


Abstract
Background: Although language concordance between patients and primary care physicians results in better quality of care and health outcomes, little research has explored inequities in travel burden to access primary care people of linguistic minority groups in Canada. We sought to investigate the travel burden of language-concordant primary care among people who speak French but not English (French-only speakers) and the general public in Ottawa, Ontario, and any inequities in access across language groups and neighbourhood ruralities.
Methods: Using a novel computational method, we estimated travel burden to language-concordant primary care for the general population and French-only speakers in Ottawa. We used language and population data from Statistics Canada’s 2016 Census, neighbourhood demographics from the Ottawa Neighbourhood Study, and collected the main practice location and language of primary care physicians from the College of Physicians and Surgeons of Ontario. We measured travel burden using Valhalla, an open-source road-network analysis platform.
Results: We included data from 869 primary care physicians and 916 855 patients. Overall, French-only speakers faced greater travel burdens than the general population to access language-concordant primary care. Median differences in travel burden were statistically significant but small (median difference in drive time 0.61 min, p < 0.001, interquartile range 0.26–1.17 min), but inequities in travel burden between groups were larger among people living in rural neighbourhoods.
Interpretation: French-only speakers in Ottawa face modest — but statistically significant — overall inequities in travel burden when accessing primary care, compared with the general population, and higher inequities in specific neighbourhoods. Our results are of interest to policy-makers and health system planners, and our methods can be replicated and used as comparative benchmarks to quantify access disparities for other services and regions across Canada.
Language-concordant health care — health care delivered in one’s language of choice — is an important element of health care accessibility1 and can improve health care quality and outcomes.2,3 However, members of linguistic minority groups may face barriers to accessing language-concordant health care. In Canada, a multicultural nation with 2 official languages (English and French), residents who speak French but not English (French-only speakers), in particular, may have difficulty accessing French-language services outside of the predominantly French-speaking province of Quebec. Many cities outside of Quebec have sizable French-speaking populations, including Ottawa (40.1%); Timmins, Ontario (52.7%); Moncton, New Brunswick (50.1%); Greater Sudbury, Ontario (39.5%); and Edmundston, New Brunswick (98.3%).4 In Canada, although most elementary- and secondary-school students receive at least some French-language training, the proportion of health care providers outside of Quebec who speak French dropped from 12.3% in 2001 to 11.5% in 2016, and fewer than 20% speak French.5 As a result, French speakers in Canada who live outside of Quebec may face a higher travel burden to obtain language-concordant health care than English speakers,6–8 especially primary care, which accounts for more than 70% of all outpatient physician visits.9 Language barriers for Francophones seeking health care in Canada are associated with misdiagnoses and longer treatment times,10 negative patient11–13 and physician experiences, 14,15 and, in the hospital setting, increased risk of death.3 However, little empirical evidence exists regarding language-based travel inequities to guide health care providers and policy-makers and to inform patients. To address this gap, we sought to develop a geospatial approach to assess access to language-concordant primary care services in Canada’s capital city, Ottawa.
Methods
Study design
We conducted a descriptive cross-sectional geospatial analysis to estimate neighbourhood-level travel times to language-concordant primary care for French-only speakers and the general population in Ottawa. Geospatial analysis has been used to study disparities in health care access across linguistic groups,16 human resource shortages17–19 and links between health care use and patient location.20 Our primary objective was to estimate neighbourhood-level differences in travel burden to language-concordant primary care for French-only speakers and the general population in Ottawa. Our secondary objectives were to investigate the effects of neighbourhood rurality and the proportion of French-only speaking residents on these travel burdens.
Study setting and context
In 2016, using the most recent data available when we conducted our analysis, Ottawa had 916 855 residents,21 of whom 40.1% reported speaking French4 and 1.4% reported speaking only French.22 Ottawa is in the primarily English-speaking province of Ontario and is situated on the border with the primarily French-speaking province of Quebec. Because health insurance is administered provincially and patients can be required to pay out of pocket for inter-provincial care,23 nearly all Ontario residents receive care from Ontario-based physicians. Patients in Ontario are largely responsible for finding their own family physicians, with some assistance from the Ontario Ministry of Health’s Health Care Connect program. 24 Recent estimates suggest that 88.4% of people in Ontario are attached to a primary care physician.25
Data sources and collection
We used public databases, including the College of Physicians and Surgeons of Ontario’s database of registered Ontario physicians, which includes physician names, specialties, practice addresses and languages spoken;26 Statistics Canada’s 2016 Census of Population, which includes residents’ language abilities and was accessed through the Web Data Service;27 Statistics Canada’s 2016 digital cartography files, which provide geographic boundaries for census regions;28 Statistics Canada’s 2016 Geographic Attribute File, which describes residents’ geospatial distributions;29 OpenStreetMap road network data, accessed from the public Geofabrik database (https://download.geofabrik.de/north-america/canada.html); Google’s geocoding application programming interface (API), which we used to convert all physician practice addresses to latitudes and longitudes; and the Ottawa Neighbourhood Study’s digital cartography files, which provide geographic boundaries for 108 neighbourhoods in Ottawa.21,30 We cross-checked data with websites for facilities including hospitals, long-term care homes, retirement homes and the Government of Ontario.
Study population
The study population of physicians included community-based primary care physicians practising in Ontario within a 50-km buffer of Ottawa’s city boundaries. First, we identified all physicians practising within this buffer. Next, we defined community-based primary care physicians as those who met 1 of 2 criteria, namely that their specialty was family medicine and their main practice location was a public-facing primary care practice (e.g., excluding long-term care homes and specialized clinics), or that they reported no specialty, but their practice location was a public-facing primary care practice (e.g., a community-based clinic, a family health team).
Data cleaning included verifying all addresses manually on digital maps. In cases when clinic types were unclear, we reviewed clinic websites and called clinics to confirm. Where possible, we also incorporated local knowledge from the Ottawa Neighbourhood Study’s community partners (e.g., recent retirements, office moves). We assumed that physicians could provide care in languages in which they reported competency. As a final step to reduce computational complexity, we excluded physicians beyond the city of Arnprior, on the western periphery of Ottawa, from our geospatial analysis, since Arnprior already contained 16 family physicians, enough to saturate our analysis.
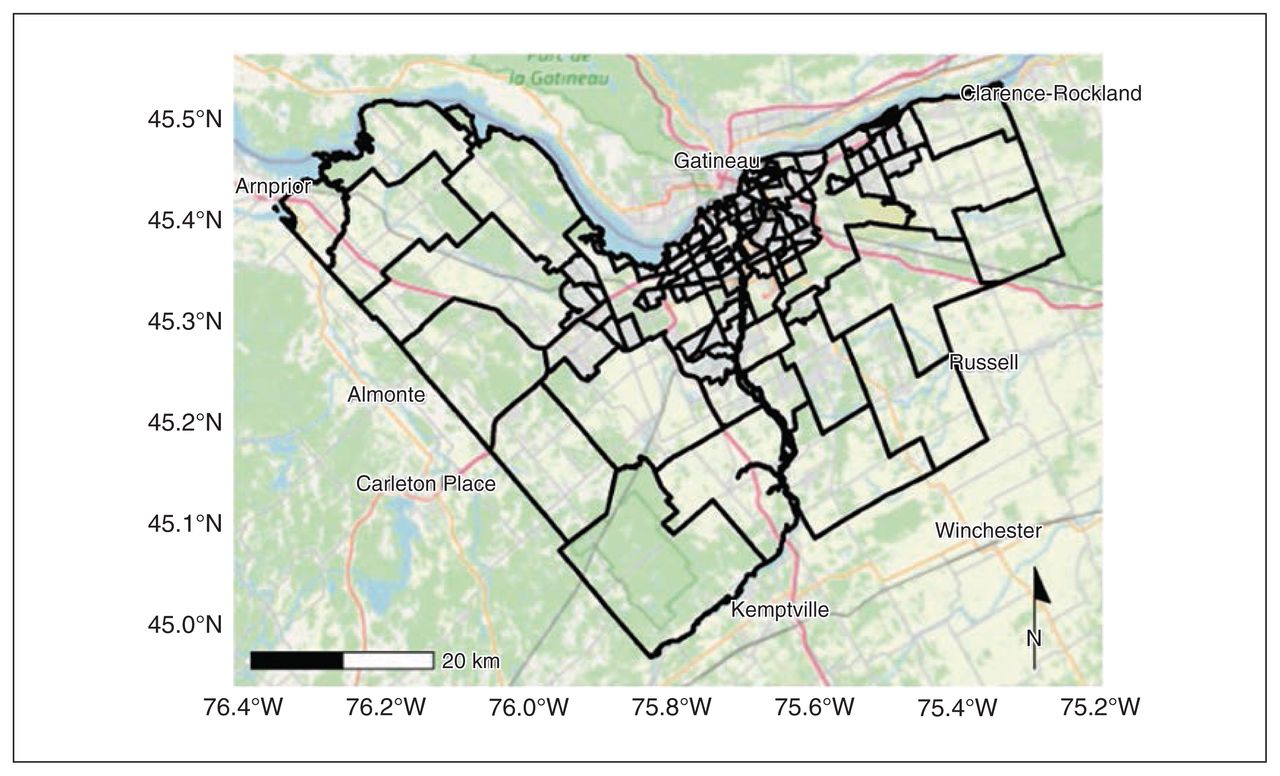
The study population of Ottawa residents included all residents of private households (i.e., excluding institutional settings) within Ottawa’s city boundaries, as identified in Statistics Canada’s 2016 Census of Population. We used population counts for census dissemination blocks, which are the smallest geographic unit Statistics Canada provides and tend to be the size of a city block. To estimate the number of French-only speakers, we used language data available only at the larger level of dissemination areas, which are agglomerations of dissemination blocks comprising roughly 400–700 people. Both dissemination area and block boundaries are set by Statistics Canada and generally align with road networks or surface features like rivers. The Ottawa Neighbourhood Study divides Ottawa into 108 neighbourhoods, which contain 8086 dissemination blocks and 1372 dissemination areas (Figure 1). These neighbourhood boundaries are set through local consultation and are intended to reflect residents’ views of their communities. Statistics Canada and the Ottawa Neighbourhood Study’s boundaries are constructed using different methodologies and align in some but not all cases.
