


Abstract
Background: There is limited research of electronic tools for self-management for patients with chronic kidney disease (CKD). We sought to evaluate participant engagement, perceived self-efficacy and website usage in a preliminary evaluation of My Kidneys My Health, a patient-facing eHealth tool in Canada.
Methods: We conducted an explanatory sequential mixed-methods study of adults with CKD who were not on kidney replacement therapy and who had access to My Kidneys My Health for 8 weeks. Outcomes included acceptance (measured by the Technology Acceptance Model), self-efficacy (measured by the Chronic Disease Self-Efficacy Scale [CDSES]) and website usage patterns (captured using Google Analytics). We analyzed participant interviews using qualitative content analysis.
Results: Twenty-nine participants with CKD completed baseline questionnaires, of whom 22 completed end-of-study questionnaires; data saturation was achieved with 15 telephone interviews. Acceptance was high, with more than 70% of participants agreeing or strongly agreeing that the website was easy to use and useful. Of the 22 who completed end-of-study questionnaires, 18 (82%) indicated they would recommend its use to others and 16 (73%) stated they would use the website in the future. Average scores for website satisfaction and look and feel were 7.7 (standard deviation [SD] 2.0) and 8.2 (SD 2.0) out of 10, respectively. The CDSES indicated that participants gained an increase in CKD information. Interviewed participants reported that the website offered valuable information and interactive tools for patients with early or newly diagnosed CKD, or for those experiencing changes in health status. Popular website pages and interactive features included Food and Diet, What is CKD, My Question List and the Depression Screener.
Interpretation: Participants indicated that the My Kidneys My Health website provided accessible content and tools that may improve self-efficacy and support in CKD self-management. Further evaluation of the website’s effectiveness in supporting self-management among a larger, more heterogenous population is warranted.
Chronic kidney disease (CKD) affects about 9% of adults in Canada.1 It is a progressive condition; 14.6% of patients with mild CKD and 16.5% with moderate CKD progress to end-stage CKD (i.e., category 5, approaching the need for or receiving kidney replacement therapy).2 Slowing the progression of CKD is a priority for patients and those who care for them,3,4 and entails lifestyle modifications, as well as medical management of relevant comorbidities.5,6
Self-management support can delay disease progression and improve quality of life for people with CKD by increasing their knowledge, skills and confidence to cope with all aspects of illness.7–9 Our previous work identified and prioritized the self-management needs of patients with CKD10,11 and informed the codevelopment of a Web-based tool to support self-management, My Kidneys My Health (MKMH) (https://mykidneysmyhealth.com/).12 Although numerous websites are available to support patients with CKD, most lack comprehensive, tailored content for patient self-management.13 In this study, we sought to assess patient engagement with MKMH, specifically the acceptability of the website, its impact on perceived self-efficacy and potential factors related to implementation and usefulness of a patient-facing eHealth tool.
Methods
Study design
We used an explanatory sequential mixed-methods design to examine acceptability of the MKMH website for adults with CKD. Our secondary objectives were to evaluate perceived self-efficacy after engagement with the MKMH website, an established correlate of self-management,14 and to explore factors related to overall engagement and future implementation. We followed the Mixed Methods Article Reporting Standards (MMARS) and the Consolidated Criteria for Reporting Qualitative Studies (COREQ) for reporting.15,16
Patient engagement
This work is supported by the Can-SOLVE CKD Network, a partnership of patients, researchers, health care providers and policy-makers.17 Our 3 patient partners (B.W., M.D., D.S.) are members of our research team and have been involved in all phases of this work.10–13,18–21 For this study, our patient partners aided in the study design (i.e., determination of the outcomes), conduct (i.e., recruitment, interview guide and reviewing results) and targeted dissemination activities (i.e., patient forums, dissemination materials).
Participants and setting
Participants were English-speaking adults (aged ≥ 18 yr) who self-reported a diagnosis of CKD, who were not on kidney replacement therapy and who had access to the Internet using a computer, tablet or mobile device.
