


Abstract
Background: In October 2012, the Canadian Supreme Court ruled that people living with HIV must disclose their HIV status before sex that poses a "realistic possibility" of HIV transmission, clarifying that in circumstances where condom-protected penile-vaginal intercourse occurred with a low viral load (< 1500 copies/mL), the realistic possibility of transmission would be negated. We estimated the proportion of people living with HIV who use injection drugs who would face a legal obligation to disclose under these circumstances.
Methods: : We used cross-sectional survey data from a cohort of people living with HIV who inject drugs. Participants interviewed since October 2012 who self-reported recent penile-vaginal intercourse were included. Participants self-reporting 100% condom use with a viral load consistently < 1500 copies/mL were assumed to have no legal obligation to disclose. Logistic regression identified factors associated with facing a legal obligation to disclose.
Results: We included 176 participants, 44% of whom were women: 94% had a low viral load, and 60% self-reported 100% condom use. If condom use and low viral load were required to negate the realistic possibility of transmission, 44% would face a legal obligation to disclose. Factors associated with facing a legal obligation to disclose were female sex (adjusted odds ratio [OR] 2.19, 95% confidence interval [CI] 1.13-4.24), having 1 recent sexual partner (v. > 1) (adjusted OR 2.68, 95% CI 1.24-5.78) and self-reporting a stable relationship (adjusted OR 2.00, 95% CI 1.03-3.91).
Interpretation: Almost half the participants in our analytic sample would face a legal obligation to disclose to sexual partners under these circumstances (with an increased burden among women), adding further risk of criminalization within this marginalized and vulnerable community.
Since the late 1980s, existing criminal or HIV-specific laws have been used in many settings worldwide to prosecute people living with HIV who were alleged to have put others at risk of acquiring HIV.1 Most of these criminal prosecutions against people living with HIV have occurred in North America.1 Canada has the second highest absolute number of convictions of people living with HIV globally.1,2 At the time of writing, an estimated 181 Canadians had been charged for allegedly failing to disclose their HIV status to sexual partners (Prof. Eric Mykhalovskiy, York University, Toronto, and Dr. Sophie Patterson, Simon Fraser University, Burnaby: personal communication, 2015).
Most people accused of HIV nondisclosure in Canada have faced charges of aggravated sexual assault, based on the legal interpretation that nondisclosure of HIV status represents fraud, vitiating consent to an otherwise consensual sexual encounter. This charge carries a maximum sentence of life imprisonment and mandatory life-long registration as a sexual offender, even in the absence of HIV transmission.
A new precedent for the use of the criminal law against people living with HIV in Canada was set on Oct. 5, 2012, when the Supreme Court of Canada released its ruling on 2 major cases.3,4 Proactive serostatus disclosure by an HIV-positive individual must now precede any sexual activity that poses a "realistic possibility" of HIV transmission. The court clarified that in circumstances where a person living with HIV engaged in condom-protected penile-vaginal intercourse with a low plasma HIV RNA viral load (defined by the court as < 1500 copies/mL), there would be no realistic possibility of HIV transmission, thus no legal duty to disclose.3 Whether this legal test would hold true for sexual encounters other than penile-vaginal intercourse was not clarified by the court.
Establishing the absence of a realistic possibility of HIV transmission may be possible for circumstances other than condom-protected penile-vaginal sex with a low viral load, depending on the evidence presented during criminal trials. Indeed, the Supreme Court of Canada indicated that differing circumstances and treatment advances could lead to future adaptations of this legal position.3 Lower courts may find greater flexibility in their interpretation of the realistic possibility of HIV transmission. After the 2012 Supreme Court ruling, a teenage boy was acquitted of aggravated sexual assault in the Nova Scotia Youth Justice Court after allegedly failing to disclose his HIV status before an episode of penile-vaginal intercourse.5 Based on evidence presented during the trial, the presiding judge deemed that there was no realistic possibility of HIV transmission in the context of an undetectable viral load, regardless of whether or not a condom was used. However, in the absence of consistency in the application of the Supreme Court's legal test by the lower courts, it is prudent to assume the strictest interpretation of this ruling.
