


Abstract
Background: Our understanding of how testing for and mutations of the BRCA1 and BRCA2 genes affect cancer risk and the use of risk-reduction strategies comes largely from studies of women recruited from specialized genetics clinics. Our aim was to assemble a generalizable cohort of women who underwent BRCA1/BRCA2 testing (the What Comes Next Cohort), irrespective of test result, to enable study of health care utilization and outcomes after testing.
Methods: This descriptive study included adult women (≥ 18 yr) who met at least 1 of 13 provincial criteria for BRCA1/BRCA2 testing and who underwent genetic testing at sites in Ontario, Canada, from 2007 to 2016. Most of the women were tested at 1 of 2 main sites, which together capture about 70% of all BRCA1/BRCA2 testing in the province. We collected detailed demographic, genetic testing and family history data through chart review for linkage with data from administrative health databases providing information on cancer history before and after testing. We followed all women to September 2019, evaluating the demographic characteristics of the cohort, indications for testing and test results.
Results: We identified 15 986 women (mean age 52.5 [standard deviation 13.9] yr) who underwent BRCA1/BRCA2 testing. Of these, 2033 women had positive results, 1175 women had variants of uncertain significance, and 12 778 women had negative results. Positive yields were 41.0% (955/2329) for predictive testing (for familial variants), 10.4% (216/2072) for Ashkenazi Jewish founder testing and 7.4% (862/11 585) for complete gene analysis. Six of the 13 provincial testing criteria had less than 10% positive yield. Among 403 women who tested negative for Ashkenazi Jewish founder mutations and subsequently underwent complete gene analysis, 12 (3.0%) tested positive for alternate pathogenic or likely pathogenic variants in the BRCA1 or BRCA2 gene.
Interpretation: Several provincial eligibility criteria for BRCA1/BRCA2 testing led to positive results in less than 10% of cases. How testing influences women’s health care behaviours, particularly those with negative results and those found to carry variants of uncertain significance, is unknown; the What Comes Next Cohort will be instrumental in the study of long-term implications of BRCA1/BRCA2 testing.
Carriers of pathogenic variants in the BRCA1 and BRCA2 genes face elevated risks of breast and ovarian cancer1 and cancer-related mortality; however, early identification of women harbouring variants can mitigate these risks. For women affected by cancer, genetic testing can guide treatment, for example, by identifying individuals who may benefit from poly(adenosine diphosphate-ribose) polymerase inhibitors. When performed among women unaffected by cancer, genetic testing can identify candidates for high-risk breast cancer screening and prophylactic surgery.2–4
Despite the availability of BRCA1/BRCA2 testing, the impact on the health behaviours of women who undergo such testing is not well understood. Studies that inform our understanding of the uptake of risk-reduction strategies among carriers of BRCA1/BRCA2 mutations have relied on patients recruited from specialized cancer or genetics clinics,5,6 and their results may not be generalizable to the broader population. Importantly, although there are some studies of cancer incidence, prevention and outcomes for women with pathogenic BRCA1/BRCA2 variants, our understanding of the implications of variants of uncertain significance and negative test results (which represent most women tested) is limited. We lack consensus on the benefit of increased surveillance and prophylactic surgery for these women, and this uncertainty can lead to variability in care.7 Few large cohorts of women with variants of uncertain significance or negative test results exist.8
The What Comes Next Cohort (WCNC), funded by the Canadian Cancer Society and the Canadian Institutes of Health Research, was established in 2016 with the aim of providing researchers with detailed genetic testing, family history, and health utilization and outcomes data for a large, unselected cohort of women who underwent BRCA1/BRCA2 testing, irrespective of test result. At inception of the cohort, its aims included assessing the uptake and variability of breast cancer screening and prophylactic surgery, quantifying the cancer risk among all test result groups and examining effects of cancer risk-reduction strategies on cancer and noncancer outcomes.9 The WCNC now provides broadly generalizable data that can be used to evaluate cancer risk, patterns of cancer treatment and prevention, and long-term cancer and noncancer outcomes after prophylactic surgery; it can also be used to perform comparative studies of women with differing test results or, through further linkage, among various health systems. In this article, we describe how we built the WCNC of women who underwent BRCA1/BRCA2 testing and also report their demographic characteristics and test results.
Methods
Study design and setting
We conducted a descriptive study detailing the characteristics of women who underwent BRCA1/BRCA2 testing in Ontario, Canada, from Jan. 1, 2007, to April 30, 2016. Since 2000, the Ontario Ministry of Health and Long-Term Care (now the Ministry of Health [MOH]) has funded BRCA1/BRCA2 testing. 10 In 2001, the ministry established 13 eligibility criteria for testing based on personal and family cancer history (Box 1). Similar to criteria used elsewhere,11 the Ontario criteria were chosen with the intention of identifying individuals with carrier probability of 10% or higher.
Ontario Ministry of HealthBRCA1/BRCA2 testing eligibility criteria
Affected individuals (breast or ovarian cancer)
At least 1 case of cancer
1. Ashkenazi Jewish and breast cancer before the age of 50 yr or ovarian cancer* at any age
2. Breast cancer before the age of 35 yr
3. Male breast cancer
4. Invasive serious ovarian cancer* at any age
At least 2 cases of cancer on the same side of the family
5. Breast cancer before the age of 60 yr combined with either a first- or second-degree relative with ovarian cancer* or male breast cancer
6. Breast and ovarian* cancer in the same individual or bilateral breast cancer with the first case before the age of 50 yr
7. Two cases of breast cancer, both before the age of 50 yr, in first- or second-degree relatives
8. Two cases of ovarian cancer,* at any age, in first- or second-degree relatives
9. Ashkenazi Jewish and breast cancer at any age, combined with any family history of breast or ovarian* cancer
At least 3 cases of cancer on the same side of the family
10. Three or more cases of breast or ovarian* cancer at any age
Unaffected individuals
11 Relative of an individual with a known BRCA1 or BRCA2 mutation
12. Ashkenazi Jewish and first- or second-degree relative of individual with breast cancer before the age of 50 yr or ovarian cancer* at any age or male breast cancer or breast cancer at any age, with a positive family history of breast or ovarian* cancer
13. A pedigree strongly suggestive of hereditary breast or ovarian cancer (i.e., risk of carrying a mutation for the individual being tested is > 10%)
↵* Including cancer of the fallopian tubes and primary peritoneal cancer.
Participants
We identified adult women (≥ 18 yr) who underwent BRCA1/BRCA2 testing between Jan. 1, 2007, and Apr. 30, 2016, primarily at 2 provincial genetic testing laboratories (North York General Hospital [NYGH] and Mount Sinai Hospital [MSH], both in Toronto). Together, these sites perform about 70% of BRCA1/BRCA2 testing provincially, serving women referred from geographically dispersed counselling centres. A small number of women who received genetic counselling at either of these 2 sites after being tested elsewhere (e.g., through Myriad Genetics, Salt Lake City, Utah) were also included if their test results were available within their genetic counselling charts. Each woman included in the cohort had to have genetic testing ordered by a physician, submission by a genetic counsellor of a requisition form stating the indication for testing, and a pedigree detailing personal and family cancer history.
Data sources
To assemble the WCNC, we abstracted charts at hospitals performing BRCA1/BRCA2 testing to obtain demographic, family cancer history and genetic testing information for the women tested. We used unique encoded identifiers to deterministically link patient records from chart review to administrative health databases housed at ICES (formerly the Institute for Clinical Evaluative Sciences), an independent, nonprofit research institute that collects and analyzes health care and demographic data for health system evaluation and improvement. Data captured in the WCNC and data available for future linkages are presented in Table 1.
Variables measured in the What Comes Next Cohort and variables available for future planned linkages
Chart review
The protocol for development of the WCNC and details of the chart review process have been described previously9 and are summarized here. We first identified all women who met the inclusion criteria, as detailed in the “Participants” section. above. We created web-based electronic case report forms using REDCap, a secure data management software platform. We used mock charts to pilot-test the case report forms before starting data collection. Trained abstractors then used electronic and paper charts to conduct the chart review for women who met the study eligibility criteria. Data abstraction was not performed in duplicate; however, the primary author (F.D.) audited the case report forms at random intervals to ensure quality and completeness of data capture.
Genetic testing
From patient charts at MSH and NYGH, we extracted the reason for testing, the type of test performed and the test result. The following 3 types of testing were performed: predictive or familial testing for a specific variant known to be carried by a family member; founder testing for 3 variants carried at highest frequency among the Ashkenazi Jewish population (BRCA1 c.68_69delAG, BRCA1 c.5266dupC and BRCA2 c.5946delT); or complete analysis, defined as sequencing of coding region and splice sites using Sanger sequencing, next-generation sequencing or analysis by denaturing high-performance liquid chromatography, and deletion/duplication detection by multiplex ligation-dependent probe amplification.
For women who underwent predictive testing, we categorized the results as positive or predictive negative based on whether the known familial variant was detected. For women who underwent Ashkenazi Jewish founder testing, we categorized the results as positive or negative. For women who underwent complete analysis, the testing sites reported test results using the 2007 and 2015 American College of Medical Genetics (ACMG) classification systems.12,13 We categorized pathogenic (ACMG category 1) and likely pathogenic (ACMG category 2) variants as positive results; ACMG category 3 variants as variants of uncertain significance; and likely benign (ACMG category 4) and benign (ACMG category 5) variants as negative results. We captured the results of prior BRCA1/BRCA2 testing if they had been reported to or performed at the genetic testing sites, applying the same categorization system.
Family cancer history
Through chart review, we abstracted information on the history of breast and ovarian cancer among first- and second-degree relatives of women in the WCNC, as listed in the detailed pedigrees included with testing requisition forms. We defined first-degree relatives as parents, siblings or children and second-degree relatives as grandparents, grandchildren, aunts, uncles, nieces, nephews and half-siblings.
Demographic and personal cancer history
From the genetic testing requisition forms and pedigrees, we obtained each woman’s ethnicity, Ashkenazi Jewish ancestry and number of biological children.
Linkage with administrative databases at ICES allowed collection of additional demographic variables. We obtained postal codes for women using the Registered Persons Database, categorizing women as living within urban (population ≥ 10 000) or rural (< 10 000) areas at the time of testing. We used Ontario Census data from 2011 and 2016 to determine the median neighbourhood household income level, categorizing women living in urban areas into 5 groups by quintile. We determined degree of marginalization using the Census-based Ontario Marginalization Index, which captures extent of material deprivation, residential instability, ethnic concentration and dependency (1 = least marginalized, 5 = most marginalized). 14 We measured health care utilization using the Aggregated Diagnosis Groups (ADGs) of the Johns Hopkins Adjusted Clinical Group System version 10.0 (Johns Hopkins University),15 with a 2-year look-back period.
For women in the cohort, we used linkage with the Ontario Cancer Registry at ICES to collect information about personal cancer history. Since 1964, the Ontario Cancer Registry has collected data on all incident invasive cancers, excluding non-melanoma skin cancers, and the registry is over 95% complete.16 Data populating the registry are collected from hospital discharge and day surgery summaries, pathology reports, records for patients referred to specialized cancer centres in Ontario and death certificates where cancer is identified as the cause of death.17 The registry also contains patients’ demographic information and details of their cancer diagnosis, including cancer type and date of diagnosis. We used this registry to determine cancer history before genetic testing and cancer occurrence afterward. We included fallopian tube and primary peritoneal cancers in our definition of ovarian cancer.
Follow-up
Follow-up began on the date of the genetic test and continued until the earliest of death or last follow-up in the administrative data. We determined participants’ vital status through the Registered Persons Database.
Statistical analysis
We determined baseline characteristics of women in the WCNC at the time of their most recent genetic test. We report continuous data as means (with standard deviations [SDs]) and categorical data as frequencies (percentages). Where we performed comparisons by genetic test result, we categorized the women on the basis of the most recent genetic test. We compared groups using analysis of variance and χ2 tests. We report missing data, where such were encountered, and we performed complete case analysis. The reported p values are 2-sided. We performed all analyses at ICES using R software, version 3.3. In accordance with ICES policies, we suppressed cells with fewer than 6 individuals.
Ethics approval
This study was approved by the research ethics boards at MSH (13-0124), NYGH (16-0035), Sunnybrook Health Sciences Centre (275-2016) and the University of Toronto (37301).
Results
The WCNC includes 15 986 women who underwent BRCA1/BRCA2 testing between 2007 and 2016 (Figure 1): 2329 (14.6%) who underwent predictive testing, 2072 (13.0%) who underwent Ashkenazi Jewish founder testing and 11 585 (72.5%) who underwent complete BRCA1/BRCA2 gene analysis. Of those tested, 2033 (12.7%) had a positive result, 1175 (7.4%) had a variant of uncertain significance, 11 437 (71.5%) had a negative result on founder testing or complete analysis, and 1341 (8.4%) had a negative result on predictive testing.
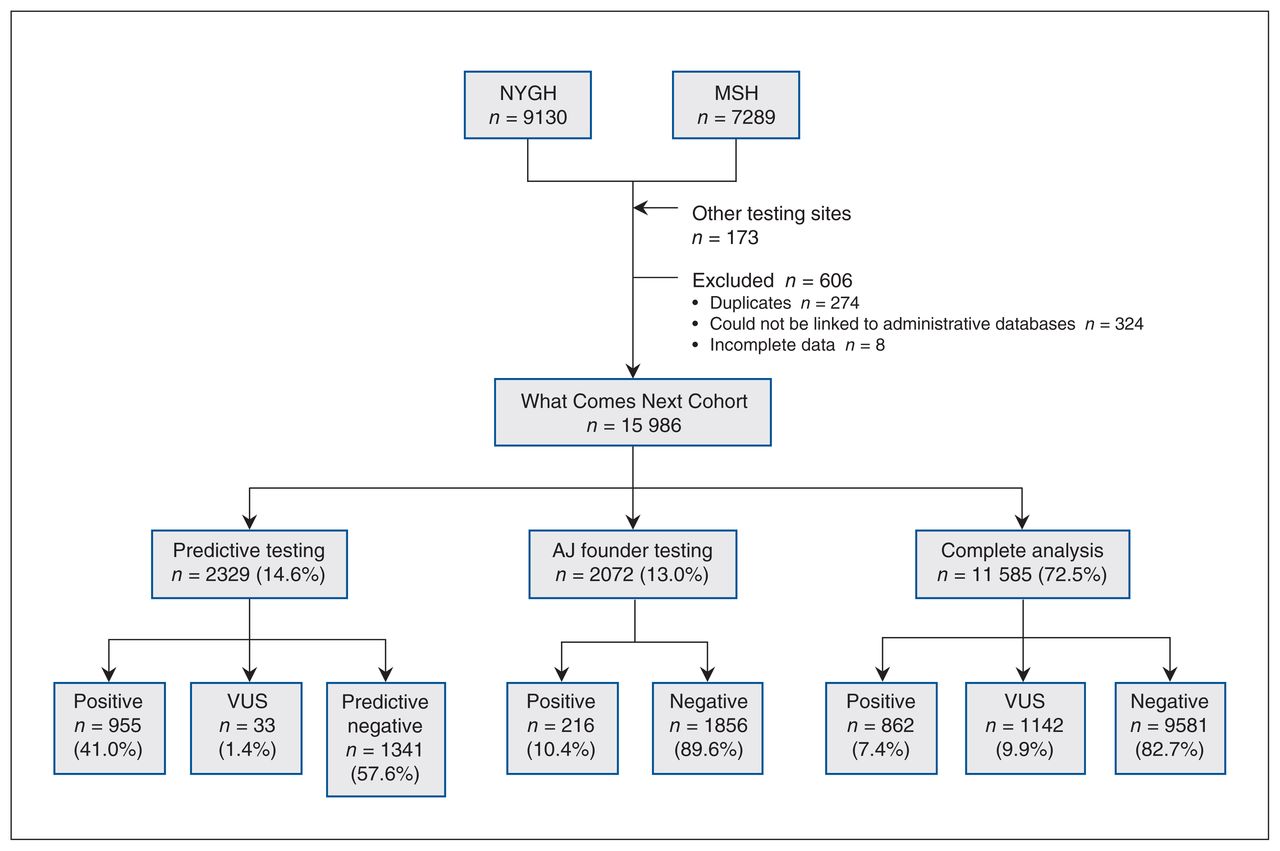
Derivation of the What Comes Next Cohort and results of various tests. Note: AJ = Ashkenazi Jewish, MSH = Mount Sinai Hospital, NYGH = North York General Hospital, VUS = variant of uncertain significance.
Table 2 summarizes the demographic characteristics of women in the cohort. The mean age was 52.5 (SD 13.9) years, with 12.1% of the women living in urban neighbourhoods belonging to the lowest quintile income group and 28.0% living in urban neighbourhoods in the highest quintile income group. Although chart abstraction was performed at only 2 hospitals, women in the WCNC resided across the province of Ontario (Figure 2). As of September 2019, median follow-up was 5.9 years, with 100 438 person-years of follow-up.
Baseline characteristics of the What Comes Next Cohort at the time of genetic testing
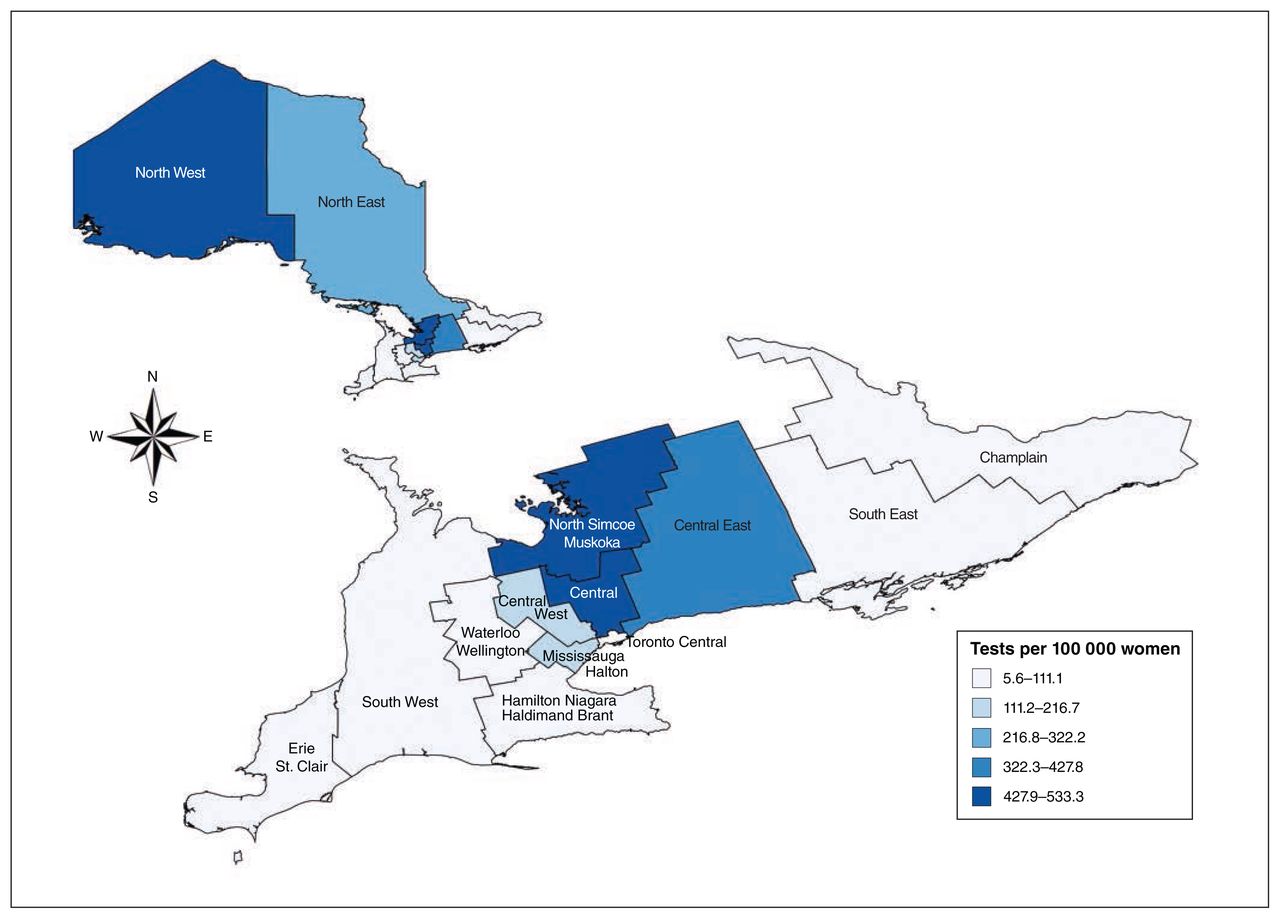
Number of women captured by the What Comes Next Cohort, by geographic region (i.e., Local Health Integration Network) in Ontario. Note: Colours represent numbers of women included in the cohort (i.e., underwent testing) per 100 000 women living within each region, based on population estimates from 2016. This map was reproduced with permission of Public Health Ontario.
Test results
Among the 2033 women who had a positive result, 1035 (50.9%) had pathogenic or likely pathogenic variants in BRCA1, 990 (48.7%) had pathogenic or likely pathogenic variants in BRCA2, and 8 (0.4%) had pathogenic or likely pathogenic variants in both BRCA1 and BRCA2. Positive yield was 41.0% (n = 955) among those who underwent predictive testing, 10.4% (n = 216) among those who underwent founder testing and 7.4% (n = 862) among those who underwent complete analysis.
We found a variant of uncertain significance in 1142 (9.9%) of the 11 585 women who underwent complete analysis; another 33 women underwent predictive testing for a familial variant of uncertain significance and were found to carry such a variant. Among these 1175 women with a variant of uncertain significance, 376 (32.0%) carried a variant in BRCA1, 754 (64.2%) carried a variant in BRCA2, and 45 (3.8%) carried variants in both BRCA1 and BRCA2.
A total of 743 (4.6%) of the women had undergone multiple BRCA1/BRCA2 tests. In addition, 403 women with a negative result on Ashkenazi Jewish founder testing also underwent complete gene analysis (either immediately or subsequently); the positive yield of complete analysis in these women was 3.0% (n = 12), and variants of uncertain significance were identified in 35 (8.7%) of these women.
Indications for testing
Testing indications, based on MOH criteria, are presented in Table 3. Testing was most commonly performed in women with breast or ovarian cancer from families with 3 or more cases of breast or ovarian cancer (n = 5293, 33.1%) and women who were relatives of a BRCA1/BRCA2 carrier (n = 2394, 15.0%). In addition, 2105 (13.2%) women were tested because of a pedigree strongly suggestive of hereditary breast or ovarian cancer. The greatest positive yield was achieved with testing undertaken in relatives of BRCA1/BRCA2 carriers (n = 860, 35.9%), followed by testing among women with breast or ovarian cancer from families with 2 cases of ovarian cancer among first- or second-degree relatives (n = 52, 26.7%) and women with invasive serous ovarian cancer (n = 195, 14.7%).
Indications for and yield of testing by Ontario MOH* testing criteria
Although the testing criteria were developed to identify women with at least a 10% risk of testing positive, 6 criteria had less than 10% positive yield, and one of these had less than 5% yield. The lowest yields were obtained with testing of women whose pedigrees suggested a greater than 10% risk of carrying a pathogenic variant (n = 93, 4.4%) and Ashkenazi Jewish women with breast cancer and a family history of breast or ovarian cancer (n = 38, 5.5%).
Personal cancer history
A history of cancer was present among 10 345 (64.7%) of the women who underwent testing, including breast cancer in 8006 (50.1%) (Table 4). The mean age at breast cancer diagnosis was 49.7 (SD 11.8) years and was highest among women with a predictive negative result (mean 55.6 [SD 13.6] yr). A total of 197 (8.5%) women who underwent predictive testing had a history of breast cancer before testing. Women with a history of breast cancer who underwent predictive testing more often received a positive result than women without a breast cancer history (75.6% v. 38.4%, p < 0.001).
Family and personal cancer history by test result
Among women who underwent nonpredictive testing, the proportion without a history of breast cancer who received a positive result was greater than the proportion who had a history of breast cancer (9.0% v. 7.0%, p = 0.005). This was expected, given that women who undergo nonpredictive testing in the absence of breast cancer likely have other high-risk factors, such as ovarian cancer or a strong family history. Women with positive results were younger at breast cancer diagnosis than women who had variants of uncertain significance or negative results (means 44.5, 48.8 and 50.3 yr, respectively; p < 0.001).
A total of 1589 women (9.9%) had a history of ovarian cancer before genetic testing (Table 4). Among women who underwent nonpredictive testing, those with a history of ovarian cancer more often received a positive result than those without ovarian cancer (16.9% v. 6.7%, p < 0.001). Women testing positive were diagnosed with ovarian cancer at a younger age than women who had variants of uncertain significance or negative results (means 53.9, 56.4 and 60.0 yr, respectively; p < 0.001).
Family cancer history
Family history of breast cancer in first- or second-degree relatives was present for 11 241 (70.3%) of the women (Table 4). Proportionally, more of the women who underwent predictive testing had a first-degree relative with breast cancer than those who underwent founder testing or complete analysis (1224/2329 [52.6%], 895/2072 [43.2%] and 5328/11 585 [46.0%], respectively; p < 0.001). Among women who underwent nonpredictive testing, those who had first-degree relatives with breast cancer tested positive as often as those who had second-degree relatives with breast cancer (7.2% and 7.9%, respectively; p = 0.1).
Family history of ovarian cancer in first- or second-degree relatives was present for 3705 (23.2%) of the women (Table 4). Those in the predictive testing group were most likely to have a first-degree relative affected by ovarian cancer (477 [20.5%] of the 2329 who underwent predictive testing, 179 [8.6%] of the 2072 who underwent founder testing and 1340 [11.6%] of the 11 585 who underwent complete analysis; p < 0.001). Among women who underwent nonpredictive testing, similar proportions of women with affected first- and second-degree relatives tested positive (12.8% and 11.0%, respectively; p = 0.1).
Interpretation
The WCNC represents about 70% of women in Ontario who underwent BRCA1/BRCA2 testing over a 10-year period within a publicly funded genetic testing program. The cohort includes nearly 16 000 women, with large numbers of previously understudied women who have variants of uncertain significance and negative test results. Despite the provincial goal of testing women with carrier probability of 10% or higher, we identified 6 testing criteria with less than 10% positive yield, and 1 criterion with less than 5% yield. Additionally, 3% of the women who had negative results on Ashkenazi founder testing and who underwent complete gene analysis carried pathogenic or likely pathogenic variants.
To date, most of the data that are important for understanding cancer development and prevention among women at high risk for breast or ovarian cancer have come from highly specialized genetics clinics. Capture of data solely from women motivated to attend these clinics may overestimate uptake of risk-reduction strategies. Generalizable data have been difficult to obtain because factors important to understanding cancer development and prevention (e.g., family history and genetic testing results18) are not routinely collected in administrative data sets. Additionally, it can be challenging to prospectively recruit and follow a large group of women with variants of uncertain significance or negative results. Through a combination of detailed chart abstraction and linkage with administrative data sets, the WCNC overcomes these challenges.
Although most of the genetic testing was performed at 2 sites in Toronto, women in the cohort came from genetic counselling centres in many jurisdictions. The testing was provincially funded throughout the study period, so affordability of testing did not limit access. By capturing the indication for testing, we were able to assess the performance of testing criteria. For future studies, linkage to administrative data sets in Ontario will enable tracking of all publicly funded health care utilization (i.e., ambulatory care visits, hospital admissions, surgeries, chemotherapy and radiation therapy) before and after genetic testing, with minimal attrition over long-term follow-up. We plan to regularly update the follow-up data for this cohort. Importantly, our cohort includes all women who were tested, not just those with a positive result.
Using this data platform, we hope to explore many of the unanswered questions important for counselling women who are undergoing BRCA1/BRCA2 testing and help to resolve ambiguity for physicians involved in shared decision-making. Ongoing and future projects seek to understand how decisions for prophylactic surgery are affected by the timing of genetic testing; to quantify the use of high-risk screening and surgery among women with variants of uncertain significance and negative test results; to provide estimates of lifetime cancer risk among women with variants of uncertain significance or negative results, with consideration of family history; to better understand the implications of risk-reducing strategies for cancer incidence and survival; to evaluate the use and efficacy of neoadjuvant therapy among women with BRCA1/BRCA2 variants; and to better understand the long-term adverse effects of treatments selected for BRCA-positive women (e.g., chemotherapy-related cardiotoxicity, long-term effects of oophorectomy).
Limitations
Despite its strengths, the WCNC also has limitations. During the chart review, we were unable to identify instances where members of the same family underwent testing, and therefore we could not track cascade testing. Capture of family history information relied upon accurate recall by the women who underwent testing.
Although we captured the genetic test result, we cannot be certain how the test results were communicated. This factor may be particularly important in understanding health care decisions made by women with variants of uncertain significance or negative results.19
Although the 2 main testing sites included in our study perform about 70% of BRCA1/BRCA2 testing in the province, women not included in our cohort may differ in terms of demographic characteristics, socioeconomic status or access to care. Given that our cohort consists of women from geographically diverse areas across Ontario, including women living at a distance from high-volume cancer centres, future projects will be able to explore how care and outcomes differ by demographics and geography.
Finally, our cohort includes only women who have undergone BRCA1 or BRCA2 testing (or both). We do not have data on men who underwent BRCA1/BRCA2 testing or any individuals who underwent panel testing (implemented in Ontario in 2016). The patterns seen here may not reflect those of panel testing.
Conclusion
The WCNC is a source of broadly generalizable data that can be used in future studies to evaluate cancer risk, cancer treatment and the use of cancer risk-reduction strategies among women who have undergone BRCA1/BRCA2 testing, irrespective of the test result. This cohort will allow researchers to perform comparative studies of women with different test results with a sufficiently large sample size to evaluate rare outcomes. It also has the potential to substantially further our understanding of hereditary cancers and their treatment and prevention.
Footnotes
Competing interests: None declared.
Contributors: Fahima Dossa, Kelly Metcalfe, Rinku Sutradhar, Andrea Eisen, Kathy Chun, Jordan Lerner Ellis and Nancy Baxter contributed to the concept and design of the cohort. Fahima Dossa, Kelly Metcalfe, Tari Little, Andrea Eisen, Kathy Chun, Wendy Meschino, Lea Velsher, Jordan Lerner Ellis and Nancy Baxter participated in data acquisition. Fahima Dossa analyzed the data. Fahima Dossa, Kelly Metcalfe, Rinku Sutradhar and Nancy Baxter contributed to data interpretation. Kelly Metcalfe, Rinku Sutradhar and Nancy Baxter provided administrative support and supervision. Nancy Baxter obtained funding. Fahima Dossa drafted the manuscript. All of the authors critically revised the manuscript, approved the version to be published and agreed to be accountable for the work.
Funding: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC; now 2 separate ministries). This study also received funding from the Canadian Cancer Society (grant no. 315358), the American College of Surgeons Resident Research Scholarship (to Fahima Dossa) and a Post-Doctoral Fellowship Award from the Canadian Institutes of Health Research (to Fahima Dossa). Genetic testing was supported by the MOHLTC.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (now 2 separate ministries). Parts of this material are based on data and information compiled and provided by Cancer Care Ontario, the Canadian Institute for Health Information, and Immigration, Refugees and Citizenship Canada (the latter current to September 2019). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of any of the funding or data sources; no endorsement by any of these organizations is intended or should be inferred. In addition, Public Health Ontario (the source of Figure 2 in this article) assumes no responsibility for the content of any publication resulting from translation/changes/adapation of its documents by third parties.
Data sharing: The data set for this study is held securely in coded form at ICES. Although data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors upon request, with the understanding that these computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/3/E874/suppl/DC1
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 CMA Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools


