


Abstract
Background: Physicians have traditionally been at the forefront of medical research, bringing clinical questions to the laboratory and returning with ideas for treatment. However, we have anecdotally observed a decline in the popularity of basic science research among trainees. We hypothesized that fewer resident physicians have been pursuing basic science research training over time.
Methods: We examined records from residents in the Surgeon-Scientist and Clinician-Investigator programs at the University of Toronto (1987-2016). Research by residents was categorized independently by 2 raters as basic science, clinical epidemiology or education-related based on the title of the project, the name of the supervisor and Pubmed searches. The study population was divided into quintiles of time, and the proportion pursuing basic science training in each quintile was calculated.
Results: Agreement between the raters was 100%; the categorization of the research topic remained unclear in 9 cases. The proportion of trainees pursuing basic science training dropped by 60% from 1987 to 2016 (p = 0.005).
Interpretation: Significantly fewer residents in the Surgeon-Scientist and Clinician-Investigator Programs at the University of Toronto are pursuing training in the basic sciences as compared with previous years.
Fundamental scientific research forms the basis for advances in medicine,1 a relationship exemplified by remarkable and rapid progress in the treatment of HIV2 and various malignant diseases.3 Increased understanding of genomics and cellular physiology has created the prospect of "personalized medicine,"4 the notion of tailoring treatment to the specific needs of individual patients. Paradoxically, however, the possibility of personalized or precision medicine coincides with an apparent devaluing of fundamental research in the field of clinical medicine. We have recently documented the decline of basic research in top medical journals over the last 20 years,5 while the Canadian Institutes of Health Research have recently ended their long-standing financial support of MD/PhD programs.6 In parallel, we have anecdotally observed that fewer residents seem to be pursuing training in the basic sciences, which might have implications for the future involvement of physicians in precision medicine. To substantiate this impression, we examined cumulative data from the Clinician-Investigator Program at the University of Toronto, the largest university in Canada. This program allows resident physicians from specialties and subspecialties of the Royal College of Physicians and Surgeons of Canada to pursue research training and is the largest such program in the country. Many graduates go on to obtain academic faculty appointments throughout North America. We sought to determine whether the proportion of resident physicians pursuing training in basic science research has changed over the last 30 years.
Methods
Setting
At the University of Toronto, postgraduate residents pursuing a thesis-based graduate degree or a postdoctoral fellowship may apply for the Clinician-Investigator program, a program for training physician-scientists that is accredited by the Royal College of Physicians and Surgeons of Canada with a minimum 2-year duration. The program is the largest in Canada, and trainees may come from any specialty or subspecialty program (e.g., Medicine, Surgery, Pediatrics) of the college.
Design
We obtained data on all trainees from Clinician-Investigator program from 1993 to 2016. All students enrolled in the program are included in the database, and their projects are registered upon enrollment; only 1 research project was recorded per trainee. The years represent the year of enrollment. Data included the title of the project, the name of the supervisor and (in some cases) the name of the graduate department (e.g., the Institute of Health Policy, Management and Evaluation; Institute of Medical Sciences; Wilson Centre for Healthcare Education).
To obtain earlier historical data, we obtained similar records from the Surgeon-Scientist program from 1987 to 1992 for all trainees who enrolled in that time period. This program was run by the University of Toronto's Department of Surgery and predated the Clinician-Investigator program. An important caveat is that enrollees were exclusively surgical residents. Most of the program's trainees after 1992 were enrolled in the Clinician-Investigator program and are included in that cohort.
We categorized the type of research that was performed (e.g., basic science v. clinical epidemiology v. education) by reviewing the title of the project and the name of the supervisor, and confirmed the categorization by searching for publications by the trainee in PubMed; this process was performed separately by 2 raters (WLL and NMG) for the entire cohort. As the focus of this study was on basic science research, basic science was intentionally defined broadly to include any investigation dealing with the mechanisms of disease or therapy. In some cases, the location of the research (e.g., the Wilson Centre for Health Care Education) was used to help categorize the topic.
Statistical analysis
We divided the 30-year period into quintiles to minimize the effect of year-to-year fluctuations in the numbers of trainees and compared the proportion of residents performing basic science research in the first and last quintile by 2-tailed t test; we considered a p value of less than 0.05 as significant. As a control, we repeated this analysis after excluding the 1987-1992 data from the Surgeon-Scientist Program (i.e., by comparing the first quartile of the Clinician-Investigator program [1993-1998] to the last quartile [2011-2016]). In addition, we performed a χ2 test for trend on all quintiles.
Results
The cohort of trainees from the Clinician-Investigator Program (1993-2016) included 525 residents, whereas the earlier Surgeon-Scientist cohort included 58 residents, for a total cohort size of 583. As indicated earlier, most of the Surgeon-Scientist trainees from after 1992 are included in the Clinician-Investigator cohort, with about 51% of the Clinician-Investigator trainees (1993-2016) being from the Department of Surgery. The categorization of the research topic remained unclear in about 1.5% of the cohort (i.e., 9 residents out of 583), but agreement between the raters was 100%; these 9 residents were included in all analyses. For clarity, sample titles and their categorization are shown in Appendix 1 (available at www.cmajopen.ca/content/4/3/E444/suppl/DC1).
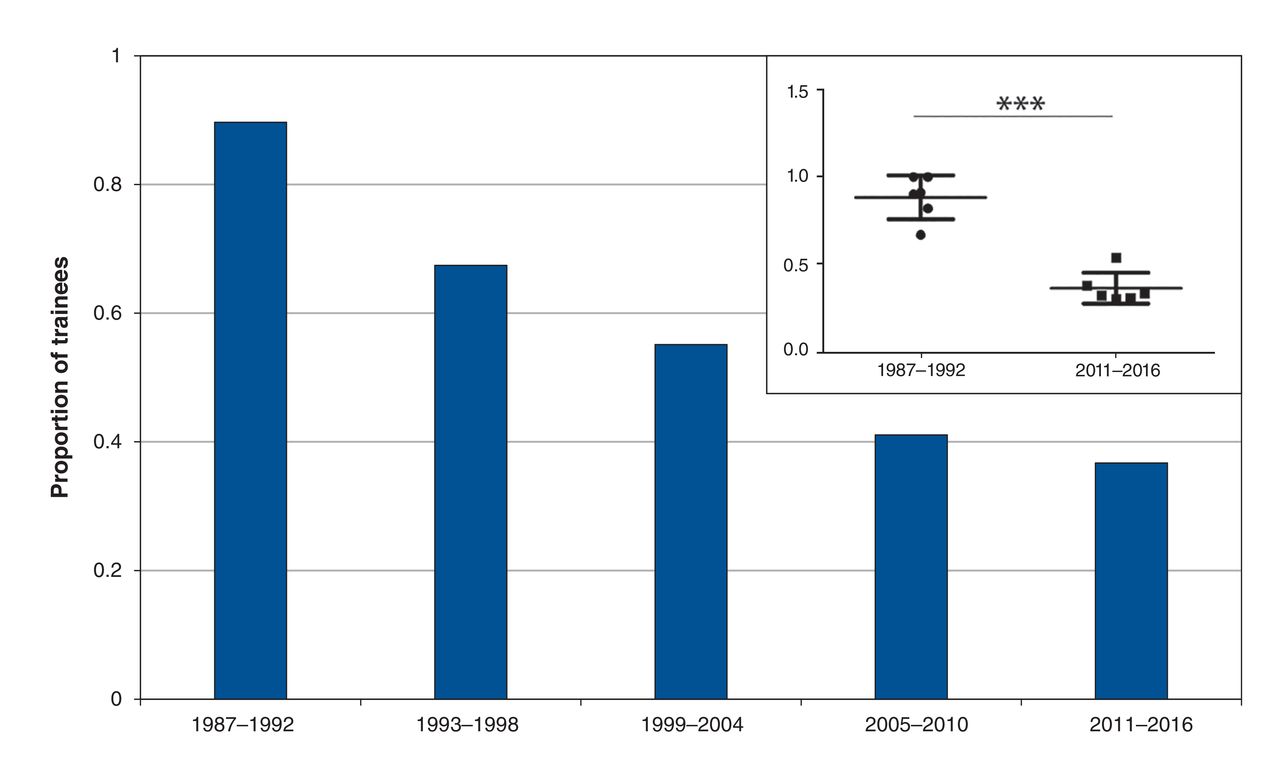
We observed a significant and persistent decline in both the relative and absolute numbers of clinicians obtaining training in fundamental research (Figures 1 and 2), with a corresponding increase in the proportion pursuing clinical research (including clinical epidemiology and education). In particular, the proportion of trainees engaged in basic science research fell by 60% from the period 1987-1992 to 2011-2016 (p = 0.005; see Figure 1 and inset). Even after excluding the 1987-1992 data from the Surgeon-Scientist Program, the proportion of Clinician-Investigator trainees engaged in basic science research fell by 55% from 1993-1998 to 2011-2016 (p = 0.005; data not shown). A χ2 test for trend for all quintiles also showed a significant decline over time (p < 0.0001; data not shown). Although the total number of trainees in the Clinician-Investigator Program increased over time (Figure 2), the absolute number of residents in basic science training has declined since 1999-2004.

Research projects from trainees in the Surgical Scientist Program (1987-1992) and Clinician Investigator Program (1993-2016) - both at the University of Toronto - were categorized by 2 independent raters as pertaining to basic science, epidemiology, or education. The proportion pertaining to basic science is depicted here. The absolute numbers of trainees are shown in Figure 2. Inset shows proportions for each year in the first and last quintiles with mean and standard deviation; p = 0.005 by 2-tailed t test.
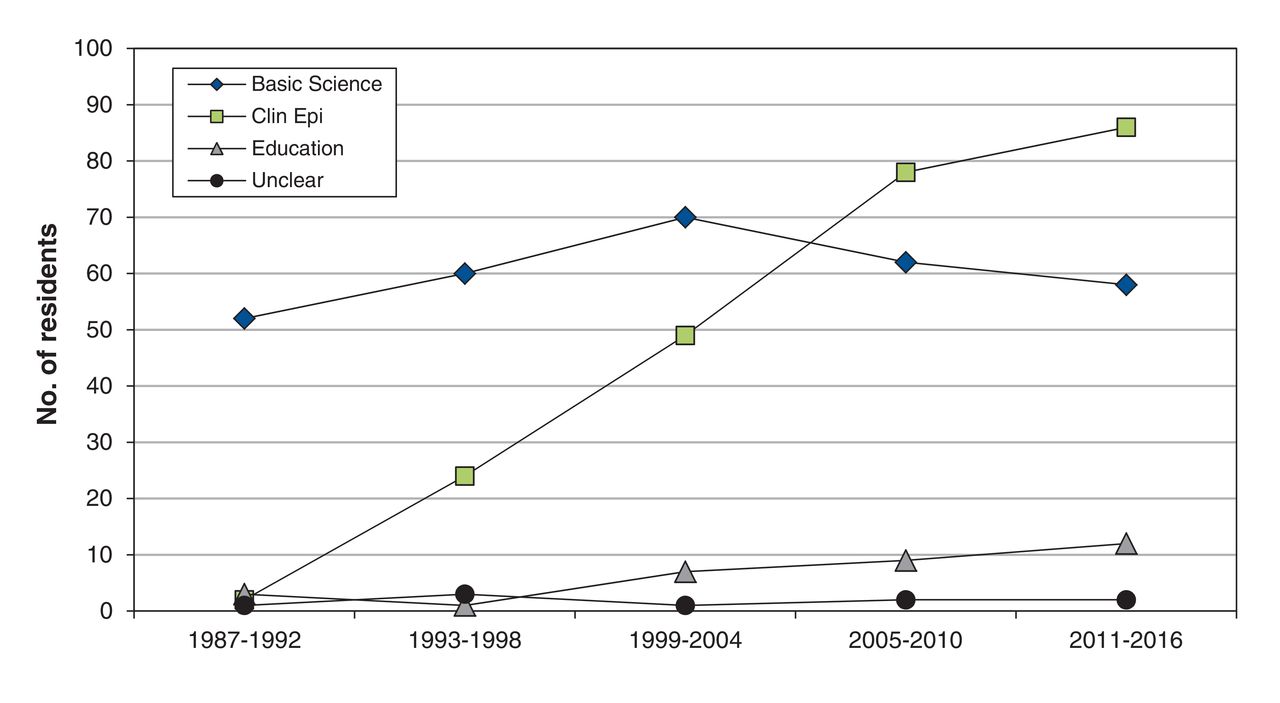
Research projects from trainees in the Surgical Scientist Program (1987-1992) and Clinician Investigator Program (1993-2016) - both at the University of Toronto - were categorized by 2 independent raters as pertaining to basic science, epidemiology or education; 9 projects could not be categorized ("unclear"). Data are divided into quintiles of time.
Interpretation
Our data show a significant decline in both the relative and absolute numbers of clinicians obtaining training in basic science research over the last 30 years. Most (90%) of the research projects completed by trainees in the Surgeon-Scientist Program at the University of Toronto from 1987-1992 were classified as basic science. More recently, only 37% were classified as basic research.
It may be argued that although the decline in the proportion of residents studying basic science is steep, the absolute numbers of trainees in basic science has fallen more recently and more gradually (e.g., from 70 in 1999-2004 to 58 in 2011-2016). However, it is instructive to note that over the same time period, the population of Canada increased by almost 17%;7 furthermore, the number of residents admitted to Core Internal Medicine and the Department Surgery at the University of Toronto increased by 56% and 21%, respectively, over the same period (1999-2016, data not shown). Thus, whether in relative or absolute terms, the cohort of potential clinician-scientists pursuing fundamental research has not been keeping pace with the growth of the trainee population or the population at large.
Clinicians pursuing academic medicine now have many more options compared with a generation ago, and the dwindling popularity of basic science parallels the birth and expansion of important disciplines such as health services research, patient safety and quality improvement. Furthermore, changes in medical school curricula away from the basic sciences or decreased emphasis on the topic in residency training programs may have contributed.
Limitations
Because our sample came from only 1 university, some may question the generalizability of our data. That said, our sample size is very large and is drawn from the largest such program in the country. Because our data focus on residents, we have a lack of information on the subsequent careers of the trainees in the cohort, or on the activity of Canadian clinician-scientists in general. Given the rigorous training required for an academic career in medicine, most clinician-scientists are likely to pursue graduate degrees; thus, the numbers of resident trainees pursuing basic research are likely be a good first-approximation of the numbers of clinician-scientists. This would have to be confirmed by further study on the career paths of physicians over time. Finally, there was potential for the misclassification of research projects. For example, our analysis was based on the project title and the supervisor, and it is possible that some trainees may have had more than 1 project. In our experience, however, these projects do not usually cross disciplines (i.e., both projects would be in epidemiology or in basic science, rather than a trainee pursuing 1 of each).
Conclusion
Our data show a significant decline in both the relative and absolute numbers of clinicians obtaining training in fundamental research over the last 30 years. If this trend continues, the participation of physicians in basic science investigation will be in jeopardy.
Historically, physician-scientists have played a key role in bringing clinical questions to the laboratory and returning with scientific advances.8 Because scientific discovery forms the underpinning of modern medicine, in our opinion, engagement by clinicians in basic science research is both desirable and essential.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/4/3/E444/suppl/DC1
Acknowledgements
The authors thank Astrid Augspols and Joanna King for assistance with data collection.
Footnotes
Competing interests: None declared.
Contributors: Neil Goldenberg, Benjamin Steinberg, Val Cabral, James Rutka, Robert Chen, Norman Rosenblum, Andras Kapus, Warren Lee made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work. Warren Lee, Neil Goldenberg, Benjamin Steinberg, Andras Kapus, Norman Rosenblum, James Rutka, Robert Chen drafted the work or revised it critically for important intellectual content. All authors approved the final version to be published.
References
- Copyright 2016, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.