There is no consensus regarding the effectiveness of legally enforced disclosure as an HIV prevention tool.6 Concerns remain that the criminalization of HIV nondisclosure fails to acknowledge the substantial challenges of HIV disclosure, including secondary disclosure; isolation; rejection by partners, friends and family; violence; stigma and discrimination.7-9 The literature suggests that people living with HIV who inject drugs face unique barriers to safe disclosure in the criminalized environment in which they live, navigate sexual relationships and seek care;7,10,11 including loss of income, drugs or housing and threats to personal safety in the form of emotional, physical and sexual violence.7,10,12
Using cross-sectional data from a community-recruited cohort of people living with HIV who inject drugs, we estimated the proportion of participants who would face a legal obligation to disclose their HIV status before penile-vaginal intercourse if both condom use and a low viral load were required to remove the realistic possibility of HIV transmission, and avoid criminal liability for HIV nondisclosure.3,4
Methods
Data sources
The AIDS Care Cohort to evaluate Exposure to Survival Services (ACCESS) is an ongoing observational prospective cohort study of people living with HIV who use illicit drugs in Vancouver. The study has been described previously.13 Briefly, participants were eligible for study inclusion if they were HIV-positive, aged 18 years or older and had used illicit drugs other than cannabis in the 30 days before their baseline interview. Recruitment of ACCESS participants began in 2005 and is ongoing. Snowball sampling methods are used, building on self-referral, word of mouth and extensive street outreach, with recruitment materials displayed in clinics and storefront agencies. Recruitment efforts are focused in the Downtown Eastside area of Vancouver; the site of an explosive outbreak of HIV infection among people living with HIV who inject drugs and their sexual partners beginning in the mid-1990s.14 This area has high levels of illicit drug use, homelessness and poverty, and an active open drug market.
At recruitment, participants complete a baseline interviewer-administered questionnaire, which elicits information on lifetime and recent characteristics, behaviours and exposures, and a nurse-led questionnaire and interview, which includes blood tests for HIV clinical monitoring. At 6-month intervals, participants are invited to complete follow-up interviews and nursing examinations. Within the cohort, loss to follow-up (defined as missing all interviews in the preceding 12 mos) is 6 (interquartile range 5-7) per 100 person-years.
HIV treatment records and clinical profiles held by the British Columbia Centre for Excellence in HIV/AIDS Drug Treatment Program are accessed for all ACCESS participants through a secure, confidential linkage. The British Columbia Centre for Excellence in HIV/AIDS provides medications and clinical monitoring tests free of charge to all people living with HIV in British Columbia through the government's universal health care plan.15
The ACCESS study's semiannual follow-up and confidential linkage to comprehensive HIV clinical data through the Drug Treatment Program permits longitudinal evaluation of the interrelations of behavioural, environmental and social-structural exposures on access and adherence to antiretroviral therapy and HIV disease progression among more than 950 people living with HIV who use illicit drugs (cohort size at the time of writing). ACCESS has been approved by the University of British Columbia/Providence Health Care Research Ethics Board. All participants provide written informed consent to participate in the study and are compensated $30 for each visit. The survey does not collect data on serostatus disclosure practices, thus this analysis does not present behaviours that could be interpreted as legal offences under Canadian nondisclosure case law.
Eligibility criteria
This cross-sectional analysis included ACCESS participants who had completed an interview since Oct. 5, 2012, to capture sexual risk behaviours and viral profile since the Supreme Court ruling. We restricted inclusion to participants with a history of injection drug use who had at least 1 viral load and CD4 measurement within 180 days of their baseline visit, and for whom data on condom use were available. If a participant completed more than 1 interview during the study period, data were drawn from the later interview. We restricted inclusion to participants who were sexually active, defined as self-reporting penile-vaginal intercourse with commercial or noncommercial sex partners in the 6-month period before the interview. Penile-vaginal intercourse was the focus of this analysis because this was the type of sexual activity on which the 2012 Supreme Court's ruling was based. The Supreme Court of Canada has yet to rule on HIV nondisclosure in the context of anal or oral sex. The date of administrative censoring was Nov. 30, 2013.
Measures
Primary outcome
We sought to identify participants who would face a legal obligation to disclose their HIV status to sexual partners if condom-protected penile-vaginal intercourse in the context of a low viral load (< 1500 copies/mL) was required to negate the realistic possibility of HIV transmission, and thus avoid criminal liability for HIV nondisclosure. Participants who self-reported 100% condom use during all episodes of penile-vaginal intercourse, and who also achieved viral load measurements consistently lower than 1500 copies/mL within 6 months before the study interview were assumed to face no legal obligation to disclose their HIV status to sexual partners. We assumed that participants would face a legal obligation to disclose if they self-reported less than 100% condom use (regardless of viral load), or if they failed to achieve a viral load consistently lower than 1500 copies/mL (regardless of condom use).
Explanatory variables
Explanatory variables were selected based on perceived importance following a comprehensive literature review and availability within the data set. We considered the following explanatory variables: age (per year increase); sex (female v. male); ethnicity (white v. nonwhite); recent injection drug use (yes v. no); recent illicit drug use (excluding cannabis; yes v. no); homelessness, defined as living on the streets or with no fixed address (yes v. no); employment in a regular or temporary job, or self-employed (yes v. no); sex work, defined as exchange of sex for money, drugs, clothing or other property (yes v. no); incarceration, defined as being in detention, prison or jail (yes v. no); stable relationship, defined as being legally married or common-law, or having a regular partner (yes v. no); and number of recent commercial and noncommercial sex partners (1 v. > 1). All nonfixed variables referred to behaviours or exposures in the 6-month period before the interview, except for relationship status, which referred to current status. We defined HIV treatment status by assessing the number of days participants had been dispensed antiretroviral therapy in the 6 months before the interview (≥ 1 v. 0 days). While a history of injection drug use was specified as an inclusion criterion for this analysis, we included recent injection drug use as a covariate to signify ongoing drug use.
Statistical analysis
We calculated the proportion of participants who would face a legal obligation to disclose HIV serostatus to sexual partners under the aforementioned circumstances. Sociodemographic, behavioural and clinical characteristics were compared between participants who would face a legal obligation to disclose versus those who would not using the Pearson χ2 test for categorical variables (and the Fisher exact test for small cell counts), and the Wilcoxon rank-sum test for continuous variables. Logistic regression identified independent covariates of facing a legal obligation to disclose. Candidates for model inclusion were variables having p < 0.2 in the bivariable analysis, or variables considered a priori to influence likelihood of facing a legal obligation to disclose following literature review.
Imputation methods were used to recode data for 10 participants for whom data related to number of recent sexual partners were missing. Specifically, the median number of sexual partners within the cohort was assigned to participants for whom data were not available. This method was used to preserve statistical power and avoid biases associated with excluding these participants from the model.
Model construction was based on the backward selection approach and Akaike Information Criterion. The most parsimonious model was selected as the model with the lowest Akaike Information Criterion value. We computed the Variance Inflation Factor to quantify the degree of collinearity present in the regression analysis on the basis that a strong correlation between variables would increase the variance of the coefficients, rendering them unstable and complicating interpretation of the model output. The Variance Inflation Factor was < 1.2 for all variables in the final model, suggesting that no collinearity was present. P values were 2-sided and considered statistically significant at less than 0.05. All statistical analyses were conducted using the SAS software version 9.3 (SAS Institute Inc., Cary, NC).
Results
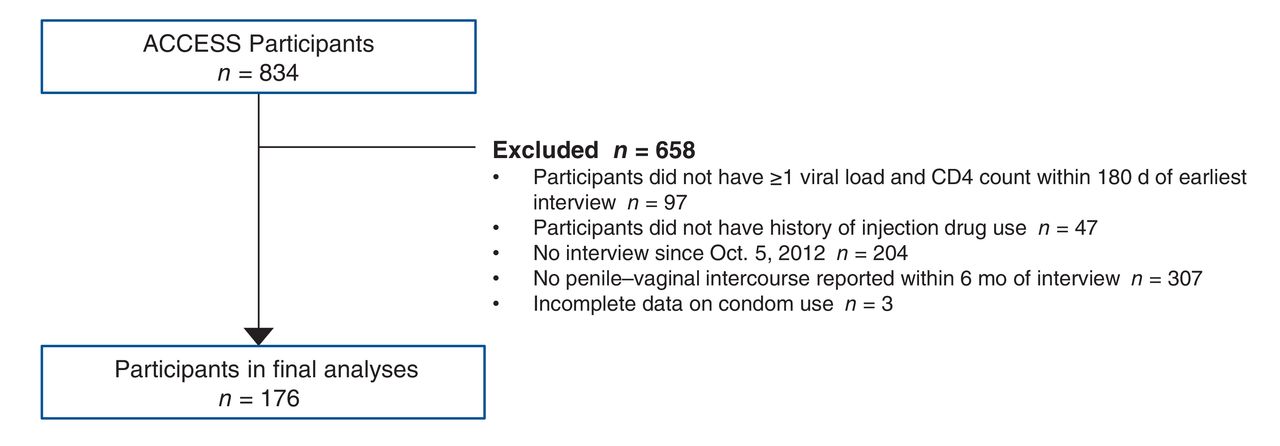
After applying the inclusion criteria, 176 (56% male) of the 834 ACCESS participants recruited between 2005 and 2013 were included in our analyses. We excluded 97 participants who did not have at least 1 viral load and CD4 count test recorded within 180 days of their earliest interview, 47 participants without a history of injection drug use, 204 participants who had not completed an interview since Oct. 5, 2012, 307 participants who reported no episodes of penile-vaginal intercourse within 6 months of the interview and 3 participants for whom data on condom use were not available (Figure 1).

Exclusion criteria applied to reach final analytic sample.
The characteristics of the analytic sample are presented in Table 1. Of the 176 participants included in this analysis, 10 (6%) failed to achieve a viral load consistently lower than 1500 copies/mL, and 70 (40%) self-reported less than 100% condom use during penile-vaginal intercourse within the 6-month period before the study interview. Among the 166 participants who consistently achieved a viral load of less than 1500 copies/mL, 67 reported less than 100% condom use. If both condom use and a viral load of less than 1500 copies/mL were required to negate the realistic possibility of HIV transmission and avoid criminal liability for HIV nondisclosure, 77 (44%) participants would face a legal obligation to proactively disclose their HIV status to sexual partners (Table 2). However, if either consistent condom use or a viral load of less than 1500 copies/mL was sufficient to negate the realistic possibility of HIV transmission, only 3 (2%) participants would face a legal obligation to disclose (0% of men, 4% of women).
When stratifying the results by sex, 35% of men v. 55% of women would face a legal obligation to proactively disclose their HIV serostatus to sexual partners if both condom use and a viral load of less than 1500 copies/mL were required to negate the realistic possibility of HIV transmission (p = 0.011). Compared with men, significantly fewer women achieved a viral load of less than 1500 copies/mL (90% v. 98%, p = 0.02) and significantly fewer women self-reported 100% condom use (52% v. 67%, p = 0.048) in the 6-month period before the study interview.
In the multivariable logistic regression model, factors independently associated with facing a legal obligation to disclose were female sex (adjusted odds ratio [OR] 2.19, 95% confidence interval [CI] 1.13-4.24); having only 1 recent sexual partner (v. > 1 partners) (adjusted OR 2.68, 95% CI 1.24-5.78) and self-reporting a stable relationship (adjusted OR 2.00, 95% CI 1.03-3.91) (Table 3).
Interpretation
Among sexually active participants in a community-recruited cohort of people living with HIV who inject drugs, we found that almost half the participants would face a legal obligation to proactively disclose HIV serostatus to sexual partners if both condom use and a low viral load were required to negate the realistic possibility of HIV transmission. In a multivariable model, facing a legal obligation to disclose under these circumstances was positively associated with female sex, self-reporting a stable relationship and having only 1 recent sexual partner.
Facing a legal obligation to disclose was driven primarily by inconsistent condom use rather than by viral load in this analysis. It should be noted that ACCESS is an older, treatment-experienced cohort in a province with an ongoing treatment-as-prevention initiative16,17 and universal access to health care free of charge, including all HIV treatment, care and medications. In other jurisdictions where such initiatives are not widespread, additional challenges to the uptake and adherence to antiretroviral therapy may be encountered, which may compromise the ability to satisfy this legal test for HIV nondisclosure. Indeed, studies in other North American settings have found that members of marginalized and vulnerable groups, including people who inject drugs,18-21 ethnic minorities,22 sex workers23 and homeless individuals,24 experience barriers to accessing antiretroviral therapy and achieving sustained viral suppression.
We found that women were significantly more likely to face a legal obligation to disclose if both condom use and a low viral load were required to negate the realistic possibility of HIV transmission, driven by both viral load and condom use. Previous Canadian studies have shown that women experience poorer HIV-related clinical outcomes compared with men, mediated by suboptimal engagement and retention within HIV services and lower adherence to antiretroviral therapy.18-21,25,26 Inconsistent condom use among women living with HIV is well-described in the literature, attributed to fertility desire and serocondordant partnerships, in addition to challenges negotiating condom use, including gendered power imbalances, fear of inadvertent status disclosure and the threat of violence.27-30 Marginalized women living with HIV may experience additional social-structural barriers to insisting upon safer sex practices, particularly those who are economically disadvantaged and who engage in survival sex work,8,31,32 compromising their ability to avoid criminal liability for HIV nondisclosure through both achievement of a low viral load and condom use.
The observed gender difference in facing a legal obligation to disclose is a particular concern, as previous work has shown that women experience unique barriers to HIV disclosure;7 particularly those who face power inequality within dependent partnerships and risk violence or abandonment associated with disclosure.12,33-35 A recent cross-sectional study among harder-to-reach people living with HIV in Vancouver found that women were significantly less likely to disclose to new sexual partners compared with heterosexual male counterparts.36Although women are underrepresented among defendants in Canadian nondisclosure prosecutions to date, marginalized women feature prominently among women who have faced criminal charges,37 including women living with addiction, survivors of violence, sex workers and indigenous women.38,39
Participants in a stable relationship were more likely to face a legal obligation to proactively disclose to sexual partners based on the legal test applied in this analysis. Unsurprisingly, this finding is driven by inconsistent condom use. This observation is supported by a previous analysis within ACCESS, which reported an independent association between condomless sex and partnered relationship status,31 and literature from other international settings.40-42 Previous work has shown that people living with HIV are more likely to disclose to regular versus casual sexual partners,43-45 thus it stands to reason that many ACCESS participants who are in a stable relationship will have disclosed to their partners and made a mutual decision to engage in condomless sex. Participants with only one recent sexual partner were also more likely to face a legal obligation to proactively disclose, which was similarly driven by inconsistent condom use. We expect that participants with more than 1 sexual partner are less likely to proactively disclose, and more likely to insist on condom use. Previous work supports that people living with HIV with 1 versus multiple sexual partners are more likely to self-report disclosing to partners.46
Notably, if either condom use or a low viral load during penile-vaginal sex were sufficient to negate the realistic possibility of HIV transmission and avoid criminal liability for non-disclosure, 98% participants in our cohort would face no legal obligation to disclose to sexual partners. Public health and human rights advocates have argued that, at a minimum, either condom use or a suppressed viral load during vaginal or anal sex should be sufficient to remove the legal obligation to disclose (emphasizing that additional factors might also be relevant in determining HIV transmission risk on a case-by-case basis).47 Furthermore, they maintain that the legal obligation to disclose should be removed in cases where there is very low risk of transmission, such as in cases of oral sex.47,48 The requirement of both condom use and a low viral load to negate the realistic possibility of sexual HIV transmission stands in conflict with evidence-based science that shows the dramatic reduction in HIV transmission risk associated with either viral suppression with antiretroviral therapy49-53 or condom use.54 A recent consensus statement by Canadian HIV experts forcefully argues that empirical evidence does not justify the current use of the criminal law against people living with HIV in Canada.55 This statement has since been endorsed by more than 75 scientists and clinicians across Canada.56
It must be acknowledged that many ACCESS participants will disclose their HIV status to sexual partners, thus will not be at risk of criminal charges regardless of condom use or viral profile. Disclosure practices are not measured within the ACCESS survey; however, a cross-sectional survey of treatment-experienced people living with HIV in Vancouver found that most (73%) of the participants self-reported disclosing their HIV serostatus to all new sexual partners.36
Readers should be aware of some limitations to our study. Our analytic sample represents a very small subset of the ACCESS cohort (those with available data, a history of injection drug use and recent history of penile-vaginal intercourse). Because data on HIV serostatus of sexual partners are not routinely collected within the ACCESS survey, we could not identify seroconcordant partnerships where legal concerns around HIV exposure and transmission may be reduced, rates of disclosure may be higher,45 and condom use may be lower.57 Condom use was self-reported, therefore subject to recall and social desirability reporting biases, resulting in potential underestimation of the proportion of participants who would face a legal obligation to disclose.
Findings from this study may not be generalizable to non-Canadian settings owing to the specificity of Canadian HIV nondisclosure case law. On account of the ambitious provincial scale-up of treatment-as-prevention in British Columbia,16,17 our findings may underestimate the number of people living with HIV who inject drugs who would face a legal obligation to disclose in other provinces, where they may experience additional barriers to treatment engagement.
Conclusion
We observed that if both condom use and a low viral load are required to remove the realistic possibility of HIV transmission and avoid criminal liability for HIV nondisclosure, almost half of the participants may risk criminal prosecution should they not disclose their HIV serostatus to sexual partners. Current case law may disproportionately impact the most marginalized and vulnerable women living with HIV in Canada. Our study reveals another dimension to how the criminal justice system can shape the health and lives of people living with HIV who inject drugs, reinforcing the critical need for public health initiatives to address barriers to HIV treatment and support safe HIV status disclosure within marginalized communities.
Future work should evaluate the awareness and impact of HIV nondisclosure case law among women living with HIV in Canada who are disproportionately affected by HIV or underserved by health services, and who encounter considerable barriers to safe disclosure.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/4/2/E169/suppl/DC1
Acknowledgements
The authors thank the study participants for their contribution to the research, as well as current and past researchers and staff.
Footnotes
Competing interests: Julio Montaner reports grants from the British Columbia Ministry of Health, the National Institute on Drug Abuse, the National Institutes of Health, Abbvie, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck and ViiV Healthcare. M.-J. Milloy reports grants from the National Institute on Drug Abuse and from National Green Biomed.
Contributors: Sophie Patterson, Angela Kaida, Robert Hogg, Gina Ogilvie, and M.-J. Milloy conceived the idea for this analysis. Robert Hogg, Julio Montaner, M.-J. Milloy, Thomas Kerr and Evan Wood contributed to design and acquisition of data. Data preparation and statistical analysis were conducted by Sabina Dobrer and Paul Nguyen. Data interpretation was performed by Sophie Patterson, M.-J. Milloy, Paul Nguyen, Sabina Dobrer and Angela Kaida. Sophie Patterson drafted the initial manuscript, and all of the authors contributed to the final version. All of the authors have critically reviewed and approved the final manuscript, gave approval for publication and agree to act as guarantors of the work.
Funding: The ACCESS study is supported by the United States National Institutes of Health (R01-DA021525). This research was undertaken, in part, thanks to funding from the Canada Research Chairs program through a Tier 1 Canada Research Chair in Inner City Medicine, which supports Dr. Evan Wood. Dr. Milloy is supported in part by the US National Institutes of Health (R01DA021525). Dr. Patterson is supported by a Study Abroad Studentship from the Leverhulme Trust. Dr. Hogg has held grant funding from the National Institutes of Health, Canadian Institutes of Health Research National Health Research Development Program, and Health Canada. He has also received funding from GlaxoSmithKline and Merck Frosst Laboratories for participating in continued medical education programs. Julio Montaner is supported by the British Columbia Ministry of Health and through an Avant-Garde Award (DP1-DA026182) from the National Institute of Drug Abuse (NIDA), at the US National Institutes of Health (NIH). He has also received financial support from the International AIDS Society, United Nations AIDS Program, World Health Organization, National Institutes of Health Research-Office of AIDS Research, National Institute of Allergy & Infectious Diseases, The United States President's Emergency Plan for AIDS Relief (PEPfAR), UNICEF, the University of British Columbia, Simon Fraser University, Providence Health Care and Vancouver Coastal Health Authority. This research was also supported through funding from the Canada Research Chairs program through a Tier 2 Canada Research Chair in Global Perspectives in HIV and Sexual and Reproductive Health, which supports Dr. Angela Kaida.
References
- Copyright 2016, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.