


Abstract
Background: Follow-up with a primary care provider within 1–2 weeks of discharge from hospital has been associated with reduced readmissions. We sought to determine appointment attendance with primary care providers postdischarge and identify factors associated with attendance.
Methods: We conducted a retrospective cohort study involving general medicine patients who had been discharged from hospital between Sept. 1, 2014, and Dec. 30, 2015, from 2 Ontario academic hospitals, and who had been supported by a transitional care specialist and advised to see a primary care provider within 1 week. Attendance was determined by self-report during follow-up by telephone. We used multivariable logistic regression to assess whether patient factors (e.g., comorbidity) or system factors (e.g., booking the appointment before discharge) predicted attendance. We used Cox proportional hazards modelling to assess whether attendance predicted readmission within 30 days.
Results: Of the 214 patients included in our study, 35% (n = 75) attended a primary care appointment within 1 week of discharge; 52% (n = 124) of patients attended an appointment within 2 weeks. After adjusting for age, sex and comorbidity, significant predictors of attendance were booking the appointment before discharge (odds ratio [OR] 2.14, 95% confidence interval [CI] 1.07–4.40), familiarity with the primary care provider (OR 5.43, 95% CI 2.25–14.1) and inclusion of a reminder, callback number and appointment time in the discharge summary (OR 15.3, 95% CI 2.09–326). Predictors of nonattendance were the presence of a home support worker (OR 0.38, 95% CI 0.17–0.80) and a booked specialist appointment before discharge (OR 0.37, 95% CI 0.18–0.73). Attendance was not associated with reduced readmissions (hazard ratio 0.66, 95% CI 0.40–1.09).
Interpretation: Timely follow-up with PCPs postdischarge remains challenging. Efforts to improve attendance should focus on reinforcing need for follow-up and coordinating follow-up before discharge, particularly for those poorly connected with the health care system.
With pressure to discharge patients sooner,1,2 coordinating prompt follow-up with primary care providers after discharge has become essential to ensure continuity of care and a safe patient transition. Although controversy remains over whether prompt primary care follow-up is of benefit to all medical patients,3–6 some studies have found that such care reduces emergency department visits and readmissions7–9 among patients with conditions such as congestive heart failure, chronic obstructive pulmonary disease (COPD), non-ST elevation myocardial infarction (NSTEMI) and cancer.10–13 Several provincial and national organizations therefore recommend follow-up within 1–2 weeks of hospital discharge as a measure of health care quality,14–17 and local initiatives, interventions and incentive structures in both Canada and the United States have been developed to improve the discharge and follow-up process to meet these quality standards.18–22
Despite recommendations and attempts to improve attendance, prompt follow-up within 1–2 weeks of discharge remains a challenge. In Canada, 1-week follow-up rates vary between 32% and 56% depending on clinical condition and region.14,18 National Medicare claims data suggest rates are similar in the US.23 Several contributory factors have been postulated. Patients self-report forgetfulness, miscommunication and logistical barriers.24–26 Studies have shown age, socioeconomic status and rural residence produce inequities in access to primary care.4,14,23,27 Attendance is likely dependent on a combination of predisposing patient factors (clinical and functional) and system resources such as ease of booking and transportation,28 but few studies have looked comprehensively at how these factors may contribute together to attendance at appointments after discharge. Better evidence is needed to inform quality improvement projects on transitional care.
The objective of our study was to determine self-reported attendance rates with primary care providers after discharge from hospital and to identify patient and system factors associated with attendance.
Methods
We conducted a retrospective cohort study that involved patients who had been discharged from the general medicine ward of 2 academic hospitals (Toronto General Hospital and Toronto Western Hospital, Toronto) between September 2014 and December 2015. The decision to discharge patients was at the discretion of the attending staff. All study participants were seen in hospital by a transitional care specialist before discharge who advised them to see their primary care provider within 7 days of discharge.
The transitional care specialist could receive referrals from any health care professional attending on the hospital unit for patients felt to be at high risk of readmission or in need of a primary care provider for postdischarge follow-up. There were no standardized criteria for referral; the transitional care specialist decided whether patients would benefit from their involvement. Their responsibilities included ensuring access to a primary care provider or home care services if needed, educating the patient about the discharge plan, and ensuring the transmission of the discharge summary to the primary care provider. The transitional care specialists advised all patients to see their primary care provider within 7 days, but did so without following a specific script, because reasons for follow-up postdischarge were heterogeneous and patient-specific. The specialists followed up with patients by telephone within 14 days and recorded whether they had attended an appointment with a primary care provider, in addition to any postdischarge issues, through an unstructured interview.
Data sources
The records of the transitional care specialist served as the primary source of our data. We subsequently verified and supplemented the data by manual chart review completed by the primary author (K.L.) using data from the electronic medical record of both hospitals (QuadraMed, Harris Healthcare). A 25% sample of the data collected was verified by a research assistant to ensure consistency between what was collected by the primary author, the transitional care specialist, and the electronic medical record. Overall agreement was 89.7%, and discrepancies were resolved by consensus on repeat review. From this initial cohort, we excluded patients who had died in hospital, who had been discharged to another care facility, who were at end of life and had been referred for palliative care in the community, or who could not be reached (patients with no contact information, who had left against medical advice or who had refused follow-up), because these changed the conditions for postdischarge follow-up. We excluded patients being seen by primary care providers in their homes or enrolled in other quality improvement initiatives or research projects intended to facilitate visits by primary care providers because of the risk of introducing unknown and unmeasured biases from among these individuals. When patients had been admitted multiple times, we only included the first admission; our unit of analysis was the patient rather than the discharge to better identify patient-level characteristics.
Covariates
We a priori generated a list of covariates that could affect attendance postdischarge following Andersen’s model of health care behaviour28 and added variables that affect the risk of readmission.29 We categorized covariates as patient characteristics if they were related to patients’ clinical status, utilization or functional status, and as system-related characteristics if they were related to the process of discharge. The first author (K.L.) reviewed the electronic health record for baseline characteristics including age, sex, presence of language barrier, discharge diagnosis and Charlson Comorbidity Index using diagnoses listed in the discharge summary.30 We recorded presence of psychiatric comorbidity, substance use disorders, cognitive impairment (diagnosis of dementia or positive on documented cognitive screening), mobility impairment (use of cane, walker or wheelchair), social isolation (living alone and without inpatient visitors) and discharge home with support services. We included other characteristics that may have affected baseline health care access and use, such as length of stay and visits to the emergency department in the previous 6 months.
System-related variables that may have affected attendance included whether the primary care appointment was booked before discharge, whether the transitional care specialist helped with booking the appointment, the time to follow-up appointment and whether discharge occurred on a weekend (Saturday or Sunday). We documented primary care provider familiarity if the patient reported access to a primary care provider We documented whether the patient requested a new primary care provider. We also noted whether a specialist appointment was booked before discharge. Finally, we recorded whether the discharge summary provided appointment details such as appointment time and a phone number to call should questions arise.
Outcomes
Attendance at a primary care appointment was based on self-report and classified as attended, not attended or unknown. We considered missed appointments as not attended and, when available, recorded the reason for not attending. In addition, we classified rescheduled appointments as not attended, because we had no standardized way of knowing if all rescheduled appointments were later attended. We excluded patients for whom follow-up appointment attendance was unknown. We recorded readmissions or visits to the emergency department to either hospital within 30 days after discharge. Information on visits to the emergency department or readmission to other hospitals was not available, and therefore could not be included.
Statistical analyses
We compared all baseline characteristics between attendees and nonattendees using χ2 and t tests, and calculated unadjusted odds ratios (ORs) for each. We used stepwise multivariable logistic regression to identify independent predictors of postdischarge primary care attendance. We chose the most parsimonious model based on a bidirectional step Akaike information criterion (AIC) modelling procedure, and further included age, sex and comorbidity to produce our final model. For each variable in the final model, we report the ORs for attendance with 95% confidence intervals (CIs), in addition to the 2-tailed Wald test p value against the null hypothesis that the true OR equals 1. We used the rule of thumb of 10 events per predictor variable to assess whether we had a sufficient number of events to reliably fit the number of predictors in our final model.31 We assessed multicollinearity using variance inflation factors using a threshold value of 2 as evidence of meaningful correlation. We performed sensitivity analyses by assigning patients with unknown outcome to either attended or not and repeating the above analyses. We used Cox proportional hazards modelling to assess the hazard ratio (HR) between nonattendance and the risk of readmission, adjusted for age, sex, length of stay, comorbidity and previous visits to the emergency department. In all analyses, we used α = 0.05 as the threshold for significance. Analyses were performed using R version 3.3.2 (The R Foundation for Statistical Computing).
Ethics approval
Ethics approval was obtained from the institutional review board of University Health Network in Toronto.
Results
Of 552 eligible patients, 300 met our initial inclusion criteria. Of these patients, we excluded 86 (29%) for whom attendance was unknown, for a final study population of 214 (Figure 1).
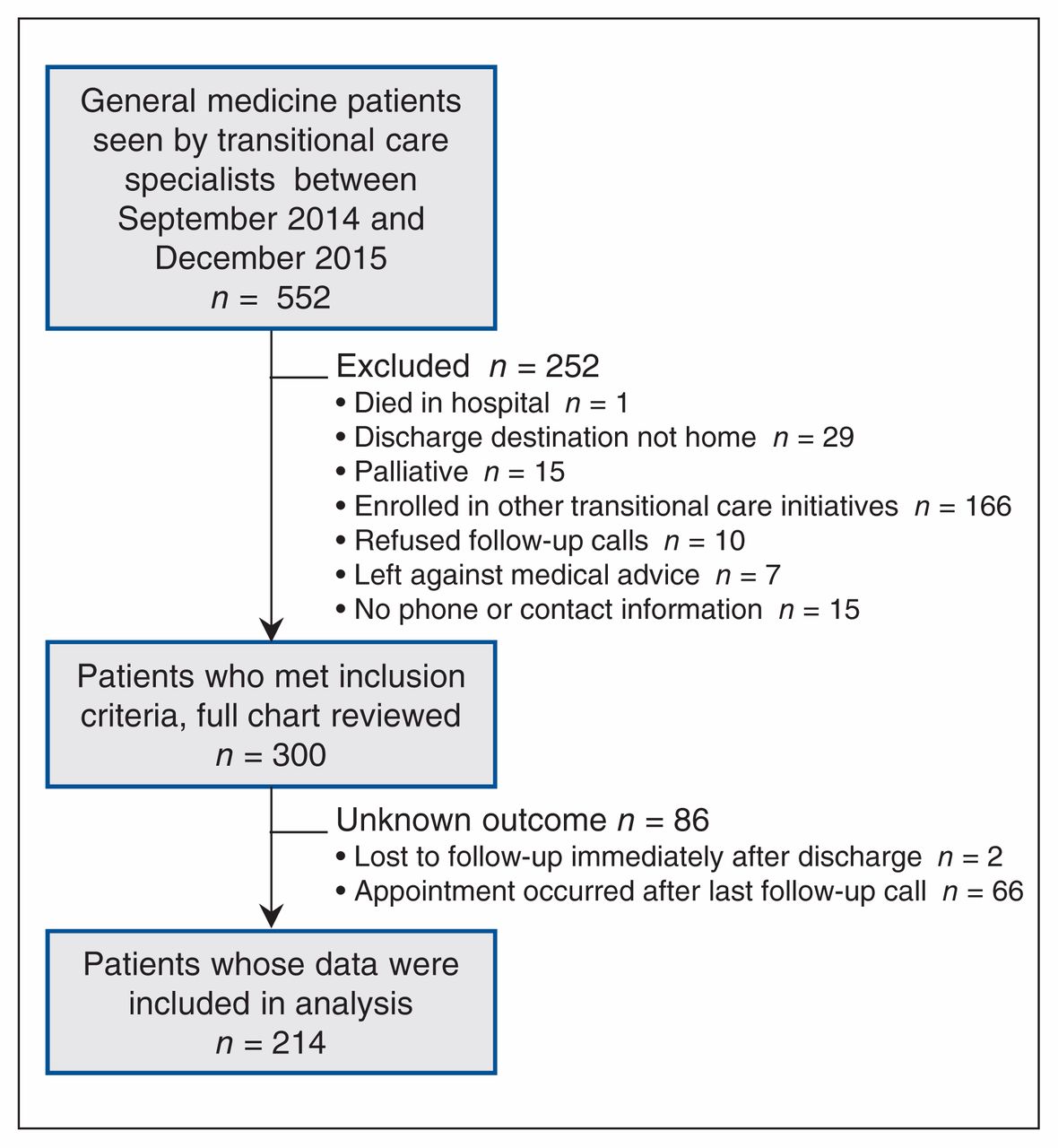
Flow of patients through the study.
Baseline characteristics of the study population are provided (Table 1). The median age was 72.5 years and 57% of patients were male. The most common discharge diagnoses were acute decompensated heart failure (19%), community acquired pneumonia (8.7%) and acute exacerbations of COPD (7.5%). The transitional care specialist followed patients for amean of 11.5 (± 8.5) days (median 10 d) postdischarge. A total of 168 primary care appointments were scheduled for a mean of 7.3 (± 5.3) days after discharge. Only 90 patients (42%) received a follow-up appointment within 7 days. At baseline, there were no significant differences in characteristics of patients who attended and patients who did not attend their primary care appointment.
Baseline characteristics of discharged medical patients categorized by attendance at primary care appointments
We identified 124 patients (58%) who attended their appointment, 75 (35%) within the first week of discharge and 112 (52%) within 2 weeks of discharge. Seventeen appointments (8%) had been rescheduled, and were thus classified as not attended. We identified 4 system-related factors associated with attendance on baseline pairwise comparison and in our final model: having an appointment booked before discharge (OR 2.14, 95% CI 1.07–4.40), a familiar primary care provider (OR 5.43, 95% CI 2.25–14.1) and a discharge summary with both appointment time and callback number (OR 15.3, 95% CI 2.09–326) were positively correlated with attendance, whereas having a specialist appointment booked before discharge (OR 0.37, 95% CI 0.18–0.73) was negatively associated with attendance (Table 2). In the final model, the presence of a home support worker (OR 0.38, 95% CI 0.17–0.80) emerged as negatively associated with attendance. Variance inflation factors for all variables in the final model were less than 2 (Appendix 1 available at www.cmajopen.ca/content/6/4/E587/suppl/DC1). For the 90 patients who did not attend their appointment, reasons for nonattendance were available for 78 (86%) of them. The reasons given included patient-related factors such as feeling an appointment was unnecessary (28%), forgetting to book or attend (17%), scheduling conflicts (12%), being readmitted at the time of the appointment (10%) or feeling unwell (4%); system-related factors included transportation difficulties (21%) and physician unavailability (10%).
Factors associated with attendance at postdischarge primary care appointment after stepwise regression,* adjusted for age, sex and Charlson Comorbidity Index
A total of 66 patients (31%) were readmitted to hospital within 30 days. For these patients, the mean time to readmission was a12.8 (± 8.0) days (median 12 d) after discharge. After adjusting for age, sex, length of stay, comorbidity and recent visits to the emergency department, the risk of readmission within 30 days was not significantly lower for patients who attended their primary care appointment (HR 0.66, 95% CI 0.40–1.09) (Figure 2, Table 3).
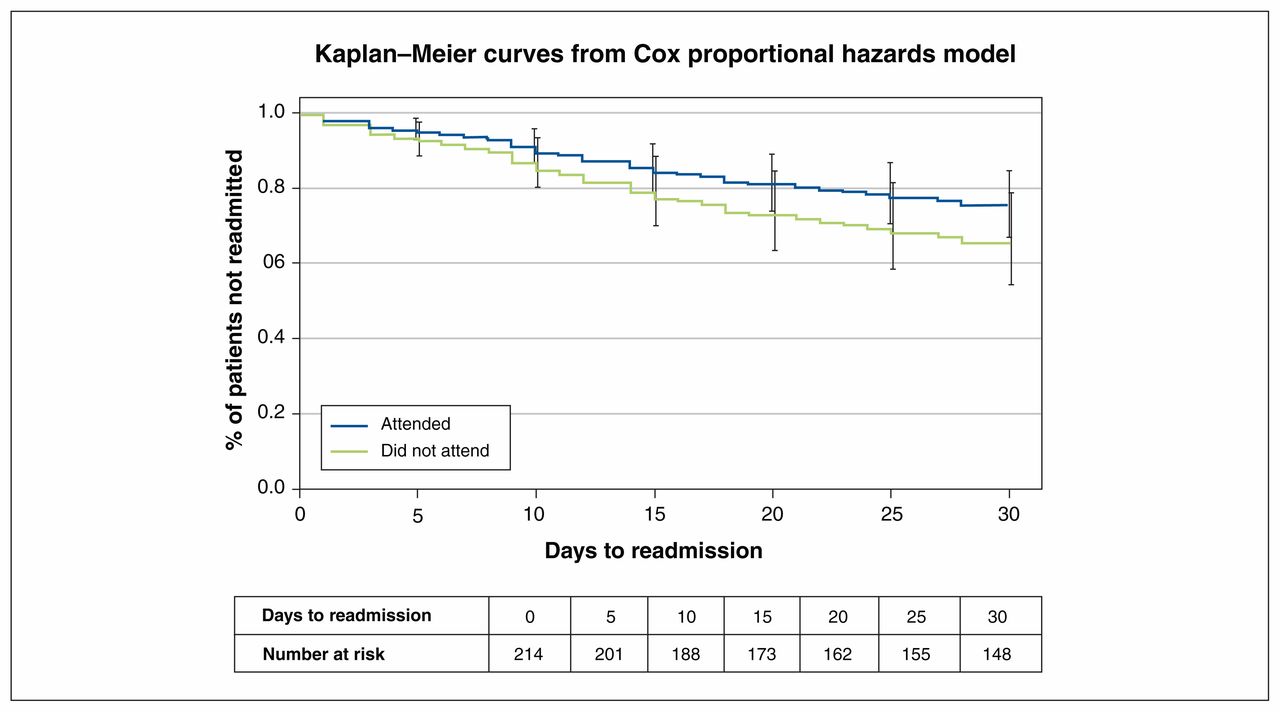
Kaplan–Meier curves for time to readmission for patients by attendance at a primnary care appointment. Models were adjusted for age, sex, Charlson Comorbidity Index, length of stay, and visits to the emergency department in the previous 6 months. Error bars indicate 95% confidence intervals.
Results of Cox proportional hazards model for readmission for patients by attendance at primary care follow-up
Sensitivity analyses
Patients with unknown attendance (n = 86) (Appendix 1) had more visits to the emergency department in the previous 6 months, were more likely to have cognitive impairment or a psychiatric diagnosis, were less likely to have their primary care appointment booked before discharge, and their discharge summaries were less likely to contain a follow-up appointment time. When unknown attendance was considered as not attended, the presence of a home support worker was no longer an independent predictor of attendance. When unknown attendance was considered as attended, booking before discharge was no longer predictive of attendance. Primary care provider familiarity, having a specialist appointment booked before discharge and providing an appointment reminder with callback number and time retained significance in both sensitivity analyses (Appendix 1).
Interpretation
Achieving prompt follow-up after discharge continued to be a substantial challenge for our study cohort. Only 35% of patients attended their primary care appointment within 1 week of discharge, and only 52% attended within 2 weeks. After adjusting for baseline demographic differences, attendance was positively associated with having an appointment booked before discharge, having a provider known to the patient and having a written reminder for the appointment in the discharge summary, and was negatively associated with the presence of a booked specialist appointment at discharge and the presence of a home support worker. Attendance at a primary care appointment was not associated with 30-day readmission. These findings suggest specific system changes may improve rates of prompt follow-up with primary care providers.
The follow-up rate for our cohort was low, yet similar to previous data from Canada and the US. The 7-day follow-up rate with any doctor was 36% for patients with COPD and 46% for patients with heart failure in Ontario,18 32%–37% for all medical and surgical discharges in Alberta and Saskatchewan,14 and 27% among 3 661 older adult patients discharged from a general medicine ward in the US.4 We propose several reasons for the low attendance rates we saw. First, appointment availability continues to be a substantial obstacle. Even with the assistance of a transitional care specialist in finding and contacting primary care providers and booking appointments, only 90 patients (42%) received an appointment within 1 week. Most patients (83%) who received an early appointment attended; a program evaluation with perspectives from both the patient and provider is likely to further elucidate reasons for unbooked appointments. Second, our cohort consisted of patients with heterogeneous reasons for admission and need for postdischarge follow-up; this may explain why attendance rates were on par with others despite the help of transitional care specialists. Third, we suspect a mismatch between how patients and health care professionals perceive the importance of postdischarge appointments; patients with a booked specialist appointment may have been less likely to attend their primary care appointment because they deemed it unnecessary to see multiple doctors.24
Appointment attendance is a complex behaviour dictated by multiple interacting components such as patient health, perceived need for care, reminders and enabling resources.28 Our study highlights the relative importance of system-related characteristics rather than patient characteristics in predicting attendance. This supports other studies with similar findings, 14,32 and literature suggesting postdischarge follow-up can be improved with predischarge interventions. For example, a randomized trial found that booking itself increases follow-up rates by 22%,33 and a before–after study found that improving the information given to patients before appointments improved attendance.25 We found that having a specialist appointment booked before discharge was associated with lower rates of follow-up, which may be due to patients disinterest in seeing their primary care provider given an alternative appointment. A similar pattern was previously seen in a study of discharges from a neurosurgical ward, where patients referred elsewhere were less likely to attend a follow-up neuropsychiatric appointment.32
Limitations
We did not perform a sample size calculation. We conducted sensitivity analyses to explore how the unknown cohort could affect our results, and found that at least 3 system-related characteristics maintained significance in influencing attendance, although sample selection bias and overestimation of the effect size of our predictors owing to small sample size remain risks.
The transitional care specialist did not use standardized criteria for deciding who to follow nor did they use a standardized script for why attendance at the follow-up appointment was important. The role the transitional care specialist played in postdischarge attendance is therefore not known and cannot be inferred from this study.
Although recall bias was of lower risk given the short duration of time during which postdischarge attendance was determined, our outcome was based on self-report, and social desirability bias may have inflated reported attendance rates.
We classified rescheduled appointments as missed, although in practice, rescheduled appointments may be a tolerable outcome if the appointment is rescheduled soon thereafter. Our short duration of follow-up meant 29% of patients with an uncertain outcome were excluded from our analyses, mostly because of appointments being scheduled after the final call by the transitional care specialist.
Conclusion
Rates of prompt follow-up, even with the assistance of a transitional care specialist, fall short of provincial and national recommendations. The relative importance of system-related characteristics in predicting attendance suggests interventions that facilitate easy appointment-making may improve follow-up rates. As we move toward more patient-centred care, greater efforts should be made to consolidate and coordinate appointments between primary care providers and specialists to minimize unnecessary visits and missed appointments.
Acknowledgements
The authors acknowledge Agnes Kulinek and Jhiffee Locquaio for their work as transitional care specialists, without which this study would not be possible, and Amy Troup for her help validating our data.
Footnotes
Competing interests: Kenneth Lam reports receiving personal fees from Mavencare. Karen Okrainec sits on advisory committees for Health Quality Ontario on care transitions and is principal investigator for a study evaluating the affect of a patient-oriented discharge summary on patient experience and health care use after discharge. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Kenneth Lam contributed in the design, data collection and analysis, and interpretation of the study and the drafting and revisions of the manuscript. Howard Abrams contributed in the design and revision of the manuscript. John Matelski contributed to the data analysis and interpretation and revision of the manuscript. Karen Okrainec contributed in the design, data analysis and interpretation of the study and in revisions of the manuscript. All authors gave final approval of the manuscript prior to submission and agreed to act as guarantors of the results.
Funding: This research received no specific grant from any funding agency.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/6/4/E587/suppl/DC1.
References
- Copyright 2018, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools


