


Abstract
Background: The advanced access model was developed 20 years ago and has been implemented in several countries. We aimed to revise and operationalize the pillars and subpillars of the advanced access model based on its contemporary practice by professionals in primary health care.
Methods: This multimethod sequential study was informed by a literature review and an expert panel of provincial and local decision-makers, primary health care clinic members (family physicians, nurses and administrative staff), patients and researchers from the province of Quebec. Throughout the consultation process, participants were asked to develop a common vision of the pillars and subpillars that make up the advanced access model and to react to suggested definitions or content.
Results: The revised advanced access model is defined by 5 pillars, of which 2 were updated from the original model (“Appointment system” and “Interprofessional practice”), 1 was merged with a revised pillar (“Develop contingency plans” with “Planning of needs and supply”) and 1 underwent major transformations (“Backlog reduction” to “Continuous adjustment”). A new pillar concerning communication emerged from the consultation process. Subsequent steps for operationalizing definitions of subpillars confirmed the nature of the revised advanced access pillars and stabilized their content.
Interpretation: The overall consultation process resulted in a revised contemporary advanced access model, with strong consensus among participating experts. The revised model will be used to develop a reflective tool for primary health care professionals to evaluate their advanced access practice.
Timely access is a cornerstone of strong primary health care and a key component of a patient-centred medical home for ensuring population health.1 Numerous innovations have been implemented to improve timely access,2 with one of the most recommended around the world being the advanced access model, also called open access.2,3 Based on greater accessibility linked with patients’ relational and informational continuity with a primary health care professional or team, the advanced access model aims to ensure that patients obtain access to health care services at a time and date convenient for them when needed, regardless of the urgency of the demand.4 Originally developed in the United States in the early 2000s, advanced access is defined by Murray and Berwick as having 5 pillars: balance supply and demand, reduce the backlog of previously scheduled appointments, review the appointment system, integrate interprofessional practice and develop contingency plans.5,6 Several scientific papers on the foundations of advanced access have been published over the past 20 years, and its benefits have been reported in many countries, including the US, the United Kingdom and Canada.6–9
Over the last 2 decades, primary health care practice has evolved to increase interdisciplinarity in clinical teams. Thus, the need for a model that incorporates new practices and professionals has necessitated development of an updated advanced access model. Furthermore, advanced access was originally developed in a context that prioritized implementing a new way of doing, with less emphasis on the ongoing practice and sustainability of the model.10,11 However, changes in primary health care practice require revisions to the advanced access model to adapt it to the contemporary context.
In this study, we redefine the pillars and subpillars of the advanced access model by integrating an interdisciplinary team–based focus, while considering the integration of primary health care professionals, such as nurse practitioners, registered nurses, social workers and other allied professionals, in primary health care practices. The objective of this study was to revise and operationalize the pillars and subpillars of the advanced access model.
Methods
This study was based on a sequential multimethod consultation process12 informed by a literature synthesis and a 3-phase consultation with advanced access experts: a deliberative face-to-face meeting, an e-survey and 2 final virtual validation meetings.
Literature synthesis
We searched for terms such as “advanced access,” “open access,” “same-day scheduling,” “timely access” and “AA implementation” in MEDLINE, CINAHL, HealthSTAR and PsycInfo for scientific peer-reviewed studies published between 2001 and 2019 (Appendix 1, available at www.cmajopen.ca/content/10/3/E799/suppl/DC1). Grey literature, such as reports or implementation guides, was also identified. English and French publications were considered. Two analysts independently screened titles and abstracts, then full publications of retrieved references. Disagreements were resolved by discussion. The research team used an inductive approach to analyze the literature and identify concepts that emerged from past use of advanced access in primary health care practices (e.g., need for regular adjustment, integration of new appointments and consultation modalities, continuity, communication and satisfaction). Concepts were integrated to delineate pillars and subpillars defined across models of advanced access developed over time.
Consultation with advanced access experts
In November 2019, we identified a variety of key stakeholders suggested to be advanced access leaders in Quebec. Provincial and regional decision-makers, family physicians, nurse practitioners, registered nurses, quality improvement coaches, administrative staff and patients were invited by email to join the research team as part of an expert panel. To be considered an expert, participants needed to be involved with an organization working closely with primary health care professionals, speak French and have extensive experience with advanced access (≥ 5 yr). A list of experts was shared with key informants, and purposive and snowballing techniques were used to complete the list. Patients from a patient-partner group developed as part of an interprofessional advanced access quality improvement study were also involved as stakeholders in the consultation.11 Forty-five advanced access experts were invited to join the expert panel, with the aim of recruiting and maintaining 20 to 25 experts throughout the consultation to ensure diverse representation of participants bringing different perspectives of advanced access principles.
Deliberative face-to-face meeting
Experts representing all categories of stakeholders participated in the deliberative face-to-face meeting (phase 1). We purposely selected the World Café method, a creative process that aims to facilitate constructive dialogue and sharing of knowledge and ideas in a cafe-style setting,13,14 to allow each participant to question the current relevance of all advanced access pillars in contemporary primary health care practice and to suggest new pillars. Groups of 5 or 6 experts were invited to sequentially debate and discuss each suggested pillar that emerged from the literature, identify disruptive or missing elements, suggest changes to the nature of the pillars and propose changes to operational definitions. A “table host” stayed to welcome subsequent groups, briefly recounted results of previous rounds and shared conversation results with the larger group at the end. Building on the World Café results, a “carousel” technique was used with advanced access experts to brainstorm essential components of the definition of each pillar within primary health care practice. The carousel technique allows participants to move sequentially around a room, stopping to comment and discuss topics or themes with the help of a facilitator.15 The results of this meeting, based on observations and summaries of present research team members, were analyzed using an inductive approach16 to reach consensus on a conceptual model of advanced access, including preliminary names and definitions for each identified pillar. After the face-to-face meeting, experts present were asked to suggest people directly involved in an advanced access practice who should be part of the second consultation phase.
Electronic survey
In phase 2, subpillar names and operational definitions were submitted via an e-survey consultation17–19 to invited advanced access experts.20 Only experts with concrete experience in advanced access implementation and improvement were considered for this phase. A descriptive analysis of relevant content from the literature and from phase 121 led to the development of a questionnaire available on Survey Monkey for the e-consultation (Appendix 2, available at www.cmajopen.ca/content/10/3/E799/suppl/DC1).
In this questionnaire, participants were asked to rank subpillar structure and hierarchy (on a scale of 1 to 9); comment on definitions, if applicable, or provide their own; and propose subpillars they felt were missing, along with a definition. Consensus on the relevance of a subpillar was considered obtained when 75% or more of responses were in the high agreement zone (6 to 9), with a median in the high zone and an interquartile range of 0 or 1. Subpillars not meeting these levels of consensus were kept for further reflection or clarification in the last phase.
Validation meetings
In phase 3, final meetings in March 2021 allowed for finalization of operational definitions of pillars and subpillars and consolidation of the revised advanced access model. Experts were invited to validate the content and definitions of subpillars in an e-carousel activity, with one virtual room available for discussing each pillar. This exercise was also performed with patients in an open discussion paying special attention to patient experiences. Both meetings were held virtually and allowed everyone to participate through an open discussion.
The study was conducted in French and professionally translated.
Ethics approval
This study was approved by the Scientific Research Committee (an independent committee working along with the research ethics board under the umbrella of the Centre intégré de santé et de services sociaux de la Montérégie-Centre), and ethics approval was provided by the research ethics board of the Centre intégré de santé et de services sociaux de la Montérégie-Centre (2020–441, CP 980475).
Results
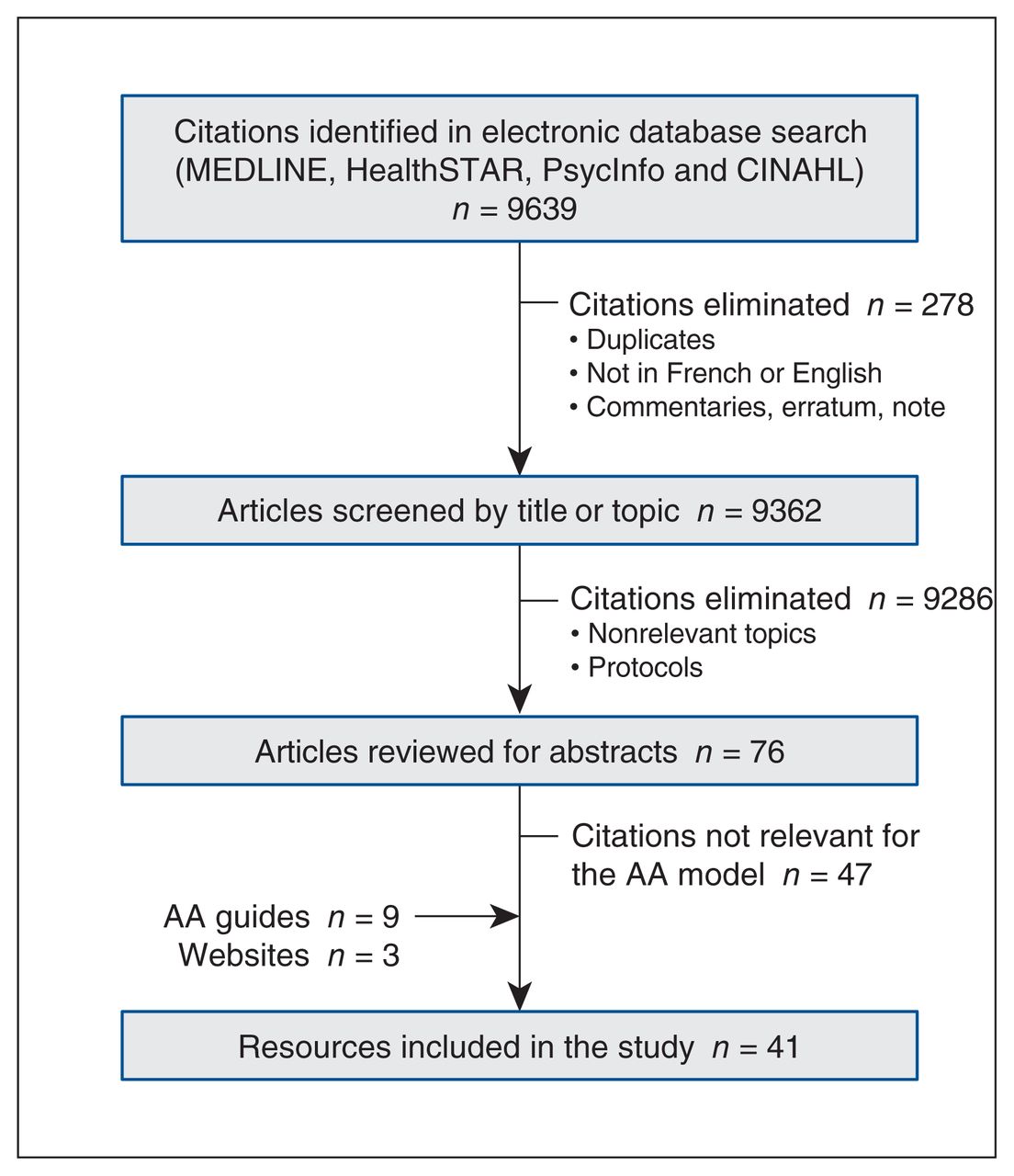
We identified 9639 citations in the electronic database search. After elimination of duplicates, 9362 titles were screened, 76 abstracts were reviewed and 41 resources were retained for inclusion in the study (Figure 1). Forty-five experts participated in at least 1 consultation phase, and 17 experts participated in them all (Figure 2). Characteristics of the expert panel are shown in Table 1. Although the expert panel was heterogeneous in composition, representing different roles in primary health care, no polarization by expert role or group was observed. More specifically, 56% of subpillars were evaluated as highly relevant by all experts in phase 2, illustrating a high level of consensus among the experts consulted. As the subpillar “Preparing for the appointment — efficiency” showed an interquartile range of 2, this subpillar received special attention in the subsequent e-survey consultation and in meetings with the expert panel and patients. Refocusing its operational definition and eliminating the element of efficiency was satisfactory for all and led to consensus on its relevance.
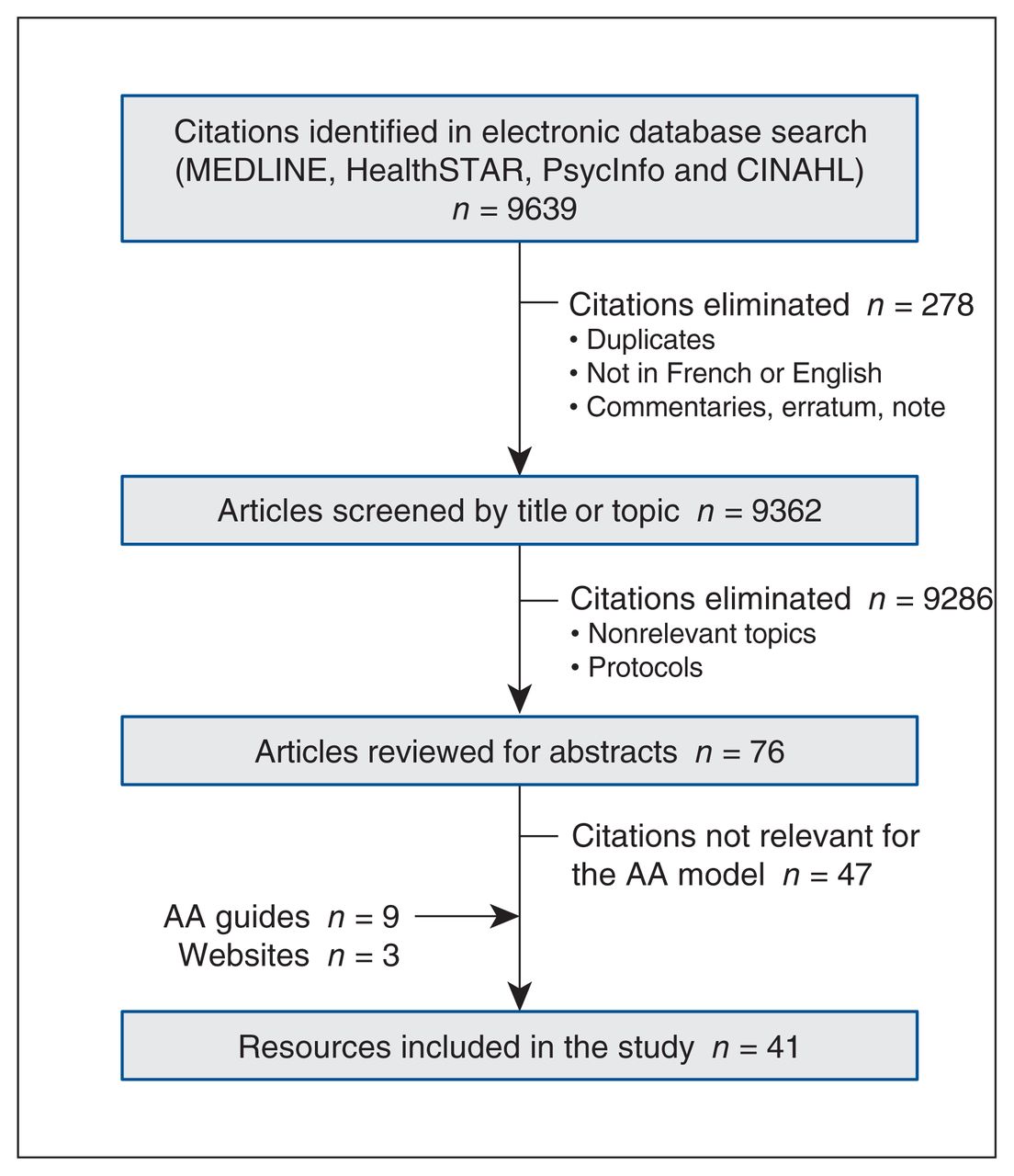
Flow diagram of resources selection. Note: AA = advanced access.

Phases of the sequential multimethod consultation. Note: AA = advanced access.
Demographic characteristics of the advanced access expert panel in the consultation phases
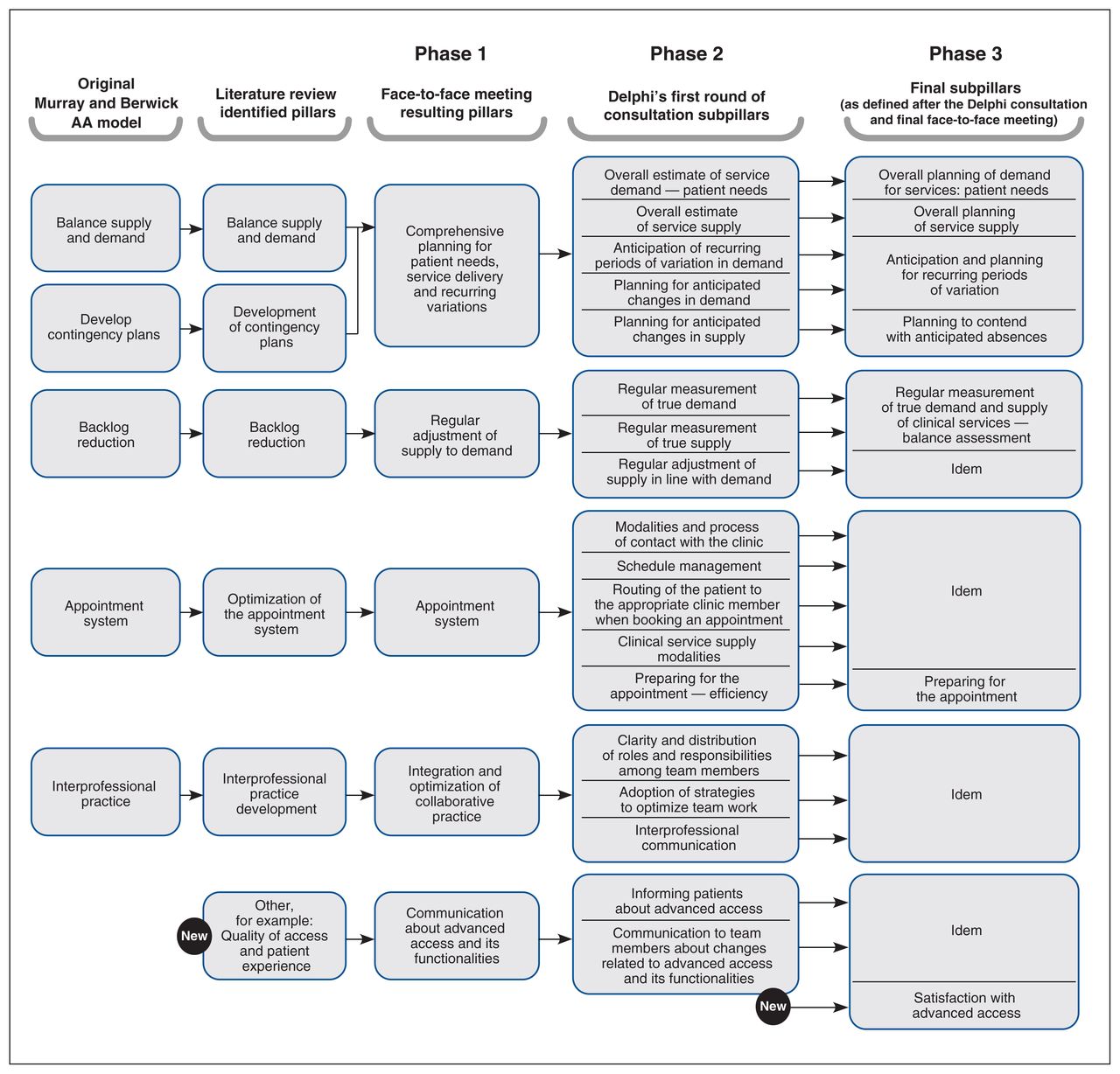
Figure 3 shows how the pillars and subpillars of the advanced access model evolved from the original model through all consultation phases. Modifications that emerged from consultations added clarification to pillars and subpillars, allowing for refinement of operational definitions as well as the revised overall advanced access model.

Evolution of the advanced access (AA) model through expert consultation — pillars and subpillars. Each arrow represents the modification performed between phases or subphases. Converging arrows indicate that a concept was combined with a pre-existing pillar, and “new” indicates the introduction of a new element at one of the consultation phases.
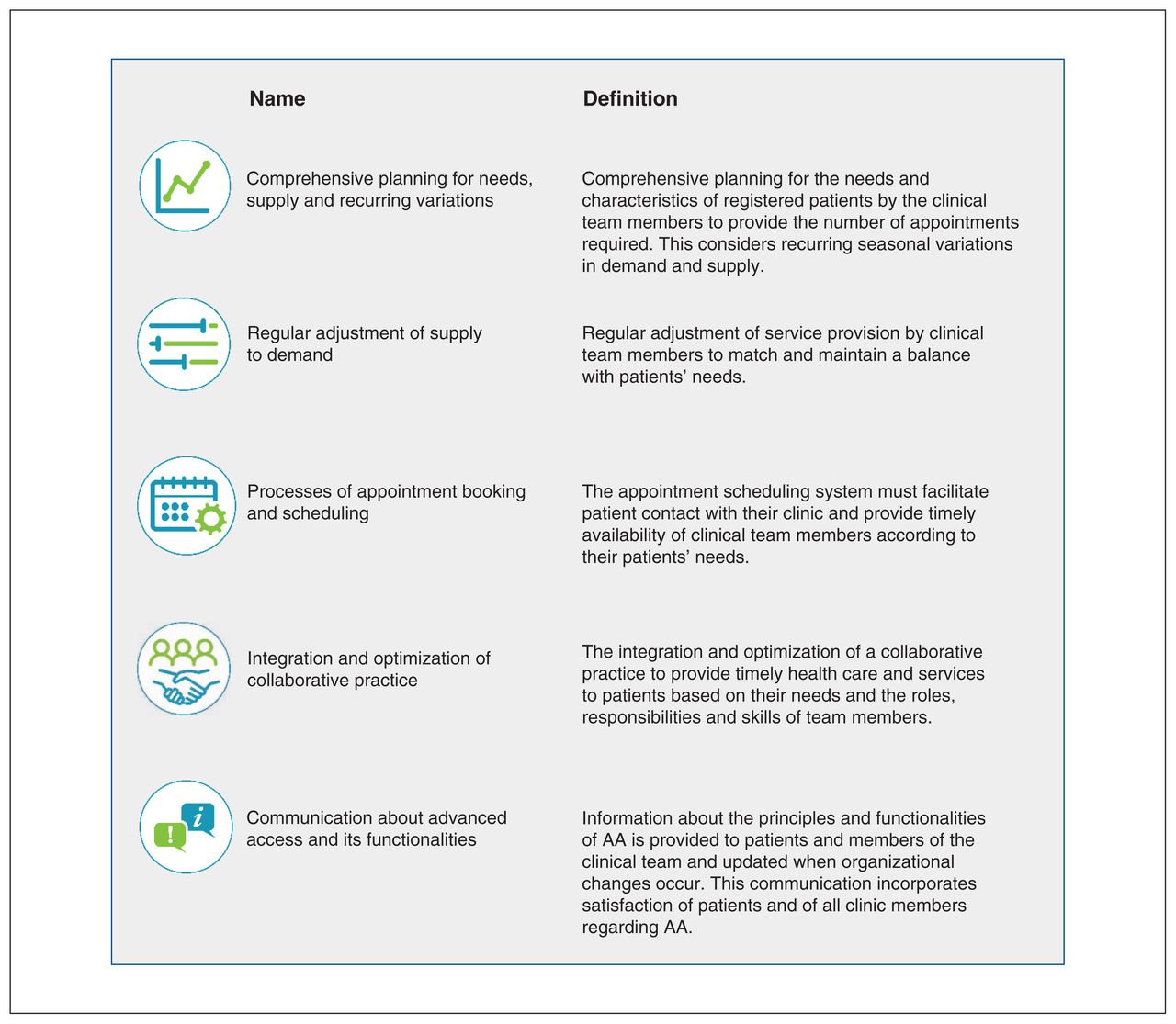
Figure 4 presents indicators used to evaluate consensus among the 25 advanced access experts who participated in the e-survey (phase 2) on the relevance of each subpillar on a scale of 1 to 9. Figure 5 presents the final consensual advanced access model pillars and their operational definitions. The overall consensus process resulted in a revised advanced access model with 5 pillars and 17 subpillars, with each subpillar representing a key individual element of the operational definition of advanced access. In the revised model, 4 pillars underwent minor to major changes (“Comprehensive planning for needs, supply and recurring variations,” “Regular adjustment of supply to demand,” “Process of appointment booking and scheduling” and “Integration and optimization of collaborative practice”), and 1 was merged with an existing pillar (now called “Comprehensive planning for needs, supply and recurring variations”). A new pillar emerged from the consultation and was added to the model (“Communication about advanced access and its functionalities”).

Indicators of consensus on the relevance of subpillars in the e-survey (n = 25). Note: All median values being 9, median values are not presented in the table. Only response choices that were used by at least 1 respondent are presented.
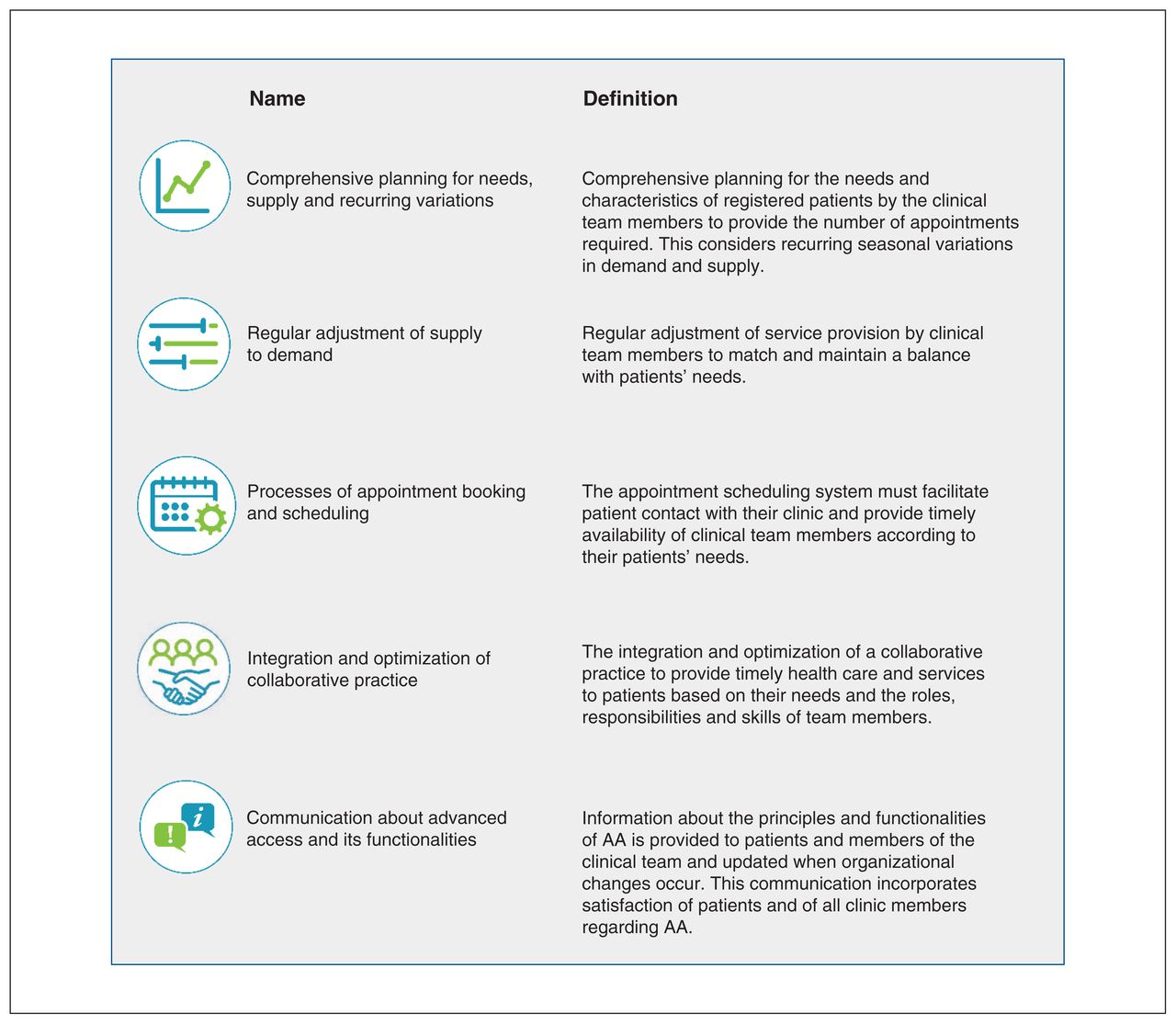
Final 5 pillars of advanced access (AA) and their operational definitions.
Of the 5 pillars of the suggested advanced access model, patients suggested substantial changes to pillars 4 and 5. Interprofessional collaboration and mental health were identified as important themes. Bidirectional and open communication between clinic and patient was also perceived as essential to allow patients to engage in their care. In addition, close monitoring of the interplay between accessibility and continuity of care was deemed crucial in the revised advanced access model. For example, participating patients mentioned that they prefer to wait longer, when appropriate, to meet their own health care provider.
Interpretation
Over the last decade, the advanced access model has been endorsed by several medical associations across Canada, including The College of Family Physicians of Canada.4 Many providers that have implemented advanced access in their organizations and practices expressed the need to better understand the advanced access model as adapted in their practice. This study aimed to revise the 20-year-old advanced access model by identifying key contemporary pillars to guide primary health care providers, practices and organizations in the continuous improvement of their practice. Here, we propose a substantially modified advanced access model developed through a rigorous consultation process. The advanced access experts involved agreed that initial pillars 1 (“Balance supply and demand”) and 2 (“Develop contingency plans”) represented elements of overall planning as defined in “Comprehensive planning for needs, supply and recurring variations.” Thus, these initial pillars were merged into a new pillar with the overall objective of achieving and maintaining balance between available appointments and demand for consultations. Considering a long-term vision for advanced access, the initial pillar “Backlog reduction” evolved into “Regular adjustment of supply to demand,” which includes maintaining a balance between patient demand and service supply of the clinic or professional, a concept that was poorly addressed in the original model. Indeed, maintaining balance is key to an advanced access practice.19–21 This expanded pillar still aims to reduce backlogs but now includes maintaining gains and preventing the return of backlogs. A new pillar, “Communication about advanced access and its functionalities,” emerged as a major principle central to implementation, and moreover sustainability, of advanced access. Finally, the growing trend toward offering multiple appointment modalities was perceived as necessary by the experts, especially in the context of the COVID-19 pandemic.
