


Abstract
Background: Patients with chronic kidney disease (CKD) and heart disease face challenging treatment decisions. We sought to explore the perceptions of patients and physicians about shared decision-making for coronary procedures for people with CKD, as well as opinions about strategies and tools to improve these decisions.
Methods: We partnered with 4 patients with CKD and 1 caregiver to design and conduct a qualitative descriptive study using semi-structured interviews and content analysis. Patient participants with CKD and either acute coronary syndrome or cardiac catheterization in the preceding year were recruited from a provincial cardiac registry, cardiology wards and clinics in Calgary between March and September 2018. Cardiologists from the region also participated in the study. Data analysis emphasized identifying, organizing and describing themes found within the data.
Results: Twenty patients with CKD and 10 cardiologists identified several complexities related to bidirectional information exchange needed for shared decision-making. Themes identified by both patients and physicians included challenges synthesizing best evidence, variable patient knowledge seeking, timeliness in the acute care setting and influence of roles on decision-making. Themes identified by physicians related to processes and tools to help support shared decision-making in this setting included personalization to reflect the variability of risks and heterogeneity of patient preferences as well as allowing for physicians to share their clinical judgment.
Interpretation: There are complexities related to bidirectional information exchange between patients with CKD and their physicians for shared decision-making about coronary procedures. Processes and tools to facilitate shared decision-making in this setting require personalization and need to be time sensitive.
Plain language summary: People with chronic kidney disease (CKD) often develop heart disease. Although heart procedures can improve outcomes of high-risk patients and reduce symptoms, patients and physicians must accept potential risks and weigh whether benefits are anticipated to exceed these risks. Shared decision-making is an approach in which clinicians and patients share best available evidence and work together to come to a decision informed by the clinician’s expertise and the patient’s values, goals, needs and preferences. In this study, we explore the perceptions about challenges to shared decision-making in this setting, as well as opinions about strategies and tools to improve these decisions. We partnered with 4 patients with CKD and 1 caregiver to design and conduct a qualitative descriptive study, analyzed thematically. Twenty patient participants with CKD and either acute coronary syndrome or cardiac catheterization and 10 cardiologists were recruited to participate. Patients and cardiologists both highlighted the complexity of information exchange, including the impact of variability in knowledge seeking and understanding by patients when discussing risks and benefits of procedures. Patients identified trust in the physician as key to their confidence in decision-making. Cardiologists identified the importance of their role in guiding patients towards evidence-informed medical decisions based on their clinical assessment of risks as well as patient values and preferences. Challenges and potential usefulness of decision aids were identified by both patients and cardiologists. Our findings suggest that processes and tools to support shared decision-making in this setting should be personalized to reflect variability of risks and patient preferences and allow for physicians to contribute their clinical judgment.
Invasive management of coronary artery disease, including coronary angiography with percutaneous or surgical revascularization, can improve long-term outcomes of high-risk patients and reduce symptoms, but patients and physicians must accept potential procedural risks and weigh whether benefits are anticipated to exceed these risks.1 The decision whether to pursue an invasive or medical approach to treatment for coronary disease may be particularly challenging for patients with chronic kidney disease (CKD) because, although rates of coronary events exceed 10 per 1000 person-years for people with CKD who are 50 years or older (i.e., high-risk status), these procedures may lead to worsening kidney function or precipitate a need for dialysis, and there is less certainty about treatment benefits.2–6 As a result, treatment selection is substantially different for patients with CKD compared with other groups of high-risk patients. There is a 20% to 50% lower likelihood for patients with CKD to receive early (within 48 hours of admission) invasive management for non–ST elevation acute coronary syndrome (ACS)7,8 when compared with similar patients without CKD.
Ideally, both patients and clinicians make important contributions to treatment decisions for ACS. Recent research on the decision-making preferences of patients admitted to hospital with myocardial infarction9 reported that more than two-thirds of patients wanted to play an active role in decision-making, with most believing both patients and physicians share a role in arriving at treatment decisions. Despite this, patients have reported that they often experience challenges participating in acute care decision-making.10 Shared decision-making is an approach in which clinicians and patients share best available evidence and work together to come to a decision informed by the physician’s expertise and the patient’s values and goals, needs and preferences, and risk tolerance.11,12 Shared decision-making can result in treatment decisions that better reflect patients’ goals, increase patient and physician satisfaction and improve outcomes.11,12 It remains uncertain whether shared decision-making could be used to improve the decision quality and experiences of cardiac care for patients with CKD.
This qualitative study explored the perceptions of both patients and physicians about challenges to shared decision-making for coronary procedures in patients with CKD, as well as opinions about strategies and tools to improve these decisions.
Methods
To illuminate poorly understood aspects of experiences, we used qualitative descriptive methods13 to conduct and analyze individual, semistructured interviews with patients with CKD who had experienced a non–ST elevation ACS or had undergone cardiac catheterization in the preceding year, and individual semistructured interviews with cardiologists experienced in ACS care.
Setting and participants
Patients were recruited from March to September 2018 from across Southern Alberta using the cardiac registry of the Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (www.approach.org), from the cardiology ward of a tertiary referral hospital (Foothills Medical Centre) and nephrology clinic (Sheldon M. Chumir Health Centre) in Calgary. Patients were eligible for inclusion if they had CKD with an estimated glomerular filtration rate (eGFR) of less than 45 mL/min/1.73m2 before admission to hospital, and had been admitted to hospital with ACS or underwent cardiac catheterization within the preceding year. Purposive sampling, a type of nonprobability sampling, was used for the recruitment from CKD clinics intentionally to select some patients who had experienced acute kidney failure requiring dialysis after invasive coronary procedures for inclusion in the study.14
Patients who were 18 years of age or older and able to communicate in English participated in an in-person or telephone interview, including any family member or caregiver that they wished to include. Participating patients and family members or caregivers were provided an honorarium of $50.
Cardiologists were purposively sampled from the Cardiac Catheterization Lab at Foothills Medical Centre, Calgary, and invited via email to participate in an individual, semistructured interview. Physicians received no compensation for participating.
Sources of data
The interview guide (Appendix 1, available at www.cmajopen.ca/content/8/4/E860/suppl/DC1) was developed with input from patient partners, researchers and physicians (cardiologists and nephrologists) based on the Ottawa Hospital Research Institute needs assessment guideline.15 Questions for patients explored reactions and decisions surrounding their cardiac care, including their perceptions regarding information provided to them at the time of the event and their role in decision-making. Cardiologists answered questions about their approach to decision-making for ACS care and coronary procedures of patients with CKD, and their own perceptions regarding practices, processes and tools for shared decision-making.
Interviews with patients or caregivers and cardiologists were 30 to 40 minutes in duration and conducted via telephone or in person at a location convenient for the participant. One research associate conducted all interviews to maintain consistency. All interviews were audio-recorded, transcribed verbatim and de-identified (except for patient or caregiver or cardiologist designation) before analysis. The data collection and analysis were iterative, and data analysis informed data saturation when no new descriptive themes emerged. Patient and cardiologist interviews ceased when saturation was achieved.
Patient engagement
Patient-oriented research engages patients as partners, focuses on patient-identified priorities and aims to apply the knowledge generated to enhance health care systems and practices.16 Our study was supported by 4 patients with CKD and heart disease and 1 caregiver who met with other members of the research team on a recurring basis for the duration of the study and provided input to the program of research. Patients partnered with us to inform the design of the study, study information material for patients and the interview questions for patients. Two patient partners (W.P. and C.C.) volunteered to participate in the analysis when invited to broaden the interpretation and credibility of the themes identified. Their perspectives were incorporated into interpretation of findings and they also contributed to coauthoring the manuscript and presenting at the Can-SOLVE CKD annual meeting (www.cansolveckd.ca).
Data analysis
Three research associates (J.F., P.A.J. and T.W.) inductively analyzed all 20 of the patient or caregiver and 10 cardiologist transcripts using qualitative content analysis.17–19 Each research associate independently reviewed the transcripts word-by-word, highlighting the precise words that appeared to capture crucial concepts and then making notes of the main impressions and thoughts to develop codes using NVivo software. The research associates then met with the principal investigator (M.T.J.) on a monthly basis to discuss and reach consensus on emerging codes and grouping and to organize themes and create meaningful clusters. Research associates met after coding the first 5 transcripts to finalize the coding scheme, and the agreed upon codes and themes were systematically applied to all subsequent transcripts.20,21 Themes, their descriptors and representative quotes were reviewed with patient partners (W.P. and C.C.) to ensure that their own experiences were reflected in the data.
Ethics approval
The University of Calgary Conjoint Health Research Ethics Board approved the research project (CHREB no. 150476).
Results
The demographic characteristics of 20 patient and 10 physician participants are provided in Table 1 and Table 2, respectively. The patients interviewed were 42 to 83 years old and included 5 (25%) women and 1 caregiver. Cardiologists interviewed had been practising from 3 to 37 years.
Characteristics of patients (n = 20) with acute coronary syndrome or cardiac catheterization in the preceding year*
Characteristics of physicians (cardiologists) (n = 10)
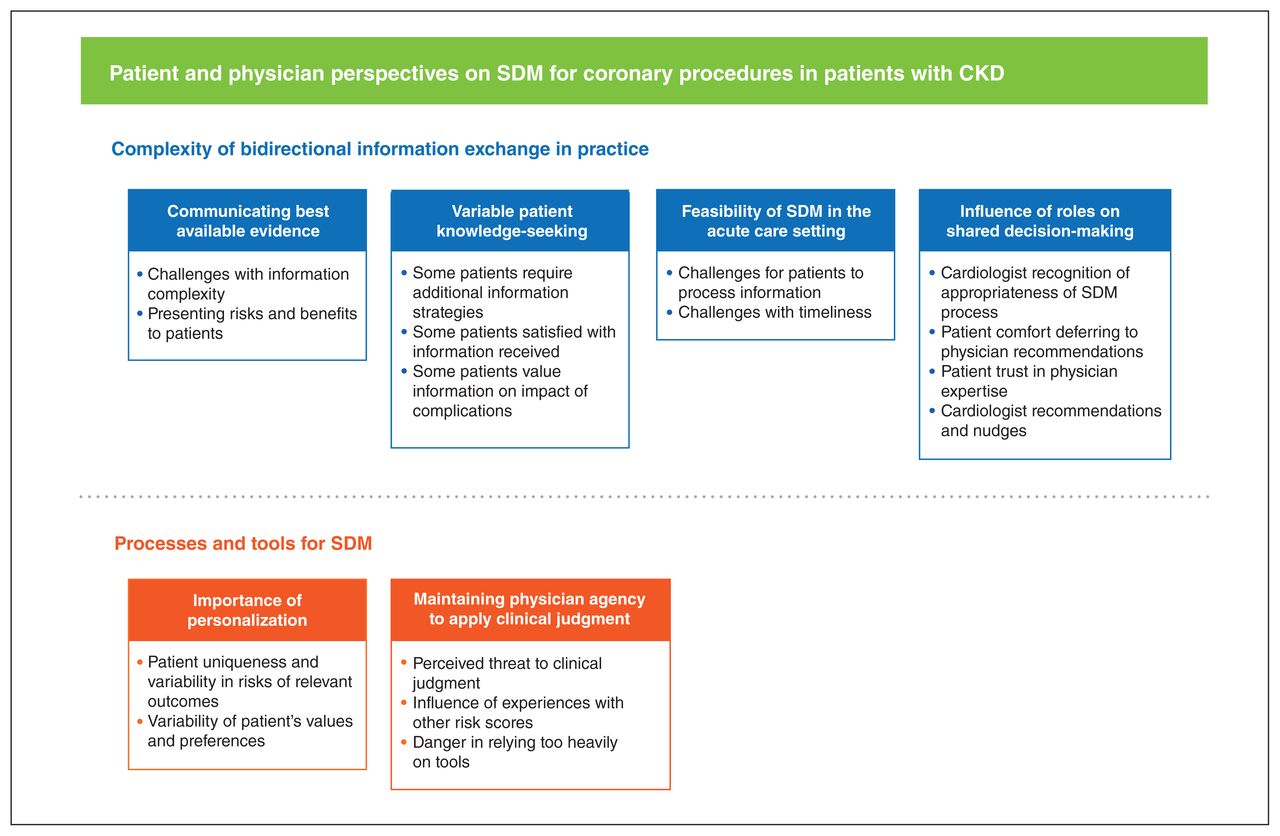
We categorized themes and subthemes according to current practices and perceptions of shared decision-making, and recommendations and challenges to be addressed for future development of decision aid tools (Figure 1). An overarching theme related to the complexity of bidirectional information exchange required to achieve shared decision-making in practice emerged from integration of both patients’ and cardiologists’ perceptions, whereas a second overarching theme about implementing processes and tools to support shared decision-making arose from cardiologists’ perspectives. Exemplar quotes are provided in Table 3.
