


Article Figures & Tables
Figures
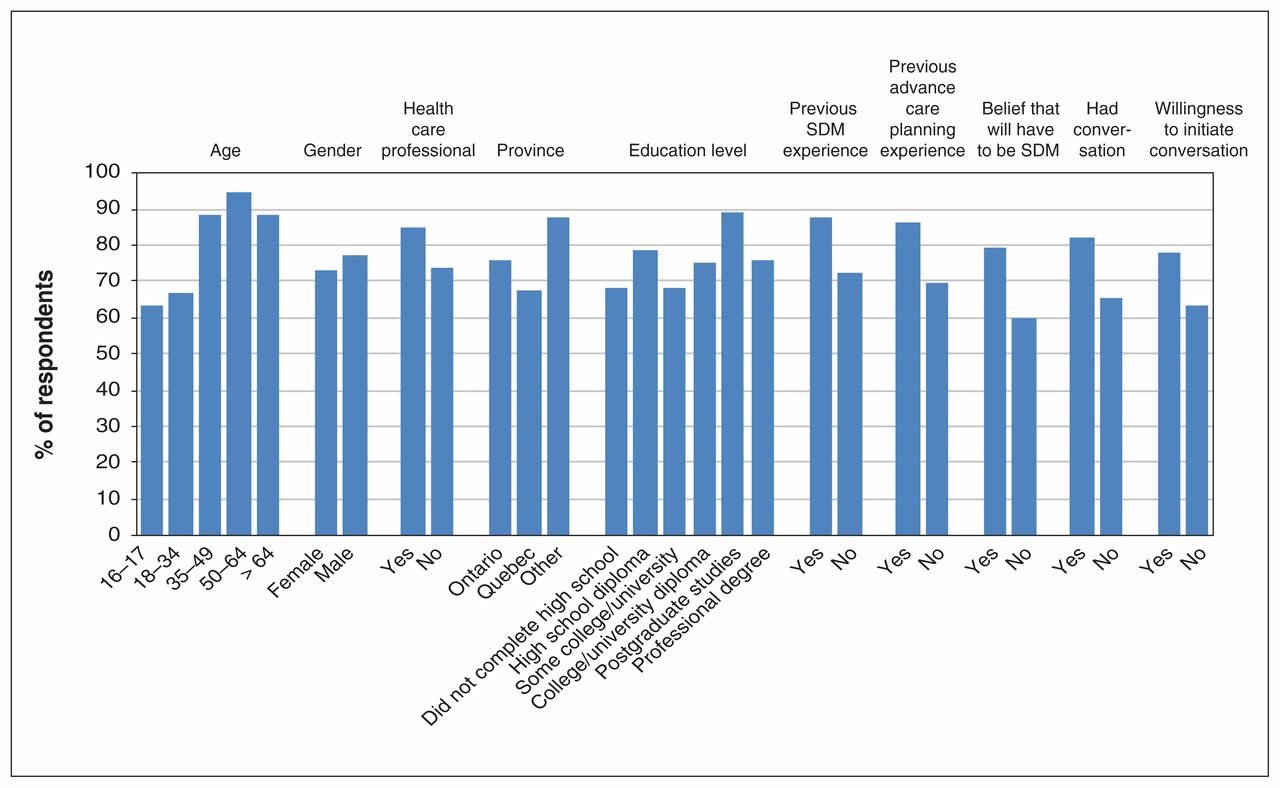
- Figure 1:
Rates of self-reported preparedness to be a substitute decision-maker (SDM) for a loved one with a critical illness, by demographic characteristics and selected predictor variables. Note: conversation refers to conversation regarding the wishes of loved ones in the event of critical illness or end of life.
- Figure 2:
Rates of belief that 16-year-old students should learn about being a substitute decision-maker (SDM) in the context of critical illness. Note: conversation refers to conversation regarding wishes of loved ones in the event of critical illness or end of life.

Tables
Characteristic No. (%) of respondents
n = 430Age, yr 16–17 23 (5.3) 18–34 253 (58.8) 35–49 62 (14.4) 50–64 53 (12.3) > 64 36 (8.4) Missing 3 (0.7) Gender Female 243 (56.5) Male 186 (43.3) Other 1 (0.2) Health care professional 34 (7.9) Province of residence Ontario 364 (84.6) Quebec 52 (12.1) Other 8 (1.9) Missing 6 (1.4) Education Did not complete high school 20 (4.6) High school diploma 49 (11.4) Some college/university 124 (28.8) College/university diploma 166 (38.6) Working on/completed postgraduate studies 48 (11.2) Professional degree 21 (4.9) Missing 2 (0.5) Previously acted as substitute decision-maker 67 (15.6) Previously created advance care plan for self 137 (31.9) - Table 2:
Logistic regression models identifying associations with preparedness to act as a substitute decision-maker and acceptability of high school education around substitute decision-making and critical care
Variable OR (95% CI) Self-reported preparedness to act as substitute decision-maker for adult loved one Belief that 16-year-olds should learn about resuscitation and end of life Age, yr 16–17 Reference Reference 18–34 1.13 (0.30–4.17) 0.11 (0.01–1.16) 35–49 3.29 (0.69–15.57) 0.07 (0.01–0.78) 50–64 7.46 (1.25–44.51) 0.10 (0.01–1.08) > 64 3.44 (0.64–18.52) 0.11 (0.01–1.23) Gender Female Reference Reference Male 1.64 (0.98–2.74) 1.16 (0.71–1.89) Health care professional Yes 1.74 (0.53–5.75) 0.67 (0.28–1.59) No Reference Reference Province Ontario Reference Reference Quebec 0.53 (0.26–1.08) 1.02 (0.50–2.07) Other 1.70 (0.19–15.14) 1.16 (0.20–6.87) Education Did not complete high school Reference Reference High school diploma 0.76 (0.18–3.24) 1.30 (0.20–8.62) Some college/university 0.86 (0.20–3.70) 1.01 (0.16–6.23) College/university diploma 0.66 (0.15–2.90) 1.22 (0.20–7.52) Working on or completed postgraduate studies 1.46 (0.25–8.43) 0.90 (0.13–6.02) Professional degree 0.35 (0.05–2.29) 1.24 (0.15–10.11) Previously acted as substitute decision-maker 0.98 (0.37–2.57) 0.77 (0.37–1.60) Previously participated in advance care planning for self 2.01 (1.06–3.83) 1.71 (0.96–3.07) Belief that one will have to act as substitute decision-maker 2.36 (1.34–4.17) 1.90 (1.07–3.37) Had previous conversation with loved ones about wishes in critical illness 1.23 (0.72–2.08) 1.20 (0.72–2.01) Willing to initiate conversation with loved ones about wishes in critical illness 1.47 (0.84–2.57) – Belief that having conversation with loved ones about wishes in critical illness is learnable skill – 2.57 (1.37–4.80) Self-reported preparedness – 0.98 (0.55–1.74) Note: CI = confidence interval, OR = odds ratio.
- Table 3:
Self-reported enablers of and barriers to preparedness to be a substitute decision-maker
Theme Subtheme Representative quotation Real-life experience Difficulty in knowing how to prepare oneself “My mother had advanced dementia. When [she died], we did not know what to expect. We wanted her to be comfortable, but she didn’t look comfortable [when she died]. If we had known how difficult it would be to watch [cardiopulmonary resuscitation], we would have stopped. [We need] more guidelines on how to prepare oneself. What questions to ask a parent. We thought we were prepared and we weren’t. ... We really didn’t know what questions to ask.” (62 yr-old woman [describing her experience with changing the code status of her parent from Do not resuscitate to full code as she died]) Information necessary for decision-making Understanding preexisting wishes through such means as conversation, living wills “I watched my dad go through this with my grandfather and he had Alzheimer’s, but they had discussed this sort of things beforehand, so it made things a lot easier on him because he already knew what my grandfather wanted and how to handle the situation.” (31-yr-old man) Understanding role of SDM Understanding capacity and SDM legislation
Clarity regarding who legal SDM is Voluntary nature of being SDM
No secondary gain“Need to have legal rights [explained], especially if you were to come [to] odds with the medical team.” (47-yr-old man) “It’s not clear what we expect from the SDM — it’s important to know and understand the different options that are available to help guide the SDM.” (66-yr-old man) Relationships among SDM/patient/family Fear of family conflict and social pressures
Family consensus“We [made] some bad decisions for my mother trying to keep some of my siblings happy. … Experience is a huge factor in empathy and understanding, and differentiating between what a loved one is saying and what [he or she] needs.” (62-yr-old woman) Attributes of SDM Maturity, strong value system
Willingness to separate personal and loved one’s values
Previous life experience
Ability to act rationally despite distress of situation“[You] need to be a good listener so you can understand the situation, need to be considerate of what the loved one would want, need to be rational and not too emotional.” (42-yr-old woman) Relationship with medical team Need for clear communication of medical information: prognosis regarding quality of life; risks, benefits and alternatives of treatments Trusting relationship with medical team “My mother didn’t have a [power of attorney] in place before getting sick and I was the SDM, but the health care team treated me as if they didn’t think I had a right to be making decisions, so this made it very difficult. I had to advocate on her behalf to the medical team.” (64-yr-old woman, health care professional) External influences on SDM Social and cultural barriers to communication
Need for time and quiet setting
Previous training“I am more open than the rest of my family to having conversations about end of life. Every time I try to initiate conversations about their wishes, they stop me. They are not open to discussing these kinds of things.” (51-yr-old woman) Fears Fear of guilt after decision
High stakes/burden of responsibility“[Barriers include the] uncertainty of you making the final decision for someone else … [and the] responsibility of living with that decision for the rest of your life. (40-yr-old man) Note: SDM = substitute decision-maker.
Theme Subtheme Representative quotation Age appropriateness Existing experience within families
Legal right denotes societal responsibility to prepare
Cognitive and emotional maturity
Subset of immature students who may not be ready“I agree because I think that if someone can legally make a decision, [he or she] should know all the information that comes with that right. People are taught about sex at 14; this is just as important, and they are mature enough to understand this as well.” (18-yr-old woman)
“Some 16-year-olds are pretty immature, and they would have to be mature to be taught this.” (82-yr-old woman, health care professional)Developmental benefit Improved decision-making
Increased sense of responsibility and maturity
Development of personal beliefs“By 16 they understand that death happens. … They will walk out of learning this and have bigger conversations with their friends and family about this topic.” (49-yr-old woman) Decreases stress/distress at time of decision Unpredictability in timing of real-life situation “I had to make these decisions as a 24-year-old. My mom, as a health care provider, always let me know what she wanted. From when I was young (10 and onwards) I felt equipped to support her and her decisions when the time came regardless of my personal feelings.” (43-yr-old woman) Societal benefit Universal issue — awareness needed
Breaking taboos
Taking care of parents“It’s like sex ed — are you going to hide it from them? It’s important to have these conversations because they can be put in this situation at any time. If you see your parents going through it you might wonder what’s going on, so it’s good to be educated on this topic. It shouldn’t be a taboo subject.” (66-yr-old man) Potential difficulties/harm in selected students Mandatory v. opt in v. opt out “People are having kids later these days, and this could come up sooner in a person’s life. Someone could be an only child and would need this [information]. No one is ever prepared for the psychological and emotional stress that comes with this.” (47-yr-old man) Risk of bias Teacher and facilitator dependent “[You] have to consider religious [implications], family members, customs, language and country of origin.” (82-yr-old woman, health care professional)
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.