


Abstract
Background: Medico-legal data show opportunities to improve safe medical care; little is published on the experience of physicians-in-training with medical malpractice. The purpose of this study was to examine closed civil legal cases involving physicians-in-training over time and provide novel insights on case and physicians characteristics.
Methods: We conducted a retrospective descriptive study of closed civil legal cases at the Canadian Medical Protective Association (CMPA), a mutual medico-legal defence organization for more than 105 000 physicians, representing an estimated 95% of physicians in Canada. Eligible cases involved at least 1 physician-in-training and were closed between 1993 and 2017 (for time trends) or 2008 and 2017 (for descriptive analyses). We analyzed case rates over time using Poisson regression and the annualized change rate. Descriptive analyses addressed case duration, medico-legal outcome and patient harm. We explored physician specialties and practice characteristics in a subset of cases.
Results: Over a 25-year period (1993–2017), 4921 physicians-in-training were named in 2951 closed civil legal cases, and case rates decreased significantly (β = −0.04, 95% confidence interval −0.05 to −0.03, where β was the 1-year difference in log case rates). The annualized change rate was −1.1% per year. Between 2008 and 2017, 1901 (4.1%) of 45 967 physicians-in-training were named in 1107 civil legal cases. Cases with physicians-in-training generally involved more severe patient harm than cases without physicians-in-training. In a subgroup with available information (n = 951), surgical specialties were named most often (n = 531, 55.8%).
Interpretation: The rate of civil legal cases involving physicians-in-training has diminished over time, but more recent cases featured severe patient harm and death. Efforts to promote patient safety may enhance medical care and reduce the frequency and severity of malpractice issues for physicians-in-training.
Concerns and confusion over medico-legal liability can be common among physicians-in-training,1–4 and educators have called for data-driven resources to prepare this group for civil legal liability in their practice.5–7 To date, however, awareness has been limited by a dearth of information on civil legal case involvement for physicians-in-training.8 In this study, we analyzed data from the national medico-legal repository of the Canadian Medical Protective Association (CMPA), with an aim to describe and characterize civil legal cases involving physicians-in-training in Canada.
Our first objective was to examine how the rate of closed civil legal cases involving physicians-in-training has changed over 25 years, compared with nontrainee physician members of the CMPA. Our second objective was to characterize the severity and timing of civil legal cases involving physicians-in-training, including the severity of patient harm, case duration, and medico-legal outcomes, and contrast them with cases involving nontrainee physicians. Our third objective was to describe practice characteristics for physicians-in-training involved in a civil legal case relative to those of nontrainee members of the CMPA and other physicians-in-training in Canada.
Methods
Study design
We conducted a retrospective analysis of closed civil legal actions and threats of a civil legal action naming at least 1 physician-in-training.
Data sources
The CMPA is a national medico-legal organization for physicians with more than 105 000 members, of whom 12% are physicians-in-training. The CMPA is a not-for-profit, mutual defence association that is governed by a council of physicians from across Canada. About 95% of Canadian physicians are CMPA members, who are eligible for medico-legal assistance from the CMPA for issues arising from their medical professional work. The CMPA maintains a national repository of medico-legal data on the files for which it assists members from across the country. During the study time frame, most physicians-in-training in Canada were members of the CMPA, with the exception of most physicians-in-training practising in the province of Quebec. Eligible CMPA data were organized by case. Each case represents an instance during which a physician or multiple physicians contacted the CMPA after being named in a civil legal action, or threat of a civil legal action, involving clinical care.9–11 To situate practice characteristics of physicians-in-training, we also examined publicly available, national data from the Canadian Post-MD Education Registry (CAPER).12
Setting
To analyze trends over time, we included civil legal cases involving physicians-in-training that were closed over a 25-year period, from the start of the first complete year of CMPA digital data collection (Jan. 1, 1993) to the end of the most recent calendar year at the onset of this study (Dec. 31, 2017). To explore cases involving physicians-in-training coming from contemporary postgraduate medical education programs, we also conducted a 10-year descriptive analysis on cases with an index patient encounter between Jan. 1, 2008, and Dec. 31, 2017, an interval we believe reflects contemporary medical practice while providing a reasonable number of cases for in-depth analysis.
Case selection
We collectively refer to civil legal actions and threats of a legal action against physicians as civil legal cases. All analyses focused on closed civil legal cases involving a physician who was registered with the CMPA as a physician-in-training at the time the clinical care alleged in a civil legal action occurred.13 Cases may have involved more than 1 physician. We excluded cases in which the physician-in-training was also practising independently during the index encounter, called “moonlighting” in some regions.14 We also excluded a small number of cases where a physician-in-training was named owing to mistaken identity.
Although the CMPA repository included a physician’s status as a physician-in-training, specific information on specialty and year of training were not routinely collected. For our analysis of practice characteristics, we excluded physicians whose specialty or postgraduate year was unavailable and analyzed the remaining subgroup. For consistency and accuracy, and to confirm eligibility, all of these cases were reviewed and information was extracted first by the lead author (A.M.) and a second time by either a CMPA medical analyst or trained research assistant.
Variables
We abstracted the following variables (defined in Appendix 1, available at www.cmajopen.ca/content/10/3/E781/suppl/DC1) directly from the CMPA’s repository: patient harm,11,15 physicians named per case, medico-legal outcomes, date of index patient encounter, date of commencement, case end date and geographic region. We also derived the following variables (defined in Appendix 1): case rate, case duration, nontrainee physician specialty, physician-in-training specialty, postgraduate training year, on-call status and on-service status. In brief, case rates were the proportions of named physicians per physician-year of CMPA membership in a given practice group, multiplied by 1000.15,16
Statistical analysis
We conducted an analysis of the trend in physician closed case rates from 1993 to 2017. We stratified physician case rates by practice group, including physicians-in-training, family physicians and other specialist physicians.
We applied Poisson regression to model physician case rates as the response variable, and with year and practice group as explanatory variables. We used type III analysis to determine the significance of differences between practice groups. We also built separate models for each practice group, with year as the explanatory variable, to determine the significance of trends over time. We completed analyses using the GENMOD procedure in SAS version 9.4.
In a separate analysis, we calculated annualized change rates for each practice group as the total change rate, divided by 1 less than the number of years in the study period, where total change rate equaled the difference in case rates in 2017 and 1993, divided by the case rate in 1993.
We used frequencies and proportions (for categorical variables), and medians with interquartile ranges (IQRs) (for continuous variables) to characterize the severity and timing of cases and to describe practice characteristics for cases closed between 2008 and 2017 that involved at least 1 physician-in-training. We explored the level of patient harm and the number of physicians per case for cases involving physicians-in-training relative to cases involving nontrainee CMPA members. Similarly, we explored practice characteristics of physicians-in-training involved in cases relative to those of nontrainee CMPA members and other physicians-in-training in Canada (from CAPER data).12
Ethics approval
The ethics review panel of the Advarra (formerly Chesapeake) Institutional Review Board, based in Aurora, Ontario, and comprising Canadian members, reviewed and approved the study.
Results
Trends over time
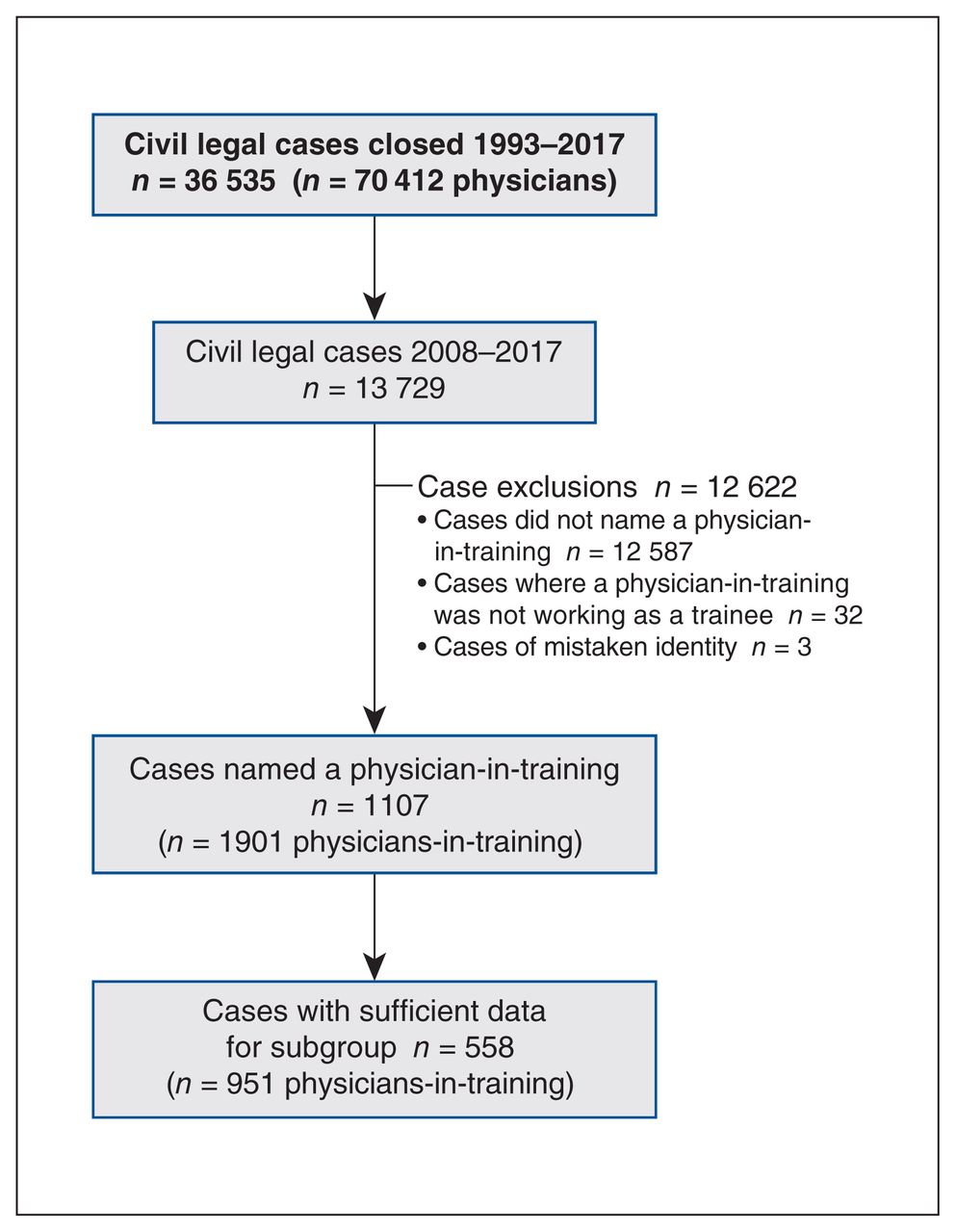
The 25-year trend analysis identified 36 535 eligible cases, representing 70 412 physicians named in a medico-legal case that was closed between 1993 and 2017 (Figure 1). Over this period, the physician case rate decreased significantly for all practice groups (physicians-in-training: β = −0.04, 95% confidence interval [CI] −0.05 to −0.03, where β was the 1-year difference in log case rates; family physicians: β = −0.02, 95% CI −0.03 to −0.02; other specialists: β = −0.02, 95% CI −0.03 to −0.02) (Figure 2). Over 25 years, there was no significant difference between the physician-in-training and family physician groups (p = 0.06), whereas other specialists had a significantly higher case rate than physicians-in-training and family physicians (p < 0.0001).

Study flow diagram.

Annual physician case rates for physicians named in a civil legal case between 1993 and 2017, where case rates are the proportions of named physicians per physician-year of membership with the Canadian Medical Protective Association in a given practice group, multiplied by 1000.
Using the annualized change rate formula, we found that the rate of physicians-in-training being named in a civil legal case decreased at an annualized change rate of −1.1% per year; the rate for family physicians decreased at −1.7% per year and the rate for other specialists decreased at −1.0% per year.
Case severity and timing
Between 2008 and 2017, there were 121 902 nontrainee physicians and 45 967 physicians-in-training who were CMPA members, fewer physicians-in-training than in national CAPER data (n = 50 602; Table 1). The CMPA closed 13 729 cases during this 10-year period. A total of 1901 physicians-in-training were named in 1107 civil legal cases that met our eligibility criteria. Across the 1107 cases, 673 (60.8%) involved patients who experienced health care–associated harm. In those 673 cases, 329 (48.9%) patients experienced little-to-moderate harm and the remaining 344 patients (51.1%) experienced severe harm or died. In contrast, among 6535 civil legal cases involving health care–associated harm that did not involve at least 1 physician-in-training, 2266 cases (34.7%) involved severe patient harm or death (Table 2).
Characteristics of physicians-in-training and nontrainee physicians who are members of the Canadian Medical Protective Association (CMPA) and of physicians-in-training in the Canadian Post-MD Education Registry*, 2008–2017
Level of patient harm in medico-legal cases with and without a named physician-in-training among closed cases in the repository of the Canadian Medical Protective Association, 2008–2017
The median number of physicians named in a case was 3 (range 1–30) for 1107 cases involving physicians-in-training (and nontrainee physicians). In contrast, there was a median of 1 physician per case (range 1–37) for 12 622 cases not involving physicians-in-training. Of the 1107 eligible cases, 1027 (92.8%) involved at least 1 additional physician and 384 (34.7%) involved at least 1 additional physician-in-training.
A civil legal case may commence many months after the case’s index patient encounter. For cases with at least 1 physician-in-training, the median time interval between a case’s index patient encounter and commencement of a civil legal case was 26 (IQR 19.7–32.7) months. From there, cases often took years to resolve. Of the 1107 cases involving physicians-in-training, 869 (78.5%) were found not to implicate the physician-in-training as the primary player in the litigation, and they were eventually released from the civil legal action after a median of 39 (IQR 24.9–64.6) months. A smaller number of cases progressed to settlement (n = 97, 8.8%) or to trial (n = 9, 0.8%). However, the median duration for these cases was longer, at 47 (IQR 33.2–68.0) months for a settlement and 75 (IQR 63.9–136.0) months for a trial.
Among the 1107 cases involving physicians-in-training, the dates of the index patient encounters were fairly evenly distributed across the 12 months of the year, with November featuring least frequently (n = 75 cases, 6.8%) and July featuring most frequently (n = 111 cases, 10.0%) (Table 3).
Months of occurrence for index patient encounters in civil legal cases involving at least 1 physician-in-training, 2008–2017
Practice characteristics
Of the 1901 physicians-in-training who were named in civil legal cases between 2008 and 2017, over two-thirds (n = 1344, 70.7%) practised in the province of Ontario. Only a subgroup of 951 physicians-in-training, involved in 558 cases (Figure 1), had information available for analysis by specialty and postgraduate year. Within this subgroup, 531 (55.9%) physiciansin-training were in a surgical specialty training program, whereas 9844 (41.0%) of the 24 012 nontrainee physicians named in a civil legal case were practising in a surgical specialty. Relative to national CAPER data,12 we noted overrepresentation of named physicians-in-training in emergency medicine, obstetrics and gynecology, general surgery and neurosurgery (Table 1).
More than half of the 951 physicians-in-training (n = 502, 52.8%) were on call at the time of the index patient encounter. Furthermore, most (n = 725, 76.2%) were working on service at the time of the index patient encounter. The exception was the group practising family medicine, which had about the same proportion on service as on call (Table 1). A greater proportion of these physicians-in-training were in the first 3 years of training (n = 535, 56.3%). This finding is not surprising given that most physicians-in-training in family medicine complete their program in 2 or 3 years and family medicine programs have more physicians-in-training than other programs. Nearly one-fifth of the named physicians-in-training (n = 170, 17.9%) were clinical fellows (Table 1).
Interpretation
Our analysis of 25-year trends showed that the case rate for physician-in-training CMPA members has decreased significantly over time. The reasons for the trend are unknown and difficult to explain. It is possible that patient safety improved overall in Canada, which resulted in fewer civil legal complaints. It is also possible that complaints against physicians were increasingly resolved through other channels besides legal action.
Few quantitative studies have considered civil legal liability of physicians-in-training; however, recent studies of malpractice data from the Comparative Benchmarking System in the United States showed that 4.1% of claims between 2007 and 2016 involved physicians-in-training,17 and 1.9% of claims between 2012 and 2016 contributed by teaching hospitals involved physicians-in-training.18 Our findings from 2008 to 2017 were slightly higher, showing that 8.1% of civil legal cases named a physician-in-training.
In line with our findings, a recent analysis of US malpractice claims involving emergency medicine physicians19 showed that cases involving at least 1 physician-in-training were associated with more severe patient harm or death than cases with no physician-in-training.
Cases involving physicians-in-training can last several years. Therefore, given 2- to 3-year residencies in Canadian family medicine programs and 4- to 5-year training programs in other specialties, civil legal cases could last the entire duration of residency and beyond. The stress caused by an unfavourable patient outcome, compounded with medico-legal matters, is potentially detrimental to the well-being of physicians-in-training;8 indeed, other research has emphasized that residents include the added stress from being named in medico-legal litigation as an adverse factor in their clinical practice or the observed practice of others.20–22
Based on other research we have conducted,23 there is evidence that physicians-in-training in Canada are increasingly calling the CMPA to request medico-legal assistance. The stress they experience from being named or potentially being named in a civil legal case remains underexplored. We found a dearth of literature about the perceptions of physicians-in-training on their medico-legal risk.
The initiation of a civil legal case does not necessarily indicate that patient harm was preventable. We focused our analysis on physicians-in-training who were named in a civil legal case, not those who provided substandard care. Our subgroup analysis of practice characteristics found that more than half of physicians-in-training named in a civil legal case were from the surgical specialties, which was a higher proportion than for nontrainee CMPA physicians (55.9% v. 41.0%, respectively). These findings confirm that physicians-in-training from surgical specialties are overrepresented in civil legal cases, aligning with US studies, which have found an overrepresentation of surgical specialties in malpractice claims.17,24,25
A recent analysis showed a significant positive association between the volume of patient safety events and civil legal cases in Canadian hospitals over a 10-year period, suggesting that improvements in patient safety could be associated with decreased medico-legal risk.26 Taken together with our findings, this body of research justifies the continued integration of more intensive or tailored risk management training as part of ongoing curricula in surgical residencies.
Limitations
We acknowledge that civil legal cases reflect a skewed sample and our analysis may not be representative of all patient safety events, preventable harm or negligent care. Our findings may not be generalizable to all physicians in Canada since a small proportion (< 5%) are not members of the CMPA. We have very limited information on cases where a CMPA member chose not to contact the CMPA for assistance with a civil legal case. Our data also underrepresent physicians in the province of Quebec. According to CAPER, physicians-in-training from Quebec made up 23.7% of Canadian residency positions between 2008 and 2017 whereas those in our civil legal cases made up 0.5%.12 The lack of information regarding the medico-legal experience of most Quebec-based physicians-in-training leaves us short of claiming a national sample.
Our study was also limited by missing data. Our physician data were not collected for research purposes; therefore, we were unable to report on specialty and other practice characteristics for some physicians-in-training. We acknowledge the possibility of selection bias insofar as we have excluded physicians whose specialty or postgraduate year was unavailable.12
Notably, we acknowledge problems in defining whether a physician-in-training was working on service or on call at the time of the relevant index encounter. The term “on call” is defined differently across specialties, particularly in specialties where both supervising physicians and physicians-in-training regularly work overnight shifts (e.g., emergency medicine and critical care medicine). Furthermore, both moonlighting status and mistaken identity were identified only through manual review and are not routinely coded at the CMPA. Therefore, we were not able to exclude these cases from the 25-year trend analysis.
We wish also to recognize that physicians-in-training often work in academic or teaching hospitals, which in some regions may mean treating cases of a higher complexity or acuity. Our observations regarding severity of harm in cases involving physicians-in-training warrant further research, particularly on the function of specialty, setting and case mix in different learning settings.
Our analysis was also not able to adjust for evidence that has shown that litigation tends to be a function of frequency.27 For example, a surgical trainee may be involved in far more surgical procedures per year than a general surgeon. Despite all limitations, we maintain that insights from medico-legal data offer numerous opportunities to make medical care safer for patients.
Conclusion
Although the rate of physicians-in-training involved in a civil legal case has decreased over time, the severity of patient harm and lengthy duration of cases can have serious, lasting impacts on physicians-in-training. We suggest that sharing these data may help physicians-in-training to anticipate and mitigate patient safety risks, and to shape their expectations for medico-legal events during postgraduate residencies and clinical fellowships. Further, a raised awareness of medico-legal patterns across specialty areas, in particular, may help stakeholders in postgraduate medical education to focus on areas of priority for addressing medico-legal risk. The role of physicians-in-training in patient safety incidents, specifically within the surgical specialties, warrants further study.
Acknowledgements
The authors acknowledge the following analysts who contributed to data capture, data cleaning and quality assurance: Anne Steen, Catherine Bernard, Robin VanderHoek and Teena Levesque. They also acknowledge summer medical students Kyung Joon Mun, Tracy Pham and Sara Trincao-Batra. The authors further wish to acknowledge additional data provided by Les Forward and Geoff Barnum on behalf of the Canadian Post-MD Education Registry (CAPER). The authors also thank the data capture team in the Department of Safe Medical Care Research at the Canadian Medical Protective Association for routine medical coding, which included classifications of patient harm.
Footnotes
Competing interests: All authors except Taryn Taylor were employees of the Canadian Medical Protective Association (CMPA) during the preparation of this manuscript. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work, and the acquisition, analysis and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was internally funded by the Canadian Medical Protective Association (CMPA). A corporate review of this manuscript took place before journal submission to ensure consistency with the CMPA mission and vision.
Data sharing: Study data are unavailable for data sharing.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E781/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.