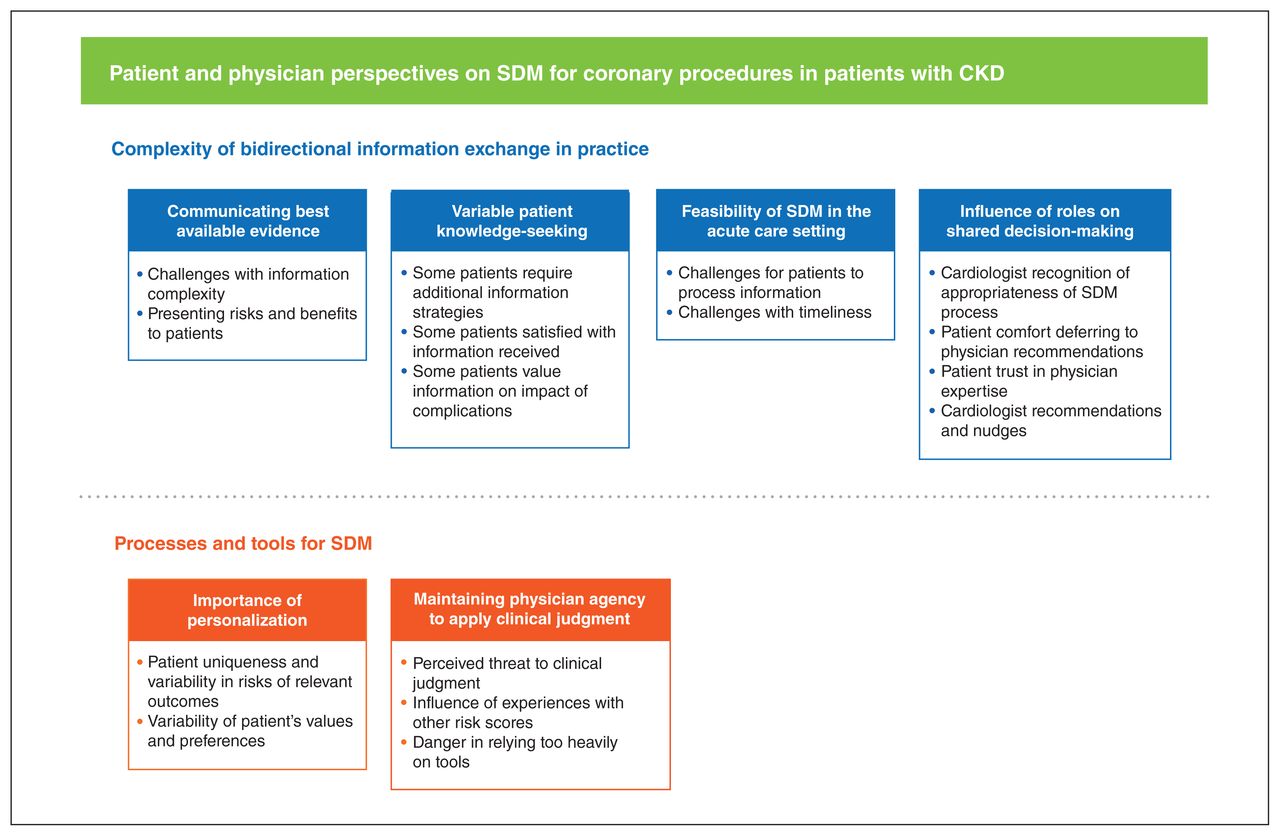
Major themes and subthemes identified from analysis of interviews with patients and physicians. Note: CKD = chronic kidney disease, SDM = shared decision-making.
Selected exemplar quotes from patients and physicians
Complexity of bidirectional information exchange
Communicating best available evidence
Cardiologists identified the complexity of the information provided in the discussion about invasive versus medical management as a challenge to practising shared decision-making. In an attempt to reduce the density of information provided to patients, cardiologists described simplification of their presentation of risks as “high, medium or low risk” of requiring dialysis “acutely” and “long term”. It was “often quite difficult for patients, particularly the elderly, to understand the risks.” Patients, too, said their understanding of the risks and benefits was limited. For patients, what was important was that the problem be fixed; that the cardiologist should “do what you need to do.”
Variable patient knowledge seeking
Although the cardiologists emphasized the volume of information they felt they needed to provide patients for shared decision-making, patients varied in their levels of knowledge seeking and desire for this information. Many stated they had been given all the information they needed to make an informed decision and were satisfied with the explanations the cardiologists provided. For those patients who wanted more information before making a treatment decision, some cardiologists identified additional steps they would take to meet their patient’s information needs, such as obtaining a consult from nephrology to discuss risk to kidney health.
Some patients who reported worsening kidney function after angiography said they would have wanted more information on these possibilities and risks and to be made aware of the impact that being on dialysis would have on their lives.
Feasibility of shared decision-making in the acute care setting
Both patients who had experienced ACS and cardiologists spoke about the difficulty of practising shared decision-making in the face of a stressful, life-threatening acute condition. Cardiologists acknowledged the impact of patients needing more information and discussion time. They spoke of the possibility that delayed decision-making might increase the potential risk of adverse effects while the patient was trying to decide. Nonetheless, cardiologists described the importance of scaling information appropriately, giving patients the opportunity to ask questions, and proving sufficient time to digest information.
Patients, too, spoke about limitations in their own ability to process information, of being “pretty sure” they knew what was happening, but not “100%.” Patients were aware time was a factor. Some patients perceived that decisions were primarily made by their care providers, but acknowledged they were still provided with information and explanations.
Influence of roles on shared decision-making
Several patients perceived that they “didn’t really make the decision” or they “went along with” the cardiologist’s recommendation. This was attributed to patient perceptions of the cardiologist as the expert and the comfort patients expressed in thinking “the doctor should decide.” Patients spoke about trust in the expertise of the cardiologist, and confidence that any actions taken by the cardiologist would result in the best care.
Cardiologists acknowledged that they provided nudges in one direction or another, providing the patient with recommendations as to which option they felt would be most appropriate. Cardiologists described providing “a recommendation as to which one I feel would be medically the most appropriate,” and in particular that “when you are at clear ends of the spectrum you tend to encourage.” Nudges, however, did not eliminate the importance of a discussion, from the cardiologists’ perspectives. Cardiologists were particularly open to patient input in situations of equipoise in the decision when “the patient’s voice becomes much louder” and cardiologists endorsed a greater dependence on their patient’s values and preferences.
Processes and tools for shared decision-making
Importance of personalization
Cardiologist emphasized potential value to improved processes and tools such as risk scores and decision aids to support shared decision-making. Importantly, they felt these should address patient uniqueness, based on different risk factors for relevant outcomes, and to help support a shared understanding of patient values and preferences.
Cardiologists spoke about each patient as a “complete individual,” and of the many considerations that factor into their recommendations. Cardiologists considered a wide range of individual factors, including the patient’s age, comorbidities, current level of kidney function, potential to benefit from revascularization and the patient’s treatment preferences. Cardiologists reported they placed “particular importance on the patient’s kidney disease,” and whether the patient recognized that dialysis was a possible outcome.
Maintaining physician agency to apply clinical judgment
Cardiologists were concerned that implementing processes and tools to support shared decision-making could threaten their agency in using their clinical judgment when recommending a course of action with patients. This perspective was influenced by their experiences using other risk tools available to them in cardiology. They expressed preference to evaluate the situation by meeting each patient and determining whether tools would be helpful with that particular patient to determine their risk.
Cardiologists expressed caution against overreliance on tools. Cardiologists did not want “the decision completely taken out of their hands” and were concerned about the potential to depend on risk estimates and then not use their clinical judgment or “look at the patient as a whole.”
Interpretation
Both patients with kidney disease and cardiologists recognize the desirability of shared decision-making when deciding whether or not to select invasive management for ACS or another cardiac indication.7,8 However, cardiologists and patients identify several challenges in practice, particularly with respect to complexities of bidirectional information exchange in this acute context. This setting poses challenges for physicians in how they communicate risk information and for patients in their ability to process information quickly and under duress of illness, understand terminology regarding procedures, and understand the meaning of being at risk.22,23 Despite some feeling that they had limited influence on the decision, patients identified trust in their physician, and respect for the cardiologist’s expertise and guidance as key to their confidence in decision-making. Cardiologists indicated that processes developed to support shared decision-making in this setting need to allow for physician agency and clinical judgment, and that decision aids (tools to support shared decision-making) need to address the individualization of patients in assessment of risks and consideration of patient values and preferences.
Our findings add to evolving knowledge on the practice of shared decision-making in acute cardiac care. Three factors that determine the appropriateness of shared decision-making include clinical equipoise, the patient being capable of making a decision and that sufficient time is available.24 We found that cardiologists placed greater value on their patient’s voice when they were less certain about whether net benefits exceeded risk for their patients with CKD. This finding may reflect the challenges physicians face to individualize the risks and benefits to individuals with CKD in this setting. Better information strategies may be needed to apply knowledge in this setting,4–6,8 as shared decision-making can be most valuable when the information needed to understand risks and benefits is available.25 Additional tools such as decision aids were perceived as a potentially useful strategy to address these barriers by reducing the time it takes to determine and communicate risks and benefits, while increasing patient understanding, provided they support physician and patient agency over the final clinical decision.
Other studies exploring shared decision-making in emergency care settings have found that although patients place high value on the opinion and expertise of the physician, they either wanted some degree of involvement in decision-making, or would have benefited from involvement.26,27 Our findings highlight similar needs to develop processes and tools that address individual patient values, ensure timeliness of decision-making and respect cardiologist expertise and judgment within the shared decision-making framework in this setting.
The findings of our study have implications for clinical practice of shared decision-making for ACS, and for future researchers and health policy-makers interested in developing processes and tools to support shared decision-making in this context. Our findings suggest that strategies and tools for shared decision-making in this setting should be tailored to patient uniqueness and variability in values and preferences, and incorporate physician agency and clinical judgment, which were perceived as important by both patients and physicians.
Future strategies in this area could focus on developing decision-aids that provide individualized information about the risks of kidney and heart disease outcomes, and include information on the impact of these outcomes, such as the need for temporary or permanent dialysis on quality of life. Given the important role that cardiologists play in guiding these decisions, physicians should be a target for training on the practice shared-decision making and use of decision-aids with patients.
Limitations
Our study included the perspectives of both patients and physicians, and representative recruitment ensured that we heard from patients without adverse events, and some who experienced kidney complications, including kidney failure requiring dialysis after invasive coronary procedures. However, there are some limitations to the study.
First, findings reflect only those of general decision-making experiences in the acute care context, so may not be similarly applicable to those who had unique decisional conflicts arise in their care. Second, our study was conducted at a single centre in Canada, which may have limited transferability to care in other regions and in other cultures. However, we included patients from rural and urban residences to address these groups’ perspectives, and participant demographic characteristics and care models from our study are similar to those elsewhere in Canada and other high-income countries. Third, patient participants were predominantly older men, so perspectives of women and younger patients with CKD were underrepresented. Fourth, we included 2 groups of patients with CKD; those who had ACS in the past year and those who had coronary catheterization for an indication not related to ACS; however, we did not distinguish whether patient and physician perspectives differed in those 2 scenarios. Finally, we recognize that patient experiences were likely influenced by how their own care providers practised, and this study cannot answer how patient experiences, decisional conflict and their preferences would be influenced by different clinical decision-making approaches. Alternative study designs are required to understand how patients’ preferences may vary, and the impact that processes and tools to support shared decision-making may have on their experiences with care.
Lessons learned from patient engagement
We used a patient-oriented research approach based on the Canadian Institutes of Health Research Patient Engagement Framework16 and benefited from the lived experience of our patient partners with CKD and heart disease. Involving them from the start of the design of the study helped us to tailor our study questions and materials to our patient study population, and reviewing the analysis of interviews with them strengthened our confidence in the relevance of the themes that emerged from the research. Although working with our patient partners required additional time and planning, we were better able to synthesize findings and identify implications for improved future care from both the patient and physician perspective, which is fundamental to the practice of shared decision-making. Patient partners have also played an active role in dissemination of our findings to other researchers, clinicians and policy-makers attending an annual CKD meeting.
Conclusion
We identified several complexities related to bidirectional information exchange needed for shared decision-making about coronary procedures between patients with CKD and their physicians, including variable patient knowledge seeking and feasibility in acute care. Processes and tools to support shared decision-making in this setting should be personalized to reflect variability of risks and patient preferences and allow physicians to maintain their agency and contribute clinical judgment.
Acknowledgements
The authors thank their patient partners and research participants for their time and for sharing their perspectives. The authors acknowledge Corri Robb for assistance with transcription. Matthew James was supported by a CIHR New Investigator Award.
Footnotes
Competing interests: Matthew James has received investigator-initiated research grant funding for unrelated work from Amgen Canada. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All authors in this study have contributed to this manuscript and approve of this submission. Juli Finlay, Pantea Javaheri, Todd Wilson, Carol Connolly, Winnie Pearson and Matthew James contributed to the study design, collected and analyzed the data, and drafted the article. All authors contributed to the design and provided critical important intellectual content to revisions to this manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by a Strategy for Patient-Oriented Research (SPOR) Chronic Disease Network Grant: Can-SOLVE Chronic Kidney Disease Network, from the Canadian Institutes of Health Research (CIHR).
Data sharing: Data available on request from the corresponding author.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/4/E860/suppl/DC1
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools