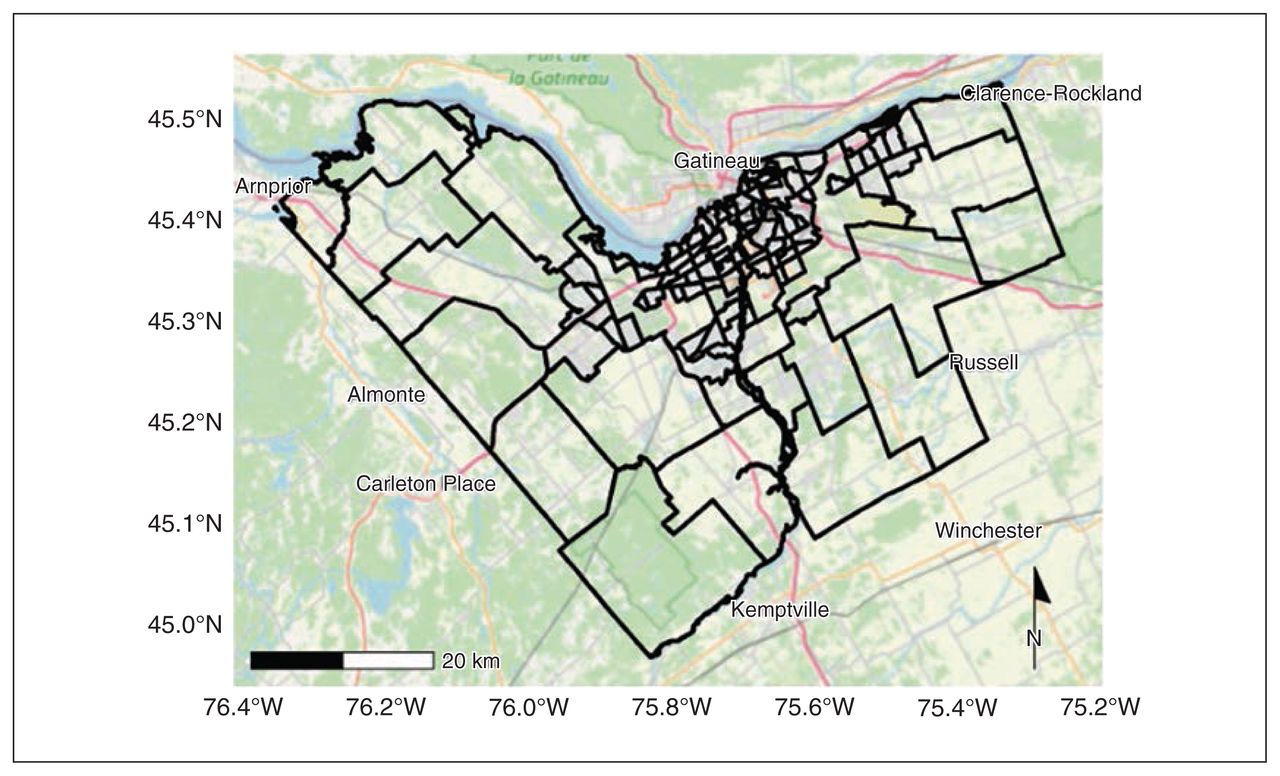
Map of Ottawa, Ontario. Black outlines show Ottawa’s city boundaries and its 108 populated neighbourhoods, as defined by the Ottawa Neighbourhood Study. Map tiles copyright of OpenStreetMap contributors. Contains information licensed under the Open Government Licence – City of Ottawa (https://ottawa.ca/en/city-hall/open-transparent-and-accountable-government/open-data).
Geospatial analysis
Our travel burden analysis used the Valhalla routing engine, an open-source platform for analysis of road networks that provides turn-by-turn directions for several travel modalities, including walking and driving, and respects traffic laws and speed limits.31 We did not consider time of day and traffic. We obtained road network data from OpenStreetMap (https://www.openstreetmap.org/). We conducted all analyses using open-source software, R and RStudio, interfacing with Valhalla through the R package valhallr.
We calculated 2 measures of travel burden, namely travel time by car and, for urban neighbourhoods, walking distance, given that around 14% of workers in Ottawa’s urban neighbourhoods regularly commute by foot.32 We assumed that residents departed from the geographic centre (centroid) of their dissemination block, and simulated driving and walking trips from Ottawa’s dissemination blocks to each physician in our data set. In the absence of recent or official data, research suggests that about 1 in 5 Ontario family physicians are accepting new patients at any point in time,33 so for each travel method, language group and dissemination block, we averaged the travel burden to the 5 closest, language-concordant family physicians. We then aggregated dissemination block–level travel burden into neighbourhood-level burden using population-weighted averaging in an attempt to reflect the lived experience of an average neighbourhood resident.
For the general population, we used unadjusted 2016 census populations, and for French-only speakers, we weighted census populations for dissemination blocks by the dissemination area–level percentage of residents who reported speaking French but not English.34 We linked dissemination blocks to the one populated neighbourhood they overlapped the most. For further details see Appendix 1, available at www.cmajopen.ca/content/11/3/E434/suppl/DC1.
The result is a set of neighbourhood-level, average walking distances and driving times to primary care for the general population to any family physician and for French-only speakers to French-speaking family physicians. For analyses of the impact of rurality on travel burden, we reported driving times and walking distances for all neighbourhoods for completeness, noting that walking will be less common in suburban or rural neighbourhoods. We created a bivariate map to investigate the geospatial relationship between neighbourhood-level driving times to French-speaking family physicians and the percentage of residents who are French-only speakers. Bivariate maps show how 2 variables change across geographies, and have been used to study patterns in cancer rates,35 HIV and hepatitis C rates,36 and respiratory health.37 As is standard for bivariate maps, we grouped both variables into tertiles. Finally, we ran a sensitivity analyses, measuring travel burden from the closest 1 to 10 family physicians, inclusively.
Statistical analysis
We compared within-neighbourhood differences in average travel burden between linguistic groups using the Wilcoxon signed-rank test, a nonparametric test. We calculated differences between the average travel burden to a French-speaking physician and the average distance to any physician, with the null hypothesis that differences in observations have a distribution centred around 0.38 The alternative hypothesis was that the differences between observations are not centred around 0, corresponding to overall greater travel burdens for French-only speakers.
Ethics approval
All data used in in this study were obtained from publicly available sources. Therefore, research ethics board approval was not required for this study.
Results
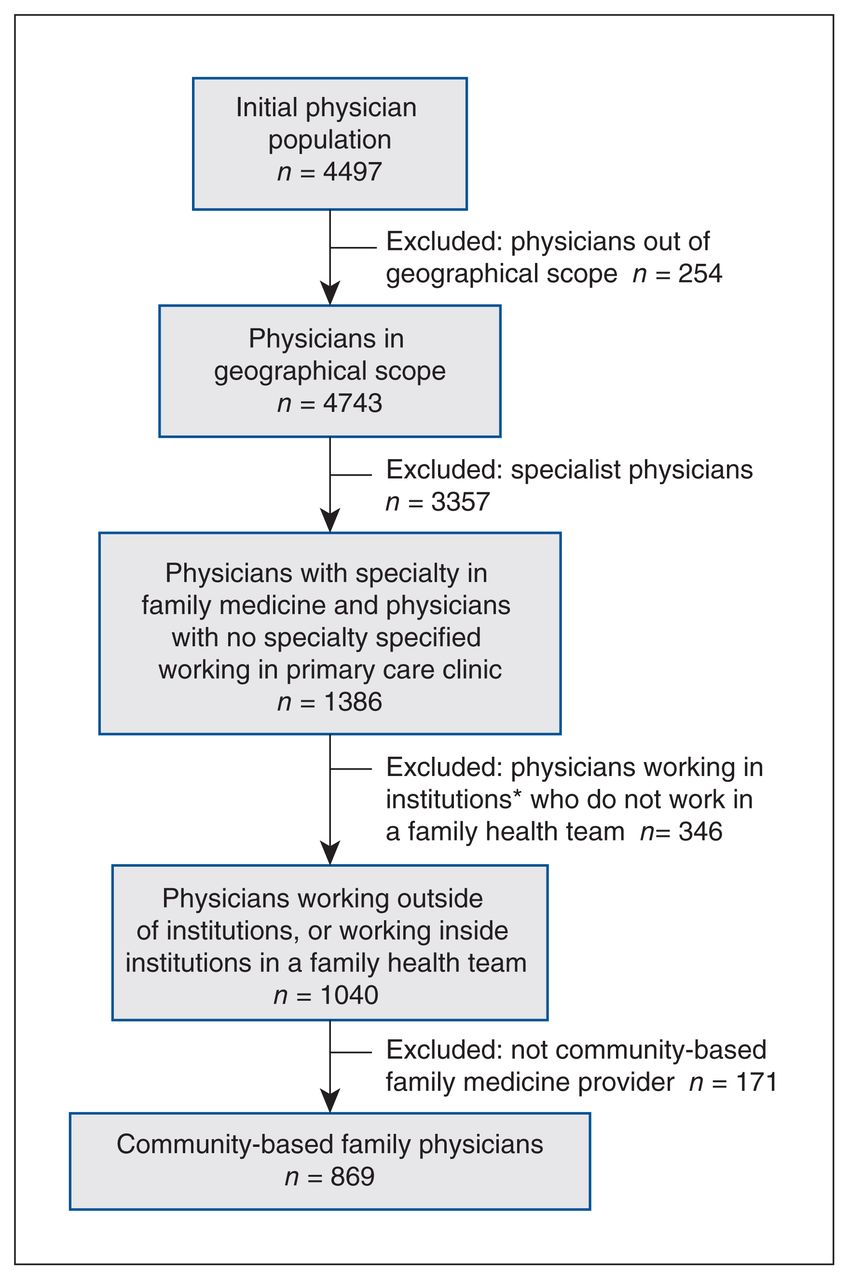
The final population included 869 family physicians who provided primary care in the Ottawa region, of whom all reported competency in English and 356 (41.0%) in French (Figure 2). Neighbourhood-level population characteristics of residents are shown in Table 1. The total number of residents was 916 855, 1.35% of whom were French-only speakers. The median neighbourhood population size was 6983 residents and most neighbourhoods (60.2%) had a proportion of French-only speakers of less than 1%.

Selection criteria for physicians for study inclusion. *Excluded institutions included hospitals, long-term care homes, retirement homes, the Canadian Medical Protective Association and the Canadian Forces Health Services Centre.
Neighbourhood population demographics
Overall inequities in access to language-concordant primary care
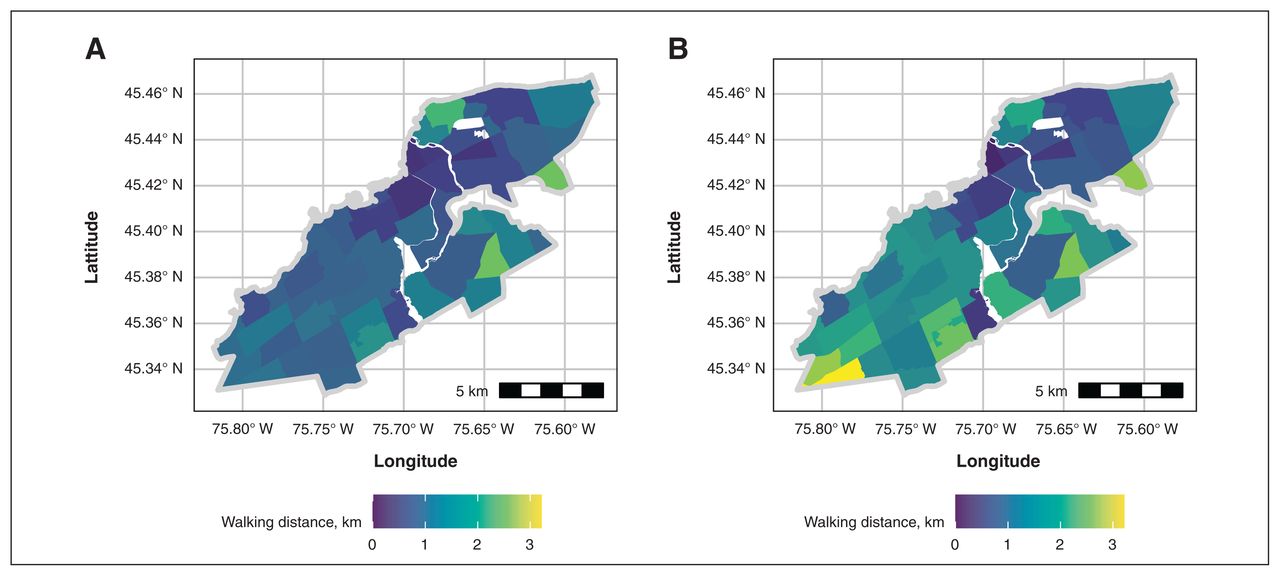
We found evidence that French-only speakers face higher travel barriers overall to accessing language-concordant primary care than the general population (Table 2). These findings were consistent using both driving times (Figure 3) and walking distances (Figure 4), and can be seen clearly when the difference in travel burden is plotted directly (Appendix 2, available at www.cmajopen.ca/content/11/3/E434/suppl/DC1).
Neighbourhood-level travel burden to 5 nearest family physicians for the general population, and to French-speaking family physicians for French-only speakers

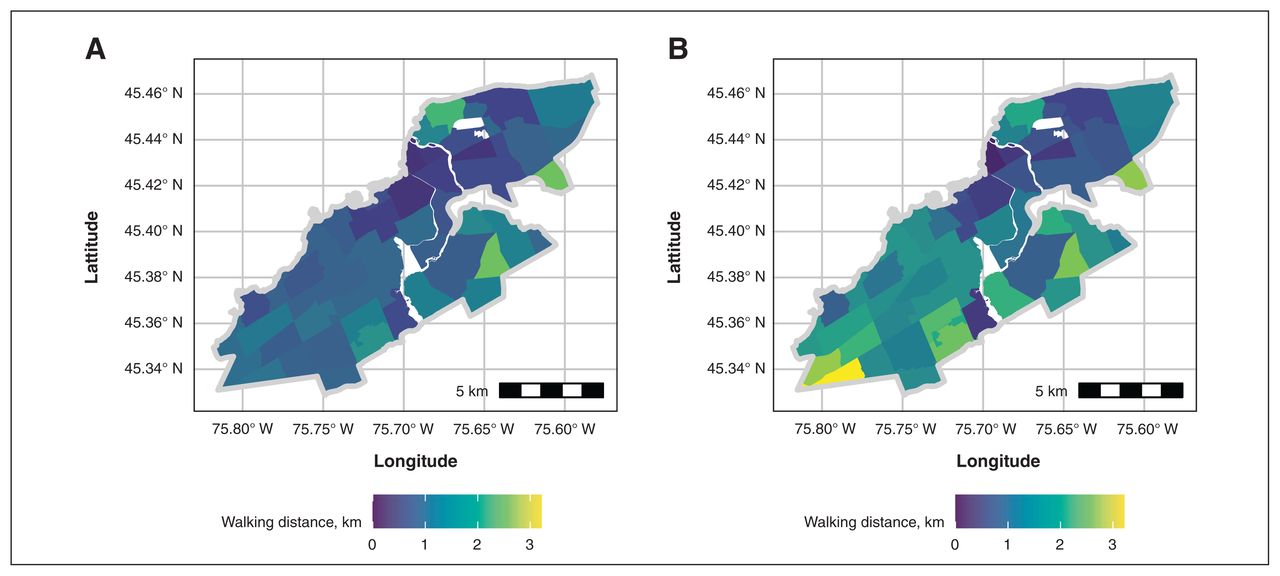
Average neighbourhood-level drive time (A) to any family physician for the general population and (B) to language-concordant family physicians for French-only speakers. Contains information licensed under the Open Government Licence – City of Ottawa (https://ottawa.ca/en/city-hall/open-transparent-and-accountable-government/open-data).
Average neighbourhood-level walking distance (A) to any family physician for the general population and (B) to language-concordant family physicians for French-only speakers in urban neighbourhoods. Contains information licensed under the Open Government Licence – City of Ottawa (https://ottawa.ca/en/city-hall/open-transparent-and-accountable-government/open-data).
Results were statistically significant (p < 0.001), with modest median differences but large interquartile ranges. Some neighbourhoods had lower travel burdens for French-only speakers, compared with the general population. However, several had much higher travel burdens for French-only speakers, including a drive-time difference of 9.3 minutes in the rural neighbourhood of Osgoode-Vernon; even modestly higher burdens may impede residents with mobility restrictions.
The impact of neighbourhood rurality on travel burden
We segmented neighbourhoods by rurality and found that travel burdens increase steadily from urban, to suburban, to rural neighbourhoods, and found statistically significant (p < 0.001) evidence that in each segment, Ottawa’s French-only speakers faced greater travel burdens to language-concordant primary care than the general population (Table 3).
Rurality-stratified neighbourhood-level travel burden to 5 nearest family physicians for the general population, and to French-speaking family physicians for French-only speakers
Relationship between travel burden and language
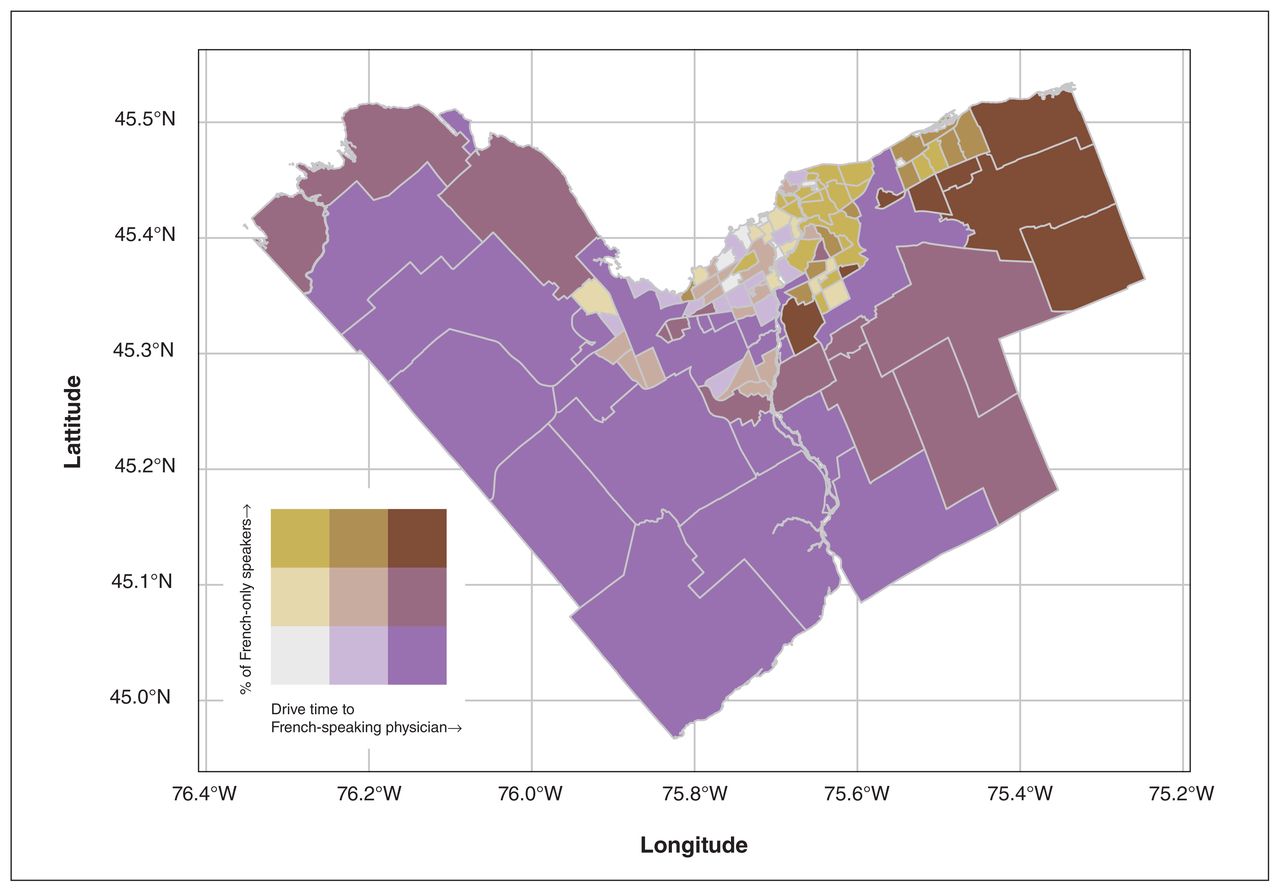
We found that many central neighbourhoods with high proportions of French-only speakers have shorter drive times, suggesting that access may be adequate (Figure 5). Ottawa’s east and northwest regions have both high percentages of French-only speakers and high travel burdens, suggesting that their needs may be unmet. Regions in the south and west had the highest travel burdens but the lowest proportion of French-only speakers.

Bivariate choropleth map showing the neighbourhood-level relationships between the percentage of French-only speakers and average drive time for French-only speakers to a French-speaking family physician. Contains information licensed under the Open Government Licence – City of Ottawa (https://ottawa.ca/en/city-hall/open-transparent-and-accountable-government/open-data).
Sensitivity analysis
In sensitivity analyses, measuring travel burden from the closest 1 to 10 family physicians, inclusively, we found that our overall results were robust. In all cases, we found a median inequity in travel burden for French-only speakers (Figure 6); population-level differences were statistically significant (p < 0.01).

Sensitivity analysis of median difference in (A) driving time and (B) walking distance for the 1 to 10 nearest family physicians (for general population) and the 1 to 10 nearest French-speaking family physicians (for French-only speakers), stratified by neighbourhood rurality.
Interpretation
Overall, French-only speakers in Ottawa face travel burdens that are statistically significantly higher than the general public when accessing primary care. Although the median difference is modest and the number of French-only speakers is small, some individual neighbourhoods face much higher burdens. For example, Ottawa’s northeastern neighbourhoods have a high density of French-only speakers and some of the highest drive times to French-speaking physicians. This suggests that, despite the small median effect, there are geographic pockets of need.
Furthermore, French-only speakers represent a small group within an important proportion of Ottawa residents who report speaking French (40.1% of the Ottawa population); 4 this larger group may also prefer to receive medical services in French, and research has found that Francophones may be less satisfied or have worse outcomes if required to receive services in English.11–13 Our findings, therefore, identify a care gap and inequities that may be relevant to a much larger segment of the population.
Our study differs from similar studies in 2 ways. We used no-cost, open-source software, R and Valhalla. Other studies generally use expensive commercial geospatial analysis software like ArcGIS and statistical software like SPSS.16,17 We computed time and distance burdens directly rather than use accessibility indices.16,17 We believe our methods complement existing approaches with an intuitive measure of travel burden easily understood by patients and policy-makers alike.
Our methods could be extended to study other regions and health care services to identify population-level access inequities, and updated to include new data from the recent 2021 Statistics Canada Census as it becomes available. Measuring travel burden as driving time and walking distance make our methods applicable for measuring inequities in urban, suburban and rural areas. We plan to validate our approach against standard commercial tools. Our method could also be extended to include travel by public transit. Future research could also systematically incorporate local knowledge and input from community partners. The use and prevalence of interpreters within primary care settings could also be explored. Lastly, we have developed a public-facing interactive online map of family physicians that can be filtered by language spoken. An English version is available at https://www.docmapper.ca/, and a French version at https://www.trouvezunmedecin.ca/. There is great interest in this tool, and we are currently preparing a user satisfaction survey.
Limitations
Our finding that 17.4% of Ottawa’s physicians practise family medicine is lower than some province-wide estimates, which can be as high as 46.3%.31 However, Ottawa is a regional medical hub that is home to large hospitals and specialty clinics, which will reduce the proportion of family physicians; in addition, we looked specifically at providers whose primary practice location provides primary care service to the public. Measuring travel to the 5 nearest physicians is evidence-based and our overall results were supported in sensitivity analyses, but our results depend on our classification of family physicians. We cannot know which physicians were accepting new patients or if this varied across language groups, and this proxy measure may have underestimated true travel burden. We used the most recent Census data available, from 2016, when we began our analysis, but population demographics may have changed. Some clinics may have French-speaking allied health care professionals who could provide language-concordant care. Our 2 study populations are not mutually exclusive since French-only speakers were included in the general population; however, they represent a small percentage of the population so we expect any error to be minimal. Our study does not include public transit, and it is uncertain how many patients use public transit to access health care or how this variable may affect travel times. Some non-English speakers have been included in the general population. Finally, we cannot account for Ottawa residents receiving cross-border care in Quebec, although financial burdens24 and anecdotal reports suggest that few regularly do so.
Conclusion
We found evidence that, overall, Ottawa’s French-only speakers face a modest but statistically significant travel burden to accessing primary care, compared with the general population, and that this burden increases with neighbourhood rurality. Our approach combined public data with open-source software to calculate neighbourhood-level travel burden in terms of time and distance using the Valhalla routing software and population weighting. Our results and methods can inform health system planning and may be of interest to patients, physicians and policy-makers, and our methods can be generalized to study access to different services in other regions.
Acknowledgement:
Lise Bjerre thanks the Ontario SPOR Support Unit Francophone Initiative (IF-COFFRE) for its ongoing support of her program of research.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Lise Bjerre conceived and designed the work. All of the authors contributed to the acquisition, analysis and interpretation of data. Chris Belanger drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding was provided by the Ontario SPOR SUPPORT Unit, which is supported by the Canadian Institutes of Health Research, the Province of Ontario and partner Ontario hospital foundations and institutes. This project was funded by an unrestricted grant to Lise Bjerre by the Ontario SPOR Support Unit Francophone Initiative (IF-COFFRE). Lise Bjerre holds the inaugural University of Ottawa and Institut du Savoir Montfort Chair in Family Medicine.
Data sharing: The data and R code used in this analysis are available from https://github.com/Belanger-Analytics/ottawa_franco_physician_access_study. Map data are copyrighted by OpenStreetMap contributors, available under the Open Database License, and available from https://www.openstreetmap.org.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/3/E434/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.