We used a convenience recruitment strategy to recruit 25–30 participants, consistent with other studies evaluating acceptability and engagement with Web-based health applications. 22–24 The study was advertised through national kidney disease organizations in Canada (i.e., Can-SOLVE CKD Network [https://www.cansolveckd.ca/], Kidney Health Strategic Clinical Network [https://www.albertahealthservices.ca/scns/kidneyhealthscn.aspx] and Kidney Foundation of Canada [https://kidney.ca/]) via email or social media platforms. In addition, staff (nephrologists, allied health) in outpatient CKD clinics in Alberta recruited potential participants by briefly describing the study at their clinic visit. Interested individuals could self-refer themselves to the research team, or the research coordinator contacted those who provided permission to be contacted. Participant consent forms included an invitation to complete a telephone interview at the end of the intervention period.
Intervention
A detailed description of the MKMH intervention has been previously reported.12 The MKMH website is a patient-facing, open-access, interactive website that provides information on various topics in multiple formats (i.e., video with subtitles, text, audio), and tailored tools to actively engage people in executing lifestyle changes and promote enhanced communication with health care providers (e.g., My Food List, a personalized food list; Depression Screener, a mental health screening tool; My Question List, a prompt aid for discussions with health care providers). Participants had access to the MKMH website for 8 weeks (intervention period) and were directed to use it in any way they desired based on their needs. This study took place before the full launch of the website in March 2021.
Data collection
Demographic questionnaire and Internet-related skills
One week before access to the MKMH website, we collected self-reported data on participant demographics and Internet-related skills using Research Electronic Data Capture (REDCap) 10 software (Appendix 1, available at www.cmajopen.ca/content/10/3/E746/suppl/DC1). This included time since diagnosis of CKD, estimated glomerular filtration rate (eGFR), cause of CKD and comorbidities. We measured Internet-related skills using the eHealth Literacy Scale (eHEALS), an 8-item instrument that uses a 5-point Likert scale to measure an individual’s perceived ability to find, evaluate and apply eHealth information. Overall scores range from 8 to 40, with a higher score indicating better self-perceived eHealth literacy.25
Quantitative evaluation
We used 3 measurement tools for our quantitative evaluation, namely the Technology Acceptance Model (TAM), Chronic Disease Self-Efficacy Scale (CDSES) and Google Analytics.
Our primary outcome was acceptability. Eight weeks after initiating use of the MKMH website, participants completed the TAM questionnaire to explore aspects of acceptability, including perceived ease of use, perceived usefulness and determination of the intention to use.26 We operationalized these concepts through 8 questions on a 5-point Likert scale (strongly disagree to strongly agree), with the opportunity to provide additional comments. In addition, we asked 2 questions about overall satisfaction (i.e., “How do you rate your overall satisfaction with the website?” and “How do you rate the look and feel of the website?”) using a numerical rating scale from 1 (not satisfied) to 10 (extremely satisfied) (Appendix 2, available at www.cmajopen.ca/content/10/3/E746/suppl/DC1).
We collected data on perceived self-efficacy, defined as confidence in one’s ability to perform specific skills and tasks,27 using the CDSES. The CDSES measures 3 dimensions of self-efficacy, namely confidence in one’s ability to perform self-management behaviours, to manage disease in general and to achieve outcomes.28 Participants responded to each question using a scale from 1 (not at all confident) to 10 (totally confident). Higher overall scores indicate higher self-efficacy. Participants completed the CDSES 1 week before using the MKMH website and within 2 weeks after the 8-week intervention.
Google Analytics captured data on MKMH system usage to provide insights into usage patterns and behaviours between July 28, 2020, and Feb. 2, 2021. We considered time spent on the website, pages of interest, and interactive engagement activities with tailored tools. Based on our MKMH website codevelopment work, we knew a priori that intended usage (i.e., how participants should use the website to derive the maximum benefit)29 would not be the same for all participants as their individual needs differ.12 To ensure privacy, we collected aggregate data and not individual data (i.e., IP addresses).
Qualitative evaluation
To augment interpretation of our quantitative evaluation, we conducted 30-minute telephone interviews within 1 month after the intervention period. A research team member trained in qualitative research (M.Do., she/her) used a semi-structured interview guide that focused on barriers and facilitators to overall engagement (i.e., acceptability and use), adoption (i.e., perspectives on embracing the website into their self-management strategy) and implementation (i.e., determinants for integrating the website into clinical care) (Appendix 3, available at www.cmajopen.ca/content/10/3/E746/suppl/DC1). The semi-structured interview guide was created by M.Do., M.S. and B.R.H., guided by concepts of the TAM and the CDSES.26,28 To establish the relevance and clarity, 2 of our patient partners reviewed the interview guide. All interviews were audio-recorded and transcribed verbatim.
Data analysis
We used descriptive statistics to examine baseline characteristics and eHEALS, TAM and Google Analytics data. We analyzed changes in CDSES scores using a paired Student t test. We conducted quantitative data analyses using Stata v.14 (StataCorp).
We analyzed interview transcripts in NVivo (QSR International) software, version 12. We used qualitative content analysis to deductively summarize the data.30,31 Two research team members (M.Do., M.S.) independently analyzed transcripts. 31 They completed familiarization and coding on the initial 2 transcripts using a preliminary framework based on the interview guide domains. Reviewing subsequent transcripts, both members agreed upon a final framework, and indexed, charted and interpreted the data according to the framework. Credibility checks involved a third research team member (B.H.), who examined sections of analyzed transcripts and provided feedback on the final categories. Simultaneous data collection and analysis permitted exploration of the categories that emerged from the text and informed determination of when data saturation was reached (i.e., the point at which little or no new information was generated).32,33
Ethics approval
Ethics approval was obtained from the University of Calgary, Alberta (no. 20–0152) and the University of Edmonton, Alberta (no. Pro00102267). All participants provided oral consent before their participation.
Results
Between June 2020 and January 2021, 33 participants from Canada were enrolled; 28 of these were enrolled in clinic and 5 were enrolled through other avenues (e.g., online calls of participation through the Can-SOLVE CKD Network and the Kidney Foundation of Canada). Twenty-nine patients completed baseline questionnaires, 22 completed the end-of-study questionnaires and 15 completed interviews (Figure 1). Participant characteristics are shown in Table 1. There was equal distribution across participant sex, age and geographic location; however, most participants had attained a level of education greater than high school and were white. The median eHealth literacy score was 28 (interquartile range 23–32), reflecting a high level of eHealth literacy.

Study flow diagram.
Participant characteristics
Quantitative evaluation
Results from the TAM questionnaire are presented in Figure 2. With respect to ease of use, all participants reported that the content of the website was understandable; most agreed or strongly agreed that the website was easy to navigate and contained useful content for dealing with the consequences of CKD. In addition, most participants would recommend the website to others and reported that they would use it in the future. The mean overall satisfaction score was 7.7 (standard deviation [SD] 2.0) and the mean score on the website’s look and feel was 8.2 (SD 2.0), out of 10.
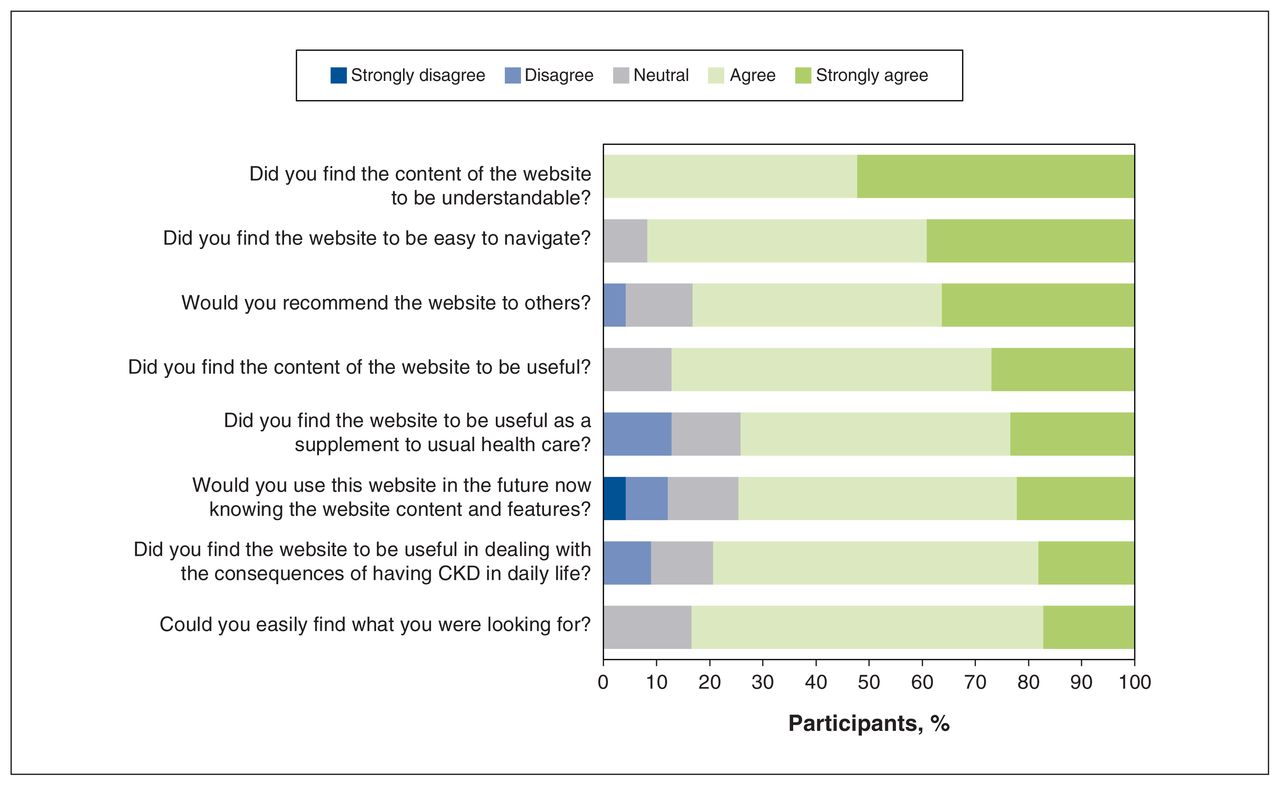
Results from the Technology Acceptance Model questionnaire after 8 weeks of access to the My Kidneys My Health website. Note: CKD = chronic kidney disease.
Results from the CDSES are presented in Table 2. Mean baseline scores were high across the subscales (range 5.7–9). We observed a statistically significant increase in participants’ confidence in their ability to get information about their disease (p = 0.033).
Participant (n = 22) scores on the Chronic Disease Self-Efficacy Scale (CDSES) at baseline and at 8 weeks postintervention
Using Google Analytics data, the average session duration was 5 minutes 40 seconds, with an average of 6.6 pages viewed per session. The top 3 pages viewed were the home page, Food and Diet, and What is CKD, and the top 3 videos viewed were How is CKD Diagnosed, Kidney Function Levels & How to Slow CKD Progression, and What do Your Kidneys Do. The website interactive features, ranked in order of popularity, were as follows: My Food List, My Question List and the Depression Screener.
Qualitative evaluation
A total of 15 patients contributed to the qualitative evaluation (Table 1). Participants voiced that the website content reaffirmed what they knew already and highlighted areas where they lacked knowledge, skills and resources, with 1 participant stating it provided, “reaffirmation of a self-management support in managing a yo-yo disease.” Figure 3 summarizes our findings for website engagement categories (i.e., acceptability, adoption, implementation), with illustrative participant quotations.

Categories of website engagement, with illustrative quotations. Note: CKD = chronic kidney disease.
Acceptability of website: ease of use
Overall, participants commented that MKMH was user friendly and easy to navigate. One participant stated, “It’s not complicated … I liked the style of it. I found it very user friendly” (P46), with others reporting that information is at your fingertips: “You can search for a food and instantly know sodium, phosphorus and potassium” (P16). One feature that was not apparent to some individuals was the prompt aid for use with health care providers (My Question List) and how to use it.
Adoption of website strategies: self-management integration
Participants spoke of how some of MKMH’s features affected their intentions and self-efficacy. For example, videos triggered individuals to seek additional information about CKD. “I wanted to expand my information as far as what I should know” (P14). Others commented on how the website influenced their lifestyle behaviours, including changing their diet and exercising, and stopping nonprescription medications that could be harmful. Some stated they would use MKMH in the future to support them in managing their CKD. Those who used the question prompt aid for use with health care providers commented that they would be more prepared for their appointments, as it would facilitate communication.
Implementation of MKMH: determinants of effective implementation
Participants provided ideas related to who would benefit from MKMH, how MKMH could be integrated into the clinical care setting and potential modifications to the website. Many participants indicated that the appropriate audience for MKMH were people with early or newly diagnosed CKD, and patients experiencing changes in their health status. Participants suggested disseminating and implementing MKMH within clinical settings where initial diagnoses are made and most routine care is provided. “By the time that somebody gets referred to a nephrologist they are usually category 4 or 5, whereas this [MKMH website] would be good to give them earlier” (P11). Suggested changes to the website included more advice and resources regarding travel, mental and sexual health, risk prediction and peer support. Other comments included ensuring the website was current, providing webinars and creating content specific to caregivers (i.e., family and friends).
Interpretation
We investigated the acceptability and usage of the MKMH website for self-management of CKD, as well as perceived self-efficacy before and after use of the MKMH. Our findings suggest that users’ acceptance of the MKMH website was high. Although perceived self-efficacy did not change for many of the subscales, participants’ confidence in gaining information about CKD increased, and interviewees discussed changing behaviours related to diet, exercise and medications. Overall, participants were interested in topics, questions and features around diet, understanding CKD and the question prompt aid for use with health care providers. Participants highlighted that MKMH would be of benefit to newly diagnosed patients and those experiencing changes in their health status.
Our conclusions are strengthened by the complementarity of the methods we used. First, responses regarding perceived accessibility were positive; however, overall mean satisfaction with the website was moderate. This discrepancy may be explained by interviewee comments that the MKMH website was most relevant for people with early or newly diagnosed CKD and those with changing health status, which were not characteristics of all patients who participated in this study. Second, we measured perceived self-efficacy using a generic, self-report questionnaire on chronic disease rather than a disease-specific instrument that captures the physical, emotional and social needs for this population. For example, some CDSES subscales may not be relevant to individuals with CKD, particularly asymptomatic patients (e.g., manage symptoms, shortness of breath). To our knowledge, there is no instrument to measure self-efficacy in patients with early CKD in the Canadian context; identifying this need, we completed psychometric testing for a potential instrument.20 The statistically nonsignificant change in scores may be related to the study time frame (i.e., during the COVID-19 pandemic) while restrictions were in place, limiting social engagements and affecting mental health, recreational activities, regular exercise and support from community and family. The availability of the website during the pandemic may have had a positive influence on patients’ ability to get information about the disease when they may have had limited access to support from health care providers. Finally, data from both Google Analytics and interviews suggested that participants were engaged with the content and interactive tools related to CKD topics, diet and health care provider questions. Engagement with virtual technologies is evolving with the COVID-19 pandemic, with the need to further explore how overall communication using MKMH can be optimized to meet patient needs.
Limitations
Study limitations include the possibility of selection bias. Participants had to have access to the Internet, excluding those who may not have regular access. Participants also had high eHealth literacy scores. In addition, most participants were recruited offline at outpatient clinics rather than online (organization websites, social media), and thus may have been more inclined and motivated to manage their condition. Our recruitment strategy may have excluded people who were disengaged in their disease management. This selection bias may have resulted in higher baseline scores on the self-efficacy questionnaire. However, both eHealth literacy and motivation reflect the current characteristics of users of a Web-based self-management support.
We were not prescriptive in terms of how often participants were to use the website; conversely, we were interested in real-world usage in a situation where they had access 24 hours a day. We captured aggregate data in Google Analytics; therefore, we cannot create individual engagement profiles to understand different patterns in use (e.g., types of activities), which may be helpful for identifying what aspects of the intervention are more engaging than others, or which features influence behaviour change. The interviews provided explanations for some of these items. Although we interviewed 15 participants, their experiences may not reflect those of a wider group of website users. Finally, our overall study size was small, with a high dropout rate, which may have limited our ability to detect a statistically significant difference in quantitative results, as well as the generalizability and interpretation of our findings.
Conclusion
Our study highlights potential adaptations to the MKMH website, including providing content specific to caregivers; more resources related to travel, peer support and mental and sexual health; a tool for predicting disease progression; new features, including webinars; and a mobile application. Further investigation of the effectiveness of the MKMH website in supporting self-management among a larger, more heterogenous population is warranted. Based on our results, we are undertaking an implementation study in the primary care setting to understand the barriers and facilitators to integrating a patient-facing eHealth tool into clinical settings.
Acknowledgement
The authors thank the patients from across Canada who participated in the study.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All authors contributed to the conception and design of the work. Maoliosa Donald and Michelle Smekal acquired data; Maoliosa Donald, Michelle Smekal and Brenda Hemmelgarn analyzed and interpreted data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work is a project of the Can-SOLVE CKD Network, supported by the Canadian Institutes of Health Research under Canada’s Strategy for Patient-Oriented Research (SPOR) grant 20R26070. The funding organizations had no role in the design and conduct of the study; data collection, analysis and interpretation; or preparation, review or approval of the manuscript.
Data sharing: In compliance with our research ethics board, data are not available for use by other researchers.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E746/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools


