


Article Figures & Tables
Figures
- Figure 1:
The organization spectrum of living donor kidney transplantation in British Columbia (based on a complex adaptive systems approach to health systems as multilevel and interconnected networks).
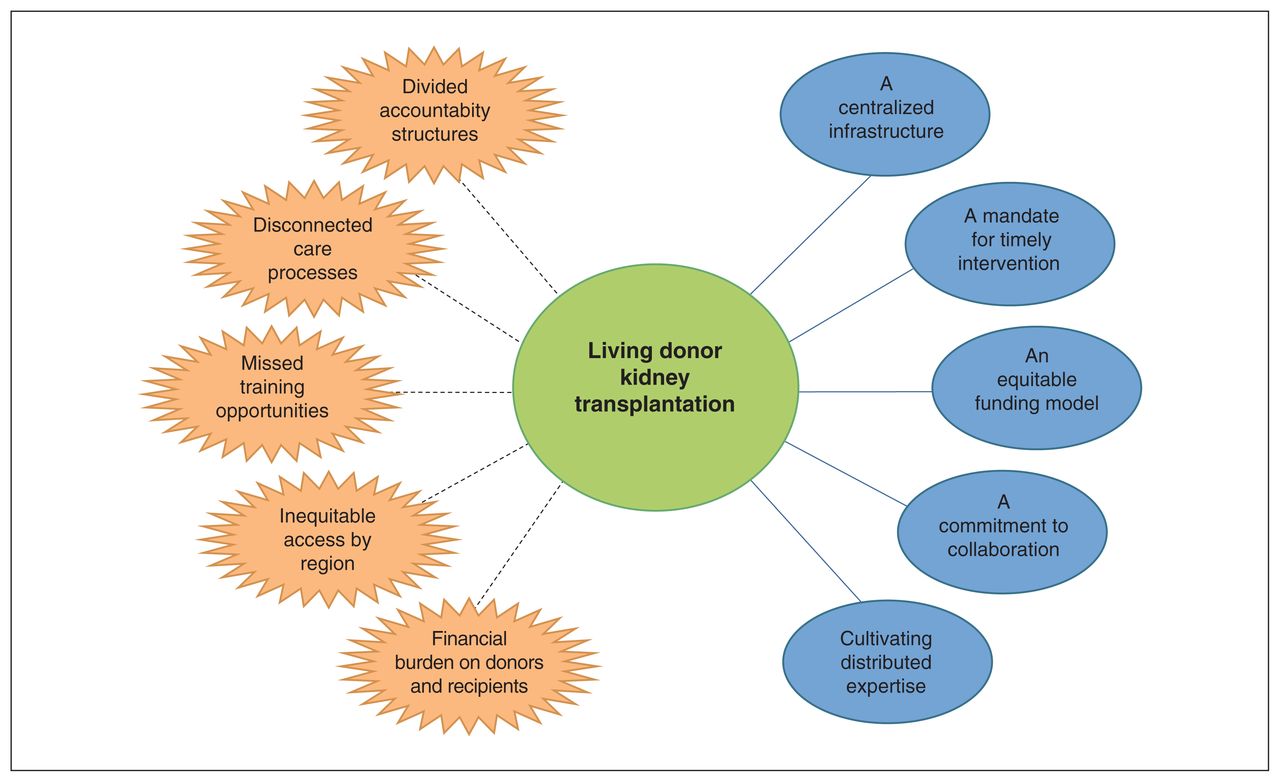
- Figure 2:
Health-system barriers (orange) and facilitators (blue) to living donor kidney transplantation in a high-performing health system in British Columbia.


