


Abstract
Background: Since the onset of the COVID-19 pandemic, there has been concern about the impact of SARS-CoV-2 infection among individuals with mental illnesses. We analyzed the SARS-CoV-2 vaccination status of Ontarians with and without a history of mental illness.
Methods: We conducted a population-based cross-sectional study of all community-dwelling Ontario residents aged 19 years and older as of Sept. 17, 2021. We used health administrative data to categorize Ontario residents with a mental disorder (anxiety, mood, substance use, psychotic or other disorder) within the previous 5 years. Vaccine receipt as of Sept. 17, 2021, was compared between individuals with and without a history of mental illness.
Results: Our sample included 11 900 868 adult Ontario residents. The proportion of individuals not fully vaccinated (2 doses) was higher among those with substance use disorders (37.7%) or psychotic disorders (32.6%) than among those with no mental disorders (22.9%), whereas there were similar proportions among those with anxiety disorders (23.5%), mood disorders (21.5%) and other disorders (22.1%). After adjustment for age, sex, neighbourhood income and homelessness, individuals with psychotic disorders (adjusted prevalence ratio 1.19, 95% confidence interval [CI] 1.18–1.20) and substance use disorders (adjusted prevalence ratio 1.35, 95% CI 1.34–1.35) were more likely to be partially vaccinated or unvaccinated relative to individuals with no mental disorders.
Interpretation: Our study found that psychotic disorders and substance use disorders were associated with an increased prevalence of being less than fully vaccinated. Efforts to ensure such individuals have access to vaccinations, while challenging, are critical to ensuring the ongoing risks of death and other adverse consequences of SARS-CoV-2 infection are mitigated in this high-risk population.
Since the onset of the COVID-19 pandemic, there has been concern about the impact of SARS-CoV-2 infection on individuals with mental illnesses, particularly severe ones.1 Recent studies have corroborated this concern, with SARS-CoV-2-related mortality rates nearly fourfold higher among individuals with a diagnosis of schizophrenia compared with the general population.2,3 In a study using electronic health records, individuals with substance use disorders were at increased risk of being infected with SARS-CoV-2, developing severe complications and dying.4
Although the rates of vaccination among those with a history of mental illness are unknown, there is reason to believe that such individuals would be less likely to be vaccinated. Early in the pandemic, there was evidence that vaccination rates were lower for individuals with low socioeconomic status, 5 and those experiencing homelessness expressed greater reluctance to be vaccinated.6 Low socioeconomic status7 and homelessness8 are more common among individuals with mental illnesses than the general population, which may reduce these individuals’ access to care and further reduce the likelihood of getting vaccinated.9
Achieving high vaccination coverage among individuals with mental illnesses is therefore especially important to protect individuals from the adverse effects of SARS-CoV-2 infection. We analyzed the SARS-CoV-2 vaccination status of Ontario residents with and without a history of mental illness.
Methods
We conducted a population-based cross-sectional study of all Ontario residents aged 19 years and older with Ontario Health Insurance Plan (OHIP) coverage as of Sept. 17, 2021. OHIP provides health care coverage to all Ontario residents, with the exception of certain populations (military and certain Indigenous populations who receive health care from the federal government). We restricted our sample to people aged 19 years and older because vaccination rules for children were different. We also excluded individuals residing in long-term care settings because vaccination schedules differed for this population. All adults aged 18 years and older were eligible for their first dose of vaccine as of May 18, 2021, and their second dose as of June 28, 2021.10 We set the vaccination prevalence date to Sept. 17, 2021, because after this date, certain Ontarians were eligible for a third SARS-CoV-2 vaccine.
Data sources
All our data sources were linked at the individual level using unique encoded identifiers and analyzed at ICES. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. We used the Ontario COVID-19 Vaccine Database (COVaxON) for our vaccination outcomes and the Registered Persons Database (RPDB) for demographic data. Our exposure of prior mental health disorder categories was captured using the following databases: the OHIP database for physician visits, the National Ambulatory Care Reporting System (NACRS) for emergency department visits, the Canadian Institute for Health Information Discharge Abstract Database (CIHIDAD) for hospital admissions to nonpsychiatric beds and the Ontario Mental Health Reporting System (OMHRS) for hospital admissions to psychiatric beds. We also used the Same Day Surgery (SDS) database.
Outcome
We measured vaccination status up to Sept. 17, 2021, and defined individuals as fully vaccinated if they had received 2 vaccine doses, and partially or not vaccinated if they had received 1 or no vaccine doses. The COVaxON data used to ascertain vaccination status have near complete capture of vaccinations. The average of the monthly linkage rate during the study period for dose 1 vaccinations was 93.6%, with the vast majority of linkages being deterministic given that health card numbers were provided (see Appendix 1, available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1, for more information on all study variables).
Exposure
Based on mental health and addiction (MHA) utilization, defined as having at least 1 service utilization visit with any of the diagnostic codes listed in Appendix 2 (available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1) in the 5 years before index, each subject was assigned to a level of MHA severity and to an MHA diagnosis recorded in the MHA utilization record of greatest severity and recency. Those individuals with no prior MHA service utilization would not be assigned to a diagnostic category because no diagnosis would have been generated. We assigned individuals to MHA level of severity in order of MHA hospitalization (highest severity), MHA emergency department visit, MHA outpatient visit and no prior MHA service utilization (lowest severity). We obtained the primary diagnosis from the record of the greatest severity, which was used to classify individuals into the following mutually exclusive diagnostic categories: anxiety, mood, substance use, psychotic or other disorders. The diagnostic codes used to assign individuals to these diