


Abstract
Background: Kratom, a plant indigenous to Southeast Asia, which has been used both recreationally and in the treatment of pain and opioid dependence, has received little scrutiny in the United States and almost none in Canada. We analyzed calls to the British Columbia poison centre to describe caller-declared exposures to kratom and the acute health effects of these exposures.
Methods: For this descriptive analysis, we accessed electronic records, including transcriptions and extracted variables, of calls specifying kratom exposure managed by the BC Drug and Poison Information Centre (DPIC) from 2012 to 2019. We describe changes in case numbers, reasons for exposure, concurrent drug exposures and clinical outcomes over the study period.
Results: We identified 32 cases during the study period. In 23 cases (72%), the DPIC was consulted by a health care worker. Case numbers increased from 0 in 2012 to 9 in 2019. Numbers were highest for males in their 20s (n = 17, 53%). A total of 27 cases (84%) involved ingestion, with online distributors and local stores named as sources of procurement. A concurrent drug exposure was identified in 13 (41%) cases. There were no deaths; in 1 case, the exposed individual was intubated to manage agitation following kratom withdrawal.
Interpretation: We observed a steady increase in kratom-related poison centre calls from 2012 to 2019, especially in young adult males. Rising call numbers may reflect increasing availability of kratom and may be a consequence of BC’s opioid crisis, with kratom used by some to lessen symptoms of opioid withdrawal.
Mitragyna speciosa Korth., commonly known as kratom, is a plant indigenous to Southeast Asia used in traditional medical practice. Historically, kratom leaves have been brewed into tea and used as an herbal stimulant and analgesic, as well as a remedy for hypertension, diarrhea and opioid dependence.1,2 Kratom leaves contain mitragynine and related alkaloids, which are likely responsible for kratom’s psychotropic effects.3 The effects of kratom appear to be dose dependent, with stimulatory effects at lower doses (1–5 g) and sedative, opioid-like effects at higher doses (5–15 g).4 Adverse effects of kratom include nausea, vomiting and liver toxicity.5 Withdrawal symptoms include insomnia, agitation, myalgia and seizures.3,6
Dried kratom leaves, formulated into powders and pills, have recently become available in Western countries. From 2010 to 2015, US poison centres experienced a 10-fold increase in calls about exposure to kratom.7 Although most calls were not associated with severe medical outcomes, cases of psychosis, seizure and respiratory depression have been reported,2,7 particularly when kratom was consumed with other substances.8–13
In Thailand, kratom, which since 1943 had been illegal to buy, sell or possess, was decriminalized in August 2021.13,14 In Canada, although possession and consumption of kratom are not illegal, sale of kratom as a consumable natural health product has not been authorized.15 Despite this, kratom has become widely available through both online and local distributors, where it is marketed as “not consumable.”13,16 Research on kratom in the United States is sparse, composed primarily of poison centre studies.7,17–20 In Canada, there are even fewer studies, predominantly involving case reports.13,21
There are many case reports of kratom being used as a substitute for opioids or as treatment for opioid withdrawal.21–24 Since 2014, British Columbia, Canada, has seen a marked rise in opioid overdoses from the substitution of heroin and pharmaceutical opioids by fentanyl and its derivatives.25 Given kratom’s toxicity and that at high doses it has psychotropic effects similar to those of opioids, awareness by clinicians of the use of kratom in BC is important. We analyzed calls to the BC poison centre to describe exposures in which kratom was specified by the caller and the acute health effects of these exposures. We also compared numbers of kratom and opioid calls over the study period.
Methods
Study design and setting
In this descriptive analysis, we reviewed calls received from 2012 to 2019 at the BC Drug and Poison Information Centre (DPIC) in which the caller reported that kratom was consumed. The DPIC provides free drug and poison information and management support to the entire BC public (2016 population 4.6 million)26 and, through a dedicated line, to the province’s clinicians. Phone calls are managed by nurses and pharmacists with certification from the American Association of Poison Control Centers (AAPCC).27
Data sources and collection
We defined a kratom case as an individual whose declared exposure to kratom led to a call to the DPIC. Call information is collected through a series of drop-down, data-coded and narrative text fields, and is stored in Visual Dotlab, a patient management software designed for poison centres. The DPIC conducts quality checks on call information collected by new staff in their first year and for selected cases for all staff.
Cases were extracted (by D.L. and V.W.) from POISINDEX (a poison information and classification system for identifying and managing toxic exposures, used by clinicians and poison centres).28 We extracted cases with the following product codes: 7224390 (kratom) and 4271683 (plants: Mitragyna), and AAPCC generic substance code 310130 (kratom).27,29 These codes are used by all North American poison centres. Cases were also identified by searching DPIC call records for “kratom” in the non-coded “substance verbatim” field. Calls in which information about kratom was sought and there was no exposure were excluded.
We (N.R. and T.K.) accessed coded fields and reviewed the verbatim case notes recorded by DPIC poison specialists. Coded fields we assessed included age and sex of the individual exposed, caller location, caller relationship to the exposed individual (physician, pharmacist, friend or parent, self), date of exposure and call, route of exposure, amount of kratom consumed in grams, concurrent exposure substances, reason for call (adverse reaction, toxicity, withdrawal, intentional abuse, suspected suicide), acute versus chronic use of kratom and medical outcome (Appendix 1, available at www.cmajopen.ca/content/10/3/E755/suppl/DC1).
Medical outcomes for cases were classified by the DPIC as minor, moderate or major using the National Poison Data System (NPDS) classification, based on clinical effects at close of the DPIC case file (DPIC operators call back individuals in cases considered unstable and encourage follow-up calls from callers whose symptoms have not resolved).30 Cases with a minor outcome typically involved a patient with minimal symptoms as a result of the exposure who returned quickly to a pre-exposure state; cases with a moderate outcome usually involved some need for medical care but were expected to resolve without complication; and cases with a major outcome involved a life-threatening condition or resulted in serious residual morbidity where major medical intervention (e.g., intubation) would be expected.
The location of the call was classified as urban, mixed urban and rural, or rural/remote, based on BC’s Health Service Delivery Areas rurality index.31 The clinical care trajectory (managed at home, treated or evaluated at health care facility) associated with the exposure was retrieved from the coded information. Census data for the 2016 BC population was obtained from Statistics Canada.26
Narrative case notes were reviewed by 2 authors (N.R. and T.K.) working together, to create new fields not part of the Visual Dotlab case record. These additional fields included source of kratom (online, local distributor), number of follow-up calls and reason for kratom use. Reasons for kratom use included analgesia, opioid withdrawal, as a supplement, recreational and “reason unclear.” Additionally, we checked for use described as “intentional,” which is defined by the AAPCC manual as “an exposure resulting from the intentional improper or incorrect use of a substance where the patient was likely attempting to gain a high, euphoric effect or some other psychotropic effect, including recreational use of a substance for any effect.”30 The text was also reviewed to extract symptoms, signs and treatment location (Appendix 1). Differences in coding between the 2 author-reviewers were adjudicated by a senior practising DPIC poison specialist (D.L.).
To address the dose-dependent nature of kratom, we labelled cases where symptoms included respiratory failure, coma or drowsiness as “depressive effect” and cases with nausea, vomiting, anxiety, tachycardia, headache or dizziness as “stimulant effect.”4,13 Cases where the patient had discontinued kratom use for more than 12 hours after long-term exposure, and had symptoms including nausea, myalgia, diaphoresis, diarrhea, tremors, agitation or anxiety were labelled as “kratom withdrawal.”4,13 Cases where the patient presented primarily with abdominal pain, jaundice, pruritus or discoloured urine, and with evidence of hepatotoxicity such as elevated liver enzymes, bilirubin or evidence of biliary tree changes on imaging were labelled as “hepatotoxic effect.”2,5
The DPIC also records opioid-related exposure calls. We accessed these calls using a cluster of 53 AAPCC codes encompassing (typically) prescription opioids, (typically) street opioids, analgesic–opioid combinations, antihistamines/decongestants with opioids, and anti-addiction agents.32 This coding is used across North American poison control centres.
Statistical analysis
Data were analyzed and figures drawn in Microsoft Excel. Equivalence of medians was tested with the nonparametric Wilcoxon rank-sum test, and contingency tables were tested with the Fisher exact test. We calculated and compared numbers of kratom and opioid exposure cases by year per 100 000 residents based on BC’s 2016 population.26
Ethics approval
We obtained a waiver for ethics approval from the BC Centre for Disease Control data access and privacy officer, as the data did not contain identifying features and were used for surveillance purposes.
Results
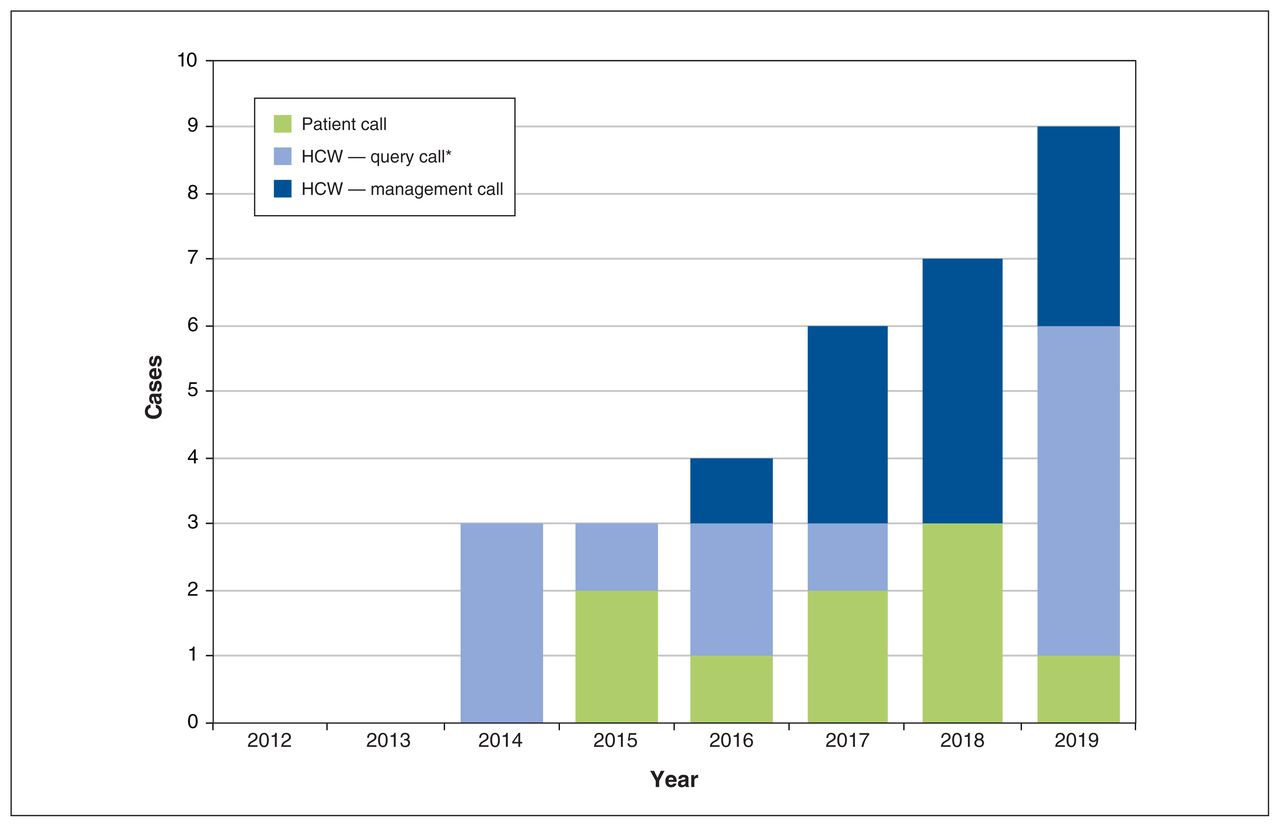
We identified 32 cases of kratom exposure from 2012 to 2019, including 1 where “kratom” was noted only in the “substance verbatim” field. There were no repeat exposures. There were no cases of kratom exposure in 2012 or 2013; case numbers increased beginning in 2014. From 2014 to 2019, there were 0.116 kratom exposures/yr per 100 000 (2016) BC residents (Figure 1).
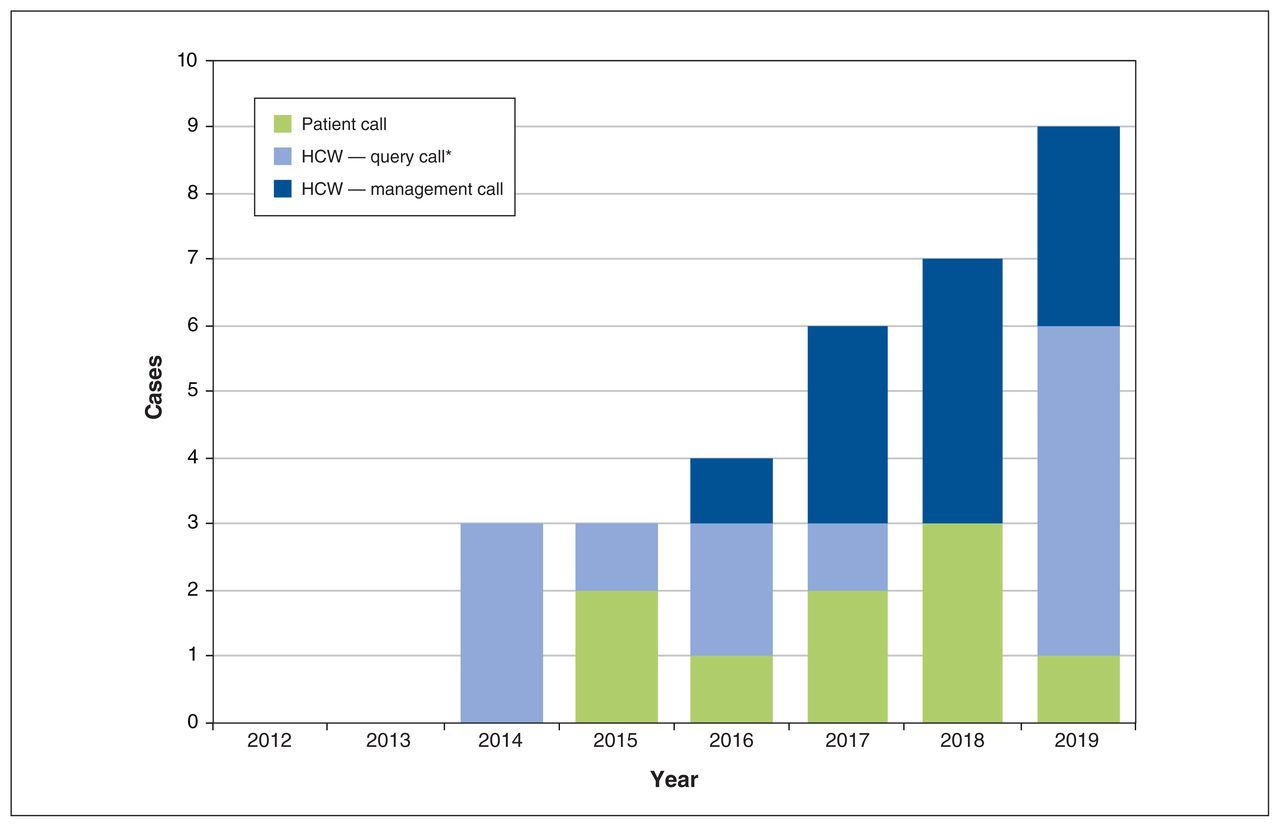
Kratom exposure calls by patients (including family and friends) and by health care workers (HCWs) and reasons for HCW calls, 2012–2019. *Query calls about toxicology, drug interactions, etc.
Patient age ranged from 17 to 79 years. There were 2 cases in adolescents aged 17 and 18 years. Age was recorded as “adult — age unknown” in 4 cases; the median age of 28 adult patients with specified age was 25.5 years. Nineteen (68%) patients were aged 20–39 years, and 4 (14%) patients were older than 50 years. Most cases (n = 25, 78%) involved a male patient (Table 1). The median age of male patients was 25.5 years, and the median age of female patients was 40 (p = 0.2, Wilcoxon rank-sum test).
Demographic characteristics of calls to the BC Drug and Poison Information Centre concerning assumed kratom exposures, 2012–2019
Two-thirds of cases (n = 21, 66%) were from metropolitan areas, 6 (19%) from mixed urban and rural settings and 5 (16%) from rural/remote areas. The corresponding values for the 2016 BC population were 56% metropolitan, 32% mixed urban and rural and 12% rural/remote (p = 0.09, Fisher exact test).
Exposed individuals, family and friends made 9 (28%) of the 32 calls. More than half (n = 19, 59%) of the calls were from physicians, and 4 (13%) were from other health care workers (nurses, emergency health technicians). Most calls (n = 19, 59%) originated in hospitals. Physicians asked about potential drug interactions, interpretation of laboratory analyses, and treatment of toxicity or withdrawal in patients (Figure 1).
Characteristics of exposures
Sources of kratom procurement volunteered to the DPIC included online distributors (n = 5, 16%), including one listed as “Kratom Canada,” and 1 local walk-in store. Most callers (n = 26, 81%) did not volunteer the source. Ingestion was the most common exposure route (n = 27, 84%); in 4 cases (13%), the route was not recorded, and there was 1 case of parenteral use. Of the cases where the form of ingested kratom was recorded (n = 18), 3 (17%) were liquids or tea, 6 (33%) were powder, 1 was leaves, and 8 (44%) were tablets.
There were 9 cases where the amount of kratom used was recorded. In 4 cases of chronic use, doses ranged from 3 g/d to 20 g/d. The doses in 5 acute exposures ranged from 3 g to 70 g.
In 13 cases, co-exposure to substances including alcohol, marijuana, benzodiazepines and others was involved (Table 2). In 1 case, concurrent exposure to an opioid (in that case, poppies) was noted. In 19 cases, no co-exposure substances were noted.
Kratom-related cases reported to the BC Drug and Poison Information Centre in which a concurrent exposure was identified, 2012–2019
In 2 cases, kratom’s concurrent use with other psychotropics suggested that it may have been taken for recreational purposes; however, no patient reported directly that kratom use was “recreational.” Five callers (16%) reported that they took kratom for pain control and 3 (9%) as self-treatment for opioid withdrawal. Two long-term users said they used kratom as a “supplement,” and another said kratom use provided “extra energy.” One short-term user took kratom to manage a “hangover, cause not specified.” In 16 cases (50%), the verbatim case notes did not inform as to why kratom was taken. In these 16 cases, the “reason for call,” a coded field, was recorded as “intentional.”
Fifteen cases (47%) involved chronic (> 21 d) exposure to kratom, and in 14 cases (44%), exposure was acute. In 3 cases (9%), use duration was not recorded.
Clinical trajectory
Most cases (n = 24, 75%) concerned kratom toxicity; however, 8 cases (25%) involved a chronic user who was experiencing symptoms of kratom withdrawal after discontinuing its use.
Stimulant effect was the most common clinical presentation, and cases with symptoms of withdrawal were also frequent. Four males aged 17–33 years presented with elevated liver enzymes; 3 of these patients had clinical manifestations of liver disease, and all of them were coded as having moderate clinical outcomes (Table 3).
Clinical presentations of kratom exposure cases reported to the BC Drug and Poison Information Centre, 2012–2019
In 3 cases (9%), the person exposed was advised to go to hospital. In 8 cases (25%), the call concerned a patient who was already hospitalized (7 in noncritical care and 1 in critical care). Eleven patients (34%) were released after evaluation and treatment at the emergency department. In 10 cases (31%), the patient’s care was managed outside of hospital; in 6 of these cases, the exposed person was at home, and in 4, the patient’s care was managed in a physician’s clinic.
More than one-third (n = 13, 41%) of cases were considered to have minor outcomes, 15 (47%) moderate and 1 major. There were no deaths. In 3 cases (9%), the medical outcome was not recorded. The 1 case with a major outcome involved intubation for control of agitation secondary to kratom withdrawal. The ratio of minor to moderate outcomes was similar in cases with exposure to other substances and cases with exposure to only kratom (Figure 2).

Medical outcome (based on National Poison Data System rules30) for cases with kratom exposure alone and with co-exposure substances.
In 13 cases (41%), there were 1 or more follow-up calls by the DPIC. Of the 13 follow-ups, 3 involved nonhospitalized individuals whose care was managed at primary care offices, and 10 involved hospitalized patients; there were no follow-ups of exposed individuals whose care was managed at home.
Kratom and opioids
Cases related to opioid use remained elevated throughout 2012–2019 and peaked at 965 in 2015. Kratom cases were much smaller in number and increased steadily from 2014 to 2019 (Figure 3).

Cases of exposure to opioids and to kratom managed by the BC Drug and Poison Information Centre, by year, 2012–2019.
Interpretation
We found a steady increase in kratom-related poison centre calls from 2012 to 2019, predominantly involving young adult males. Ingestion was the most common route of exposure. Most calls originated in hospitals and were from physicians and other health care workers asking about drug interactions, laboratory analyses, and treatment of kratom toxicity or withdrawal. Most cases were considered to have minor or moderate medical outcomes, with only 1 major outcome, which followed kratom withdrawal. DPIC cases related to opioid use remained consistently elevated throughout 2012–2019, while kratom cases increased steadily from 2014 to 2019.
In our literature search, reports of kratom exposure and its consequences were found mostly in poison centre studies, and there was no research based on hospital data. This difference may be a result of an absence of a specific International Classification of Diseases code for kratom. Poison centre records thus provide useful data on emerging substances such as kratom.
An analysis of kratom cases from Thailand’s Ramathibodi Poison Center identified 52 cases managed from 2005 to 2009.16 A case series from the Virginia Poison Center identified a kratom call as early as 2002.17 Fourteen exposures were described in a study that included calls to 5 Texas poison centres from 2009 to 2013.18 Three reports, based on calls to all US poison centres uploaded into the NPDS, described sharply rising call numbers from 2010 to 2017.7,19,20 The most comprehensive pan–United States report enumerated 1807 exposure calls from 2011 to 2017.19 More serious outcomes were associated with exposure to kratom along with other substances.19 Although these US reports provide insight into trends in kratom use, a limiting feature is that none accessed information beyond mandatory NPDS fields.
Compilations of reports from several poison centres, as in the 2013 Texas analysis, or the 2016 and 2019 studies of all cases managed by 42-plus US poison centres, use a variety of data platforms.7,17–20 Of note in our analysis, the DPIC is the sole source of poison information and management for BC, ensuring complete capture of all calls from BC residents. The DPIC has maintained an electronic database since 2012 and provides a consistent source of information recording for the province.
Kratom likely came late to BC compared with Thailand, Malaysia and Myanmar, where, although historically illegal, it has long been in use.1 Whereas in the US, cases were noted as early as 2002, besides our 2018 scan of DPIC cases from 2014 to 2017 that included 15 cases,33 only 2 Canadian case reports of kratom use have been published to our knowledge.13,21 Our current series of 32 cases shows that while calls about the use of kratom are increasing in BC, characteristics associated with its use are similar to those described in the US. Call rates were highest in northwestern US, including 3.8/million/yr in Oregon and 3.9/million/yr in Idaho between 2011 and 2017.19 Our study showed an annual call rate of 0.116/million/yr.
In the current study, the median age of patients was 25.5 years, comparable to the median age of 28 years reported by the multicentre US Centers for Disease Control and Prevention in a study of 660 cases.7 Among the cases in our study where sex was recorded, 78% of patients were male, similar to the 72% proportion reported in the US.7 Although prevalence of kratom use appears to be highest among young males, one study based on a single US poison centre did show an increase in kratom exposures in adults older than 60 years from 2014 to 2019 that mirrors the increase observed in our study.34
Almost all BC cases in our study involved ingestion as the exposure route, through powder, capsules or tea, which is consistent with US findings.7,18 In BC, there were slightly more cases of kratom use alone than cases of use with other declared substances; the most common co-exposures were alcohol, benzodiazepines and other botanicals, such as marijuana. Both findings are consistent with reports from US poison centres.7,17,19
Our study differed from other poison centre studies in the incorporation of case notes, which offered insight into reasons for kratom use. Most often, this was recorded or coded as “intentional.” We did identify a fraction who used kratom specifically for pain and a smaller fraction who used kratom for opioid withdrawal. Reference to case notes also showed that, in BC, kratom is sourced both locally and online. Rising exposure rates may reflect recent ease of access to online distribution, and one recent study indicates that most Canadian kratom vendors provide poor-quality consumer health information. 35 Using case notes, we were also able to classify clinical presentations as hepatotoxicity, kratom withdrawal, stimulant effect or depressive effect. Hepatotoxicity occurred occasionally among BC cases and was of greater medical concern, whereas the most common clinical presentation was stimulatory effect.
Despite the publication of articles about kratom in the BC Medical Journal33 and the CMAJ,36 as well as local press coverage, 37 the DPIC continues to receive requests for patient management support from clinicians. Most (72%) of the DPIC case calls were from health care workers, similar to proportions seen in US poison centre studies.7,17–19,34 As for management site, one pan-US study of 1566 kratom exposures found that 9.6% were managed outside hospital, compared with 31% of cases in BC.19 Comparing clinical outcomes, BC had a larger percentage of moderate outcomes than the pan-US poison centre study (47% v. 43%) and fewer major outcomes (3% v. 9%).19
In Canada, although the sale of kratom for consumption is not authorized, kratom is still sold and consumed. Our analysis found few severe outcomes among the 32 exposed individuals. Lacking surveys of kratom use in BC, estimates of 10 million to 16 million current regular users in the US might suggest that 100 000 or more BC residents use kratom.38 Accordingly, we suspect that only a small fraction of exposures in BC result in poison centre calls and that a much smaller fraction is associated with serious acute effects on health.
Limitations
There are limits to the comprehensiveness and quality of the information we gathered from poison centre records. Kratom exposure was self-reported, and as such, this study relies on assumed rather than confirmed exposures. The DPIC record of exposure to kratom was not validated by assessment of the substance consumed, or by biological sample. We were also limited in understanding the source of exposure, as we relied on information volunteered by users or caregivers, and there was little information regarding dose. Additionally, exposure to kratom may not have been specifically named by callers, and poison centre staff may have recorded cases as exposures to “plants” or “hallucinogens.” Lastly, it was difficult to attribute symptoms and medical outcome to kratom in cases of polysubstance use.
Conclusion
Poison centre records inform the surveillance of population exposures to potentially harmful substances. Our study of 8 years of calls to the BC poison centre about exposure to kratom shows increasing numbers, driven by ingestions in young adult men. This may reflect both increased availability of kratom and kratom’s use to mitigate opioid withdrawal. Still, serious adverse events are infrequent. As exposures continue to rise, it is important that health care professionals and regulators are aware of kratom and its effects.
Acknowledgement
The authors thank Michele Wiens, National Collaborating Centre for Environmental Health, for literature search and referencing.
Footnotes
Competing interests: Dennis Leong reports employment with the BC Drug and Poison Information Centre. Tom Kosatsky was the medical director administratively responsible for the BC Drug and Poison Information Centre during the period covered by this manuscript. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Noah Reich, Grazia Salvo and Tom Kosatsky contributed to study conception and design. Victoria Wan and Dennis Leong extracted the data and performed the statistical analysis. All authors were involved in data interpretation. Noah Reich and Tom Kosatsky reviewed case notes and drafted the manuscript. All authors gave final approval of the version to be published and have agreed to be accountable for all aspects of the work.
Data sharing: Data for this project was provided by the BC Drug and Poison Information Centre and can be accessed only by approved staff members. For this reason, study data are not available to others.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E755/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.