Tables
- Table 1:
Participants who were interviewed for data collection within each category of the organization spectrum
Participant category and role No. of participants
n = 22Provincial organization (n = 5) Representative from BC Transplant 2 Representative from BC Renal Agency 2 Representative from the Kidney Foundation of Canada 1 Transplant centre care team (n = 7) Nephrologist 2 Social worker 2 Nurse 3 Regional unit care team (n = 8) Pretransplant clinic nurse 3 Kidney Care Clinic nephrologist 1 Kidney Care Clinic nurse 1 Kidney Care Clinic social worker 2 Dialysis centre social worker 1 Patients (n = 2) Donor 1 Recipient 1 - Table 2:
Participant quotes that illustrate each theme that was identified as a facilitator to living donor kidney transplantation in British Columbia
Theme Illustrative quote A centralized infrastructure In BC, there is one provincial health authority, which funds BC Renal [Agency] and BC Transplant through MOH [Ministry of Health] dollars and has the mandate to enable provincial services. The centralization of funding and clarity of mandate; helps break down the silos to some extent. (Representative from BC Renal Agency 1)
I think that’s a huge strength in BC, is the communication with the Kidney Care Clinics and the provincial renal agency as well as BC Transplant. We are lucky that it’s one big program here. And that the communication is the same and that we work and have the same messaging across centres and sites. (Transplant centre nurse 1)
We have the provincial renal agency, which does a lot and they promote a lot. And we have our database and we have — they are always working on new teaching and patient materials and DVDs and stuff. (Kidney Care Clinic nurse)A mandate for timely intervention So generally speaking, the Kidney Care Clinics in our province try to refer people that are transplant suitable, are eligible, when their GFR [glomerular filtration rate] is around 20–25. So the thinking is that gives us enough time to be assessing them and helping them find a donor in time. (Transplant centre social worker 1)
We’re seeing that recipients are being referred a little bit earlier for their transplant assessments, but conversations are also starting earlier about living donation. So, we will see and hear from living donors much earlier in the process so that they have time to work through it prior, ideally, before their recipient needing to start dialysis. So, we’re really trying to support pre-emptive living donor transplant where we can. (Transplant centre nurse 1)
It was just going so perfectly down the road as things went along. And it was sort of nice maybe, not to be flooded with all the information, too. (Living donor recipient)An equitable funding model So, in BC, we use let’s call it an activity-based funding model, meaning you get a certain bundle of funding per patient-year of services. And what’s built into that is all the activities that are assumed to take place through the year. And so, yeah, [in 2015] that’s when they added a lift to specifically say that one of the items, once people got down to a certain GFR [glomerular filtration rate], is that they would be assessed for transplant. It’s relevant because even though it’s just a small amount for each patient, in aggregate, it can become a large amount. And that’s what, it actually let some places — like, for example, where I work in xxxx — it let us set up a dedicated, we have a couple of dedicated nurses, who specifically do this transplant work. (Representative from BC Renal Agency 2)
It’s a lot easier to lobby a transplant organization to give you funding for transplant than it is to lobby a hospital, who has to support everything. (Representative from BC Transplant 1)A commitment to collaboration I think everybody in the renal world is pretty well-connected to ask questions or provide good care and figure out how we can make things work better. We are always kind of asking that question. (Kidney Care Clinic social worker)
There’s a large working group that includes nurses, patients, doctors, transplanters and social workers. And they’ve come up with a work plan [for Transplant First] and they’ve come up with tools. (Representative from BC Renal Agency 1)
That’s, I think, the key piece of it. Working together, working collaboratively, bringing in the regions, working with the Kidney Care Clinics. (Pretransplant clinic nurse 1)Cultivating distributed expertise So there is an initiative, a pretransplant initiative, training all our CKD [chronic kidney disease] nurses in terms of recognizing patients that would benefit from pre-emptive transplant and beginning the whole workup. So, the nephrologists are aware of this as well. But this comes from the ground up. So when I walk in to see a patient for clinic, my nurse might say, “hey, so-and-so has a donor. I was talking to her about transplant. Can we refer her?” So it’s not only got the nephrologists thinking about it, but we’ve also got our nurses prompting us. (Kidney Care Clinic nephrologist)
Everyone’s open to talking about it – all of our team members are open to talking about transplant and feel, you know, some comfort level in doing that (Kidney Care Clinic social worker) - Table 3:
Participant quotes that illustrate each theme that was identified as a barrier to living donor kidney transplantation in British Columbia
Theme Illustrative quote Divided accountability structures The other challenge, though, with doing that collaboration — you know, we would see it as being a spectrum of care. And as a clinician, I see kidney transplant as just being a spectrum of care for [a] kidney patient. Right? It’s part of their trajectory. But when [BC Transplant and BC Renal Agency] are different groups … there can be a predisposition to, kind of silo things. Which is trying to break apart, whose dollar is it that’s paid for which task, as opposed to just say, well, it’s a patient, it needs to get done and just get on with it. (Representative from BC Renal Agency 1)
There are processes at BCT [BC Transplant] over which we at BC Renal [Agency] do not have authority. But some of the processes are a little bit inefficient, but part of that is because they don’t have the funding. But I can’t give them the funding because that’s not how it works. (Representative from BC Renal Agency 1)Disconnected care processes … a big challenge for us is — from the recipient side — is making sure that all the tasks that need to be done for them to get approved, worked up and approved, get done. It’s challenging just making sure that it’s clear who’s doing what, because the way it works here, a lot of it is done regionally and then they get referred to the transplant centre downtown. Sometimes there is a bit of confusion of who’s doing what and when things are being done. You’re sitting around waiting for tests and nobody knows if it’s done or not. (Representative from BC Renal Agency 2)
Like, 3 years of me saying he’s failing and — anyways, that’s the problem, right? The system is clunky and doesn’t have a way to prioritize. (Representative from BC Renal Agency 1)
[The pretransplant process] can be very disjointed and pieces go missing. (Dialysis centre social worker)
I know that there is donor fatigue. There’s definitely donor fatigue there. (Transplant centre nurse)
There is a lack of consistency between VGH [Vancouver General Hospital] and St. Paul’s, in terms of multiple areas actually, which is a problem. (Kidney Care Clinic nephrologist)Missed training opportunities I see other social workers that are new to the area who don’t understand because they just haven’t been through it, they haven’t learned about it. They don’t understand the transplant process and therefore they can’t support patients with that transplant process. (Dialysis centre social worker)
I don’t really see a lot of trained transplant people. It’s basically on-the-job training — the people are here, let me show you what to do. (Pretransplant clinic nurse 2)
I’m just frustrated that the people that are actually in the positions, aren’t trained in the positions. And the fact that administration seems to think that, well, everything works, so we’ll just continue on as it is. You know, we’ll bring one person in and we’ll train them and then we’ll bring another one and we’ll train them. And it doesn’t work. I mean, we can see it doesn’t work. (Pretransplant clinic nurse 2)Inequitable access by region The bad thing is if you live not within driving range of Vancouver, your incentive to get a living donor is potentially marred by the notion, a. you’ve got to be away from home for 3 months, b. your donor has to come from a way. (Representative from BC Renal Agency 1)
[Kidney Care Clinics in Vancouver] have access to all that knowledge and education and processes, whereas in the regions it’s a bit different. We don’t have immediate access to that. (Pretransplant clinic nurse 1)Financial burden on donors and recipients I mean, I think everybody understands the financial benefits of living donor transplant. So, you know, this is a resource we are getting for free. So let’s put some money into it, for God’s sakes. It’s ridiculous. (Transplant nephrologist)
But the hardest part for [my donor] was all of that time off and just the financial end of it, you know. Like she doesn’t have a husband, like I say, and 2 kids, and she has to pay rent and — or mortgage, I guess — and it was very hard on her. (Living donor recipient)
My challenge is always that we don’t — the health care system and, you know, the clinicians, everybody who works to do transplant — we don’t want transplant or finances to be a barrier to transplant. But the reality is, is that it is. (Kidney Care Clinic social worker)
In this issue

{kind=link}
{kind=link}
Article tools
Respond to this article






Related Articles
Cited By...
- No citing articles found.