen.ca/content/9/3/E728/suppl/DC1).
We also conducted an analysis of the effectiveness of each physical activity category by outcome. For continuous outcomes, we used the change from baseline to immediately after the intervention (mean change score, standard deviation [SD] of mean change score) for both the intervention group and the control group to generate the summary measures of effect in the form of standardized mean difference (SMD).23 We used SMD as a summary statistic because many studies in this systematic review assessed the same outcome measured in a variety of ways (e.g., mobility measured as stair climb, balance test, gait speed, chair rise repetition, Sit-to-Stand test, Short Physical Performance Battery, gait speed, Timed Up and Go test). In this situation, it was necessary to standardize the results of the studies before they could be compared across studies or combined in a quantitative synthesis. The SMD-based effect sizes represent the magnitude of the intervention effect relative to the variability observed in a particular study. Therefore, studies for which the difference in mean change score was the same as the proportion of SD of mean change score have the same SMD, regardless of the actual scale or unit of measurement used to obtain the outcome measures. 19,24 The SMD is interpreted based on its magnitude according to recommended Cohen d thresholds (~0.2 = small effect, ~0.5 = medium effect, ~0.8 = large effect).25 For studies in which measure of variance was reported as confidence intervals (CIs), standard error or p values, we used Cochrane-recommended methods to convert these data to SD.19
We used a multilevel meta-analytical approach (where applicable) to account for statistical dependence, that is, dependency in effect sizes introduced by comparison of multiple intervention arms within a study to a common control group, or by multiple outcome measures or suboutcome measures of a primary outcome of interest within a study (such as Short Physical Performance Battery reported as gait speed, balance and chair stand test separately).26 In such cases, we nested the correlated measures or effect sizes within studies first, by introducing a random effect to our grouping variables such as studies, outcome measures and intervention arms. This grouping variable, also known as a random intercept, told our model to assume different values (intercepts) for each grouping level. Specifically, we used 2 grouping variables: that on level 2 and that on level 3. We assumed that these grouping variables are nested, in the sense that several effect sizes on level 2 together make up a larger cluster on level 3. For pooling of performance measures, we adjusted the direction of effect to ensure consistency of desirable outcome responses.
For dichotomous outcomes, we used the number of events after the intervention to generate the summary measures of effect in the form of risk ratio (RR) using DerSimonian and Laird random-effects models with the Mantel–Haenszel method. We used the Cochran Q test (α = 0.05) to detect statistical heterogeneity and the I2 statistic to quantify the magnitude of statistical heterogeneity between studies, where an I2 value of 30%–60% represents moderate heterogeneity and a value of 60%–90% represents substantial heterogeneity across studies.
We estimated the statistical heterogeneity I2 statistic in the context of the multilevel meta-analytical approach.24,26 We estimated I2–level 2 to account for the amount of within-cluster heterogeneity (i.e., across effect sizes or multiple arms of same study), I2–level 3 to account for between-cluster heterogeneity (i.e., effect sizes across studies or subgroups of interest) and I2–total to represent the heterogeneity not attributable to sample error (sum of values at levels 2 and 3). We added I2–total to all forest plots for overall pooled effect estimates and summary effect size within subgroups.
We assessed publication bias using funnel plots27 when there were at least 10 studies in the meta-analysis.
We performed all analyses using R software (metafor and dmetar packages) (R Foundation for Statistical Computing).
Ethics approval
As this study was solely literature based, it was not eligible for institutional ethics approval, and none was sought.
Results
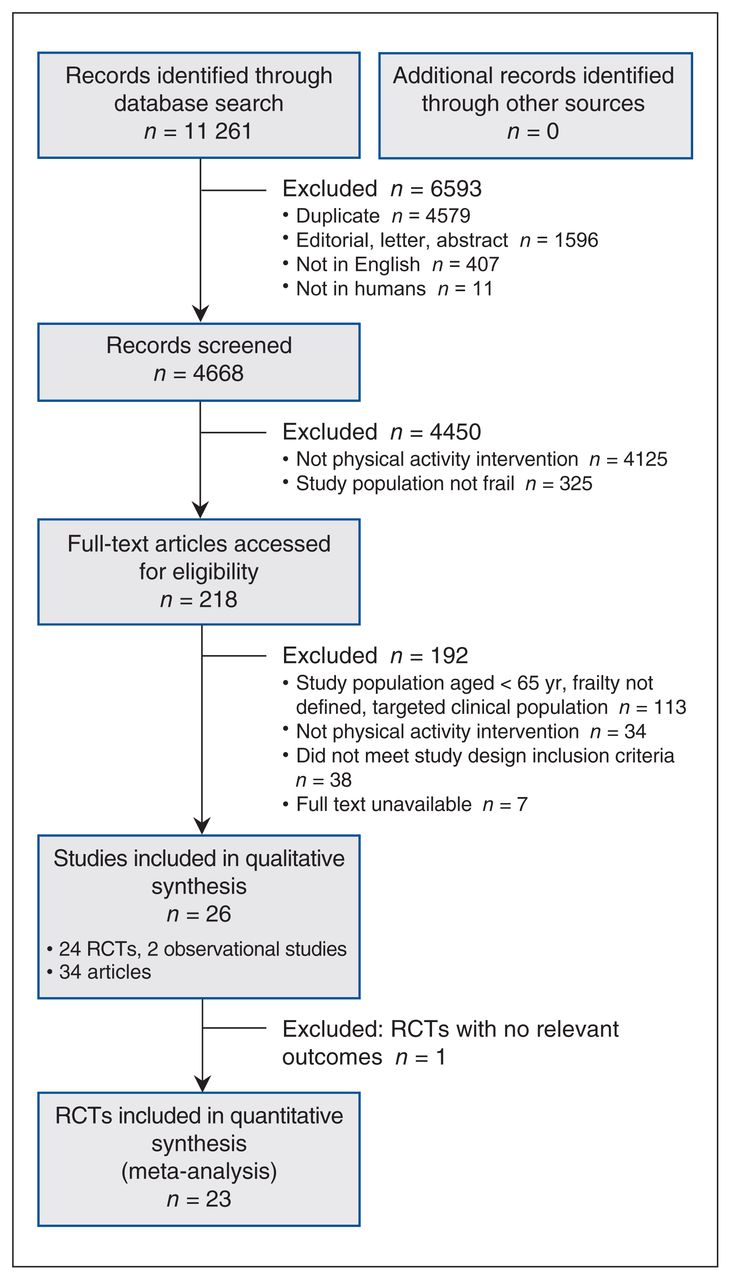
From the 4668 citations identified, we assessed 218 full-text articles for eligibility and included 26 studies described in 34 publications in the qualitative synthesis (Figure 1); the studies were published from 1998 to 2019. Of the 26 studies, 24 were RCTs28–51 and 2 were observational studies;52,53 however, 1 of the RCTs did not have any relevant outcomes for extraction.51 Therefore, we meta-analyzed 23 RCTs and their outcomes.

Flow diagram showing study selection. Note: RCT = randomized controlled trial.
The 26 studies included in the qualitative analysis involved 8022 frail older participants aged 65 years or more (mean 69.8–85.4 yr); the proportion of women ranged from 50% to 100%. All of the included RCTs had fewer than 280 participants (median 88; quartiles 62, 88, 148, 1635), with the exception of 1, which had 1635 participants.30
Characteristics of the included studies are presented in Table 1, and further demographic data from the studies can be found in Appendix 4 (available at www.cmajopen.ca/content/9/3/E728/suppl/DC1). Briefly, interventions were conducted in Asia, Europe and North America (all in the United States) with participants who were community-dwelling or living in care homes (n = 12), or had been admitted to hospital.
Characteristics of the included studies
The tools used to measure and assess frailty included standardized tools such as Fried’s frailty phenotype but also other assessments of mobility, physical dependency and ADL indices. Most interventions (n = 13) consisted of both aerobic and muscle-strengthening activities, known as the mixed (or multicomponent) category, followed by muscle-strengthening activities only (n = 8) (Table 2). The intensity of the interventions was mostly resistance or strength training (n = 9), followed by moderate intensity (n = 7). Activities were performed 1–2 or 3–4 times per week and were 30–60 minutes in duration. The interventions lasted on average 29 weeks, with only 4 studies having a duration of 9 months or more.
Category, intensity, frequency, duration and delivery of included studies
Adverse effects or harms that were directly related to the intervention were reported in 7 studies (5 mixed physical activity,36,43,45,52,53 1 muscle-strengthening intervention31 and 1 mobilization or rehabilitation intervention44), and no occurrences of any adverse effects were reported in 5. Most of the harms consisted of falls (occurring during the intervention protocol or physical activities); fractures, sprains, strains or other injuries; muscle ache and fatigue; and incidents from other pre-existing health problems, such as angina; there was no significant difference between the intervention and control groups. Events were successfully managed with adjustments to intervention protocols in most cases, and participant retention remained high (79%44 to 92%31), but 3 participants withdrew from 2 studies.43,45
Risk of bias and quality of studies
Using the Cochrane Collaboration risk of bias tool, we found that 9 studies had low risk of bias28,36,37,41–44,48,49 and 2 studies had high risk of bias;32,34 the risk of bias was unclear for 13 studies,29–31,33,35,38–40,45–47,50,51 mostly owing to unclear sequence generation, allocation concealment and blinding procedures (Table 3).
Risk of bias for the included studies
The certainty of evidence as assessed with the GRADE approach ranged from very low to moderate; it was moderate for most outcomes owing to downgrading for risk of bias (Table 4; Appendix 5, available at www.cmajopen.ca/content/9/3/E728/suppl/DC1).
Physical activity intervention effect estimates for outcomes and certainty of evidence, for all interventions combined and by intervention category
We did not observe any significant asymmetry across funnel plots for publication bias (Appendix 6, available at www.cmajopen.ca/content/9/3/E728/suppl/DC1).
Benefits of treatment
The meta-analysis included an examination of the between-group impact of all physical activity RCTs together and subgroup analyses based on the intervention category (aerobic [n = 1], muscle-strengthening [n = 8], mobilization or rehabilitation [n = 4] and mixed [n = 13]). Owing to heterogeneity, we analyzed the physical outcomes separately based on the individual measures of ADLs, falls and fatigue level. Forest plots for meta-analyzed outcomes for all interventions and by intervention category can be found in Appendix 7 (available at www.cmajopen.ca/content/9/3/E728/suppl/DC1).
Overall
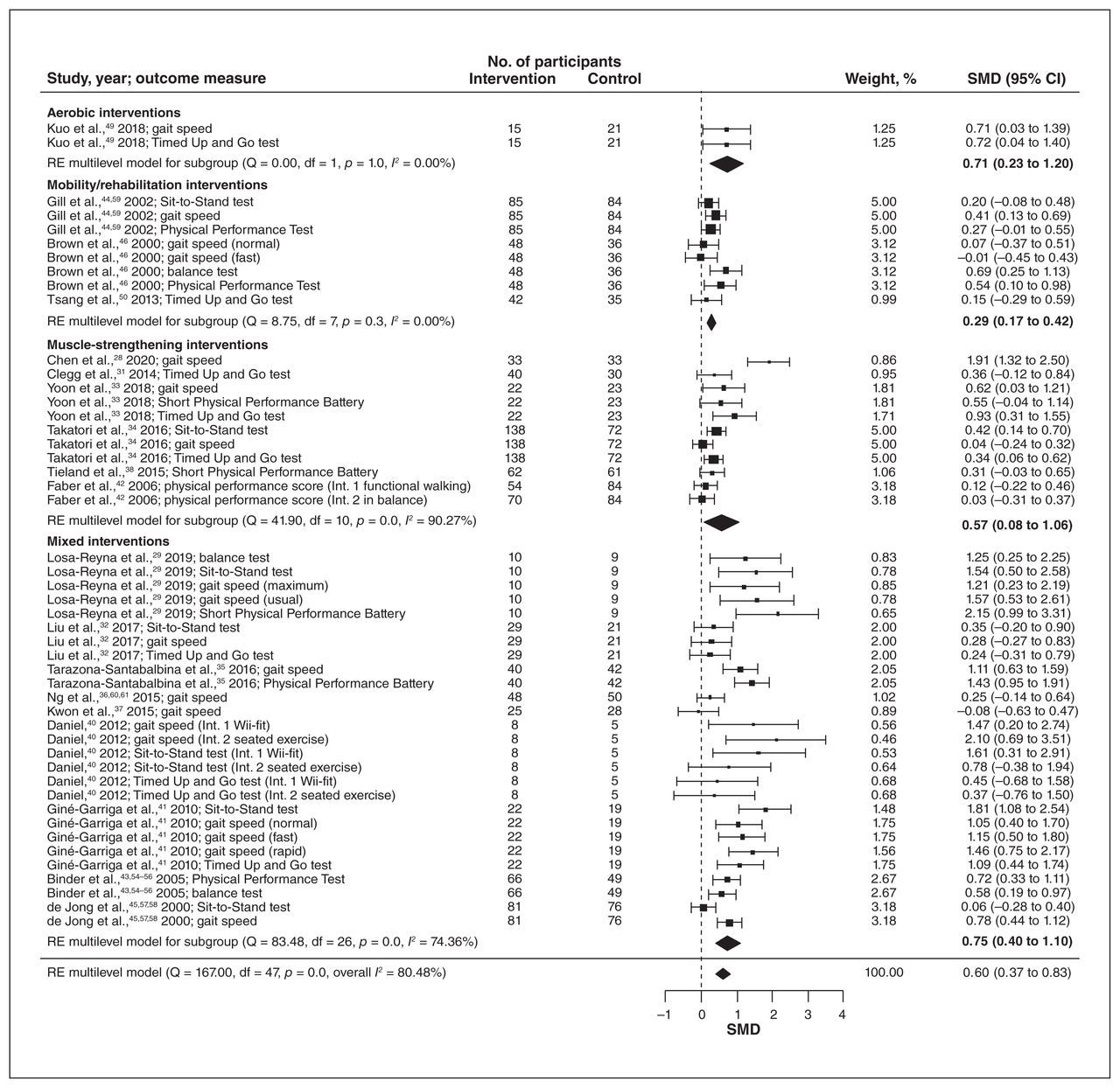
Overall, the RCTs had significant pooled effect estimates on measures of mobility (SMD 0.60, 95% CI 0.37 to 0.83) (Figure 2), ADLs (SMD 0.50, 95% CI 0.15 to 0.84) (Figure 3A), cognitive function (SMD 0.35, 95% CI 0.09 to 0.61) (Figure 3B), quality of life (SMD 0.60, 95% CI 0.13 to 1.07) (Figure 4A) and frailty (SMD −1.29, 95% CI −2.22 to −0.36; RR 0.58, 95% CI 0.36 to 0.93) (Figures 4B and 4C, Table 4; Appendix 7), with moderate certainty of evidence (Appendix 5, Supplemental Table S3). These effects were large for frailty, medium for mobility, ADLs and quality of life, and small for cognitive function. There were no significant effects on measures of falls or fatigue level (Appendix 7).

Effects of overall physical activity interventions on measures of mobility. Weights are from random-effects (RE) multilevel model analysis. Note: CI = confidence interval, df = degrees of freedom, Int. = intervention, SMD = standardized mean difference.

Effects of overall physical activity interventions on measures of activities of daily living (A) and cognitive function (B). Weights are from random-effects (RE) multilevel model analysis. Note: ADL = activity of daily living, CI = confidence interval, df = degrees of freedom, GARS = Groningen Activity Restriction Scale, IADL = Instrumental Activities of Daily Living, Int. = intervention, LLFDI = Late-Life Function and Disability Instrument, LOTCA-G = Loewenstein Occupational Therapy Cognitive Assessment – Geriatric version, MMSE = Mini-Mental State Examination, RBANS = Repeatable Battery for the Assessment of Neuropsychological Status, SMD = standardized mean difference.

Effects of overall physical activity interventions on measures of quality of life (A) and frailty (B [continuous] and C [dichotomous]). Weights are from random-effects (RE) multilevel model analysis. Note: CI = confidence interval, df = degrees of freedom, DL = DerSimonian and Laird, EQ-5D = EuroQol-5 Dimension, RR = risk ratio, SF-36 = 36-Item Short Form Health Survey, SMD = standardized mean difference, SoF = Study of Osteoporotic Fractures criteria for frailty.
Aerobic interventions
The only aerobic intervention, which was a prescribed stepper walking program,49 had a medium but significant effect estimate on mobility (SMD 0.71, 95% CI 0.23 to 1.20) (Table 4; Appendix 7), with low certainty of evidence (Appendix 5, Supplemental Table S4). The mean age of participants was 69.8 years, and 83% were women.
Muscle-strengthening interventions
The muscle-strengthening RCTs had significant pooled effect estimates on measures of mobility (SMD 0.57, 95% CI 0.08 to 1.06) and frailty (RR 0.21, 95% CI 0.10 to 0.43) (Table 4; Appendix 7), with moderate certainty of evidence (Appendix 5, Supplemental Table S5), and a small but significant effect on the measure of cognitive function (SMD 0.45, 95% CI 0.19 to 1.72) (Table 4; Appendix 7), with very low certainty of evidence (Appendix 5, Supplemental Table S5). The mean age of participants ranged from 74 to 85 years; 70% were women.
Mobilization and rehabilitation interventions
One of the 4 mobilization or rehabilitation RCTs did not have any relevant outcomes for extraction.51 The 3 remaining RCTs had small but significant pooled effect estimates on measures of mobility (SMD 0.29, 95% CI 0.17 to 0.42) and ADLs (SMD 0.48, 95% CI 0.28 to 0.67) (Table 4; Appendix 7), with moderate certainty of evidence (Appendix 5, Supplemental Table S6). The mean age of participants ranged from 75.4 to 84.9 years; 70% were women.
Mixed interventions
The RCTs of mixed interventions had significant pooled effect estimates on measures of mobility (SMD 0.75, 95% CI 0.40 to 1.10), ADLs (SMD 0.64, 95% CI 0.004 to 1.27), cognitive function (SMD 0.62, 95% CI 0.12 to 1.11), quality of life (SMD 0.68, 95% CI 0.16 to 1.21) and frailty (SMD −1.57, 95% CI −2.57 to −0.57; RR 0.72, 95% CI 0.63 to 0.83) (Table 4; Appendix 7). These effects were large for frailty, with moderate certainty of evidence; medium for mobility, cognitive function and quality of life, with moderate certainty of evidence; and medium for ADLs, with low certainty of evidence (Appendix 5, Supplemental Table S7). The mean age of participants ranged from 75.9 to 84.1 years; 69% were women.
Both observational studies were prospective cohorts with mixed physical activity.52,53 Only 1 contained data for the outcomes selected in this review.53 Evidence with low certainty indicates that there is a reduced risk of frailty with higher physical activity levels compared to lower physical activity levels (Appendix 8, available at www.cmajopen.ca/content/9/3/E728/suppl/DC1).
Interpretation
Our review showed a significant benefit of physical activity interventions of various types on certain outcomes including mobility, ADLs, cognitive function, quality of life and frailty when compared to control groups in frail adults aged 65 years or more. The effect sizes ranged from small to large, with low to moderate certainty of evidence. When we looked at all physical activity interventions together, there was a large effect on frailty, a medium effect on quality of life, ADLs and mobility, and a small effect on cognitive function.
Previous systematic reviews and meta-analyses have been conducted to evaluate various physical activity interventions and their outcomes related to frailty prevention, progression and reversal, but few have used such an explicit inclusion criterion for prefrailty or frailty, or combined individual measurements of outcomes (such as muscle strength and gait speed) into overall effect estimates (such as physical performance) to allow for a more robust presentation of the results.9–11,62–67 However, frailty itself was measured infrequently, both at baseline and after the intervention. The authors of only 4 of the 23 studies that we meta-analyzed reported frailty outcomes after the intervention, 29,33,35,36 3 of which were mixed physical activity interventions. When compared to control, these interventions showed a large effect size, with moderate certainty of evidence, similar to other reviews;5,63,66,68,69 however, the GRADE approach was not used in any of those reviews, and only 2 included a meta-analysis of outcomes.63,69
Mobility-related outcomes (gait speed, Timed Up and Go test, Sit-to-Stand test, Short Physical Performance Battery, balance test and Physical Performance Test) and ADLs (measured with valid tools such as the Barthel Index, Lawton Instrumental Activities of Daily Living Scale, Instrumental Activities of Daily Living instrument and Groningen Activity Restriction Scale) were significantly improved by almost all physical activity intervention types. Mobility was the most common outcome reported among the studies in our review (19/26). The significant pooled effect estimates were mostly the result of the mixed (n = 9) and muscle-strengthening (n = 6) interventions. Mixed training has been shown to be effective at managing frailty in older adults, with improvements in mobility-related outcomes such as muscle strength and balance, and reductions in disability and falls.15,62,63,66,68,69 Previous reviews have also shown that older adults with frailty can improve mobility and ADL status with progressive resistance-based (muscle-strengthening) training.62,65,68,70–73
We did not compare the effectiveness of different types or categories of physical activity in reducing frailty and frailty-related outcomes in older adults with frailty or prefrailty. Previous reviews also showed that mixed physical activity and muscle-strengthening interventions were the most common types of physical activity investigated in older adults with frailty.9,62,66,74,75 Other types of exercise, such as aerobic or endurance training, balance training, and flexibility or stretching training, have not been studied sufficiently, and their effectiveness has not been established.74 We also did not analyze interventions based on frequency, intensity or duration, as this was not always clearly reported. Previous investigators have also struggled to analyze these data.9,15,65,74,76
Physical activity interventions do not appear to introduce undue harm for older adults with frailty. Several studies reported no occurrences of adverse events, and minor events, such as aches, minor pains and fatigue, were managed successfully through adjustments made to the training protocols. For studies with more severe adverse events (e.g., falls, hospital admission), occurrence rates were similar between intervention and control groups,44 and participant retention in these studies remained high (79%44 to 92%31). Engaging in physical activity comes with inherent risks, but there are also well-known risks associated with sedentary time in older adults.77 Although it is not realistic for all risk of harm to be eliminated during physical interventions, it is important that future studies and clinical and community programs follow published preparticipation screening recommendations to minimize risk to participants.78 Importantly, as was evident from the high level of supervision in the studies in this review, these programs should engage professionals with the requisite skills and knowledge (such as nurses, physiotherapists and kinesiologists) to be able to adjust training protocols for this high-risk population as appropriate.
Research explicitly identifying prefrail and frail older adults, and consistency in the use of frailty identification tools are still lacking. In our review, very few studies measured frailty as a postintervention outcome. Likewise, the wide range of outcome measures used across studies, including unvalidated tools to assess frailty, may reflect the lack of clarity in frailty identification and diagnosis. Well-designed clinical trials that have explicit definitions of frailty and use outcomes that reflect frailty identification and diagnosis are needed to inform clear interventions that prevent or delay frailty progression in older adults.
We identified only 1 study specific to aerobic physical activity, so further research in this area is warranted.
Although the diversity of outcomes reflects the use of physical activity interventions in clinical and real-world settings, 54% of studies did not report the occurrence of adverse events. This limits our knowledge on the safety of the interventions and hampered comparison of studies.
Limitations
We used the inclusion criterion of frailty in an attempt to identify a more homogeneous population. However, it led to a large number of exclusions, which may have resulted in the exclusion of potentially frail populations or those with overlapping conditions. Furthermore, the variety of tools and definitions used to describe participants still made for a diverse population of study participants that was subject to the authors’ interpretation and description. We extracted outcomes immediately after the interventions, which leaves the long-lasting effects of the interventions unknown.
The practicality and uptake of exercises in real-world settings is unknown from this review. Dent and colleagues1 noted that community-based programs for older adults with frailty often fall short of evidence-based recommendations, and that adherence to physical activity programs is poor among older adults for reasons such as fear of falling, lack of self-belief, attitude, and adverse social and environmental influencers. Although we did not observe any significant asymmetry across funnel plots for publication bias, studies were small (< 300 participants) and had risk of bias concerns. Our search protocol had limitations, including restriction to English-language citations, our search end date of July 2019 and the fact that we did not search the grey literature.
Although there may be concerns about the reuse of the same participants from the same study to contribute data for multiple measures of a given outcome, our group agreed that this approach is preferred over selective reporting of effect sizes for a given outcome or averaging outcome measures from the same study to conduct a conventional 2-level meta-analysis. Both selective reporting (i.e., choosing 1 outcome measure for a given outcome) and averaging all outcome measures result in the potential loss and dilution of relevant information, and may produce misleading, inaccurate and biased results. These ad hoc approaches may also lead to missed opportunities to use all available data to address the relevant research questions.79
Conclusion
This review adds to the body of evidence identifying physical activities that benefit components of frailty in older adults, such as mobility, quality of life, cognitive function and ADLs, along with frailty itself. Our use of a strict inclusion criterion that attempted to identify a prefrail or frail population showed that studies need to better define frailty to ensure clear identification of older adults who would benefit from such interventions. This would support the development of clear recommendations and facilitate the adoption and implementation of effective interventions into clinical practice.
Acknowledgement
The authors thank Angela Eady for developing the search strategy.
Footnotes
Competing interests: Jeanette Prorok, Perry Kim, Amanda Lorbergs and John Muscedere are salaried employees of the Canadian Frailty Network. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Megan Racey, Muhammad Usman Ali, Diana Sherifali, Donna Fitzpatrick-Lewis, Leah Gramlich, Heather Keller, Jayna Holroyd-Leduc, Anik Giguère, Ada Tang, Danielle Bouchard, Jeanette Prorok, Perry Kim, Amanda Lorbergs and John Muscedere designed the study. Megan Racey, Muhammad Usman Ali, Diana Sherifali, Donna Fitzpatrick-Lewis, Ruth Lewis and Milos Jovkovic acquired and analyzed the data and drafted the manuscript. Megan Racey, Muhammad Usman Ali, Diana Sherifali and Donna Fitzpatrick-Lewis interpreted the data. Leah Gramlich, Heather Keller, Jayna Holroyd-Leduc, Anik Giguère, Ada Tang, Danielle Bouchard, Jeanette Prorok, Perry Kim, Amanda Lorbergs and John Muscedere revised the manuscript critically for important intellectual content. All of the authors approved the final version to be published and agreed to be accountable for all aspects of the work.
Members of the Canadian Frailty Network: John Muscedere (Scientific Director), Carol Barrie (Executive Director), Perry Kim (Assistant Scientific Director), Amanda Lorbergs (Manager, Research and Knowledge Translation), Jeanette Prorok (Manager, Special Projects and Initiatives), Kyle Plumb (Project Manager), Mat LaBranche (Finance & Administration), Amy Doyle (Manager, Strategic Partnership Development and Communications), Kelsey MacIntosh (Health Promotion Coordinator)
Funding: This research was funded by the McMaster Institute for Research and Aging, the McMaster Evidence Review and Synthesis Team (MERST) and the Canadian Frailty Network (CFN) (Technology Evaluation in the Elderly Network), which is supported by the Government of Canada through the Networks of Centres of Excellence program. The CFN was responsible for the conception of the research question and supported the editing of the manuscript. MERST was independently responsible for data extraction, analysis, interpretation and reporting. Together, these funds supported the work of Megan Racey as a postdoctoral fellow. Diana Sherifali holds the Heather M. Arthur Population Health Research Institute/Hamilton Health Sciences Chair in Interprofessional Health Research, which supported her role in this work.
Disclaimer: No one from the Canadian Frailty Network had any involvement in the data extraction or analysis for the review. All screening of articles, data extraction, and data analysis and interpretation were conducted by the first 6 authors, independent from the steering committee and funders.
Data sharing: Data used in this review can be requested for confidential research purposes by contacting the corresponding author(s).
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/3/E728/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 CMA Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