The involvement of advanced access experts from different backgrounds and health professions ensured that the model reflected the current context of primary health care practice and was not restricted to a family physician perspective. Considerations such as the importance of involving not only primary health care professionals, but also managers, decision-makers and patients helped redefine the pillar “Integration and optimization of collaborative practice,” making it more inclusive and extending advanced access practice to all clinic professionals, an important contribution of this study. Additional attention is now given to the importance of professional and patient satisfaction with advanced access, in line with 2 of the Quadruple Aim goals.22
Patient-partners were key stakeholders in the consultation process. They emphasized the importance of specific elements key to the patient access experience, such as the overall access journey and the desired balance between accessibility and continuity. Indeed, accessibility starts when the patient needs to contact the clinic for an appointment. Getting an appointment in a timely manner means being able to contact the clinic easily and efficiently in a way that is convenient for the patient. This was raised by all types of participating experts but particularly by patients, for whom this step may represent a substantial barrier to accessing clinic services.
Continuity was deemed as important as accessibility by patients, depending on the urgency of their need. Although continuity is not an intuitive element of an access model, several scholars interested in advanced access23,24 underline its importance in patient management as well as in limiting demand for appointments and contributing to better overall quality of care.23 Indeed, a patient who meets with their usual professional, with whom a relationship of trust has developed over time, is less likely to make another confirmation appointment. 24 Thus, at the end of our consultation process, this concept was an integral aspect of referring patients to the appropriate professional. Patients emphasized the importance of relational continuity and said they would prefer to wait for an appointment with a known professional, especially those dealing with complex needs.25 By increasing timely access to patients’ own providers, advanced access improves relational continuity as a consequence of increased availability of the professional while avoiding the need to consult another professional or visit another setting to access timely care.26
The overall consultation process involved multiple methods that provided experts the opportunity to express themselves in various ways and at different times throughout the iterative process. Confirmation of various aspects of the model by patients and the addition of important elements specific to the patient experience also represent important additions to the original advanced access model.
Limitations
There were limitations to this study. The entire consultation process took place in a very supportive organizational and political context for advanced access, potentially limiting the generalizability of our findings. Indeed, the experts consulted are early promotors or adopters of advanced access and are convinced of the benefits of an advanced access practice. Advanced access practice is also actively promoted by Quebec’s Ministry of Health and Social Services as a model for improving access not only to family physicians but to all professionals in primary health care clinics. The literature search was limited to English and French, which may have excluded some resources or perspectives from our attention. Although many members of our expert panel work in bilingual environments and are fluent in English, they were required to speak French to be included in the consultation. However, we are confident that the model applies to other primary health care contexts, as it is based on general concepts central to primary health care practice.
Conclusion
This study led to a revised advanced access model based on consensus among advanced access experts representing diverse stakeholder types, including patients. This new model and the development of operational definitions expand the original model to professionals other than physicians and nurses working in primary health care. The final consensus definitions are measurable and represent levers for actionable changes that can lead to an optimal advanced access practice. This model is an essential step in supporting both individual and collective reflection on advanced access practice and will guide the development of a reflective tool to support professionals working in primary health care. This redesign of the advanced access model integrating a contemporary perspective of primary health care offers opportunities to support primary health care professionals who have either already implemented advanced access or are willing to do so and to ensure its sustainability.
Footnotes
Competing interests: Isabelle Gaboury reports funding to her institution from the Ministry of Health and Social Services. No other competing interests declared.
This article has been peer reviewed.
Contributors: Mylaine Breton and Isabelle Gaboury led the conceptualization and design of the study, but all authors were involved. Mylaine Breton, Isabelle Gaboury and Christine Beaulieu wrote the first draft, and Maxime Sasseville, Catherine Hudon, Sabina Abou Malham, Isabel Rodrigues, Lara Maillet, Arnaud Duhoux and Jeannie Haggerty critically reviewed it and provided comments to improve the first draft and the revised version of the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was supported by a 2-year grant from the Ministry of Health and Social Services of Quebec for $500 000. The funding organization was not involved in the design of the study or the writing of the protocol (980475).
Data sharing: Owing to the easily identifiable nature of the data, they are not available for sharing.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E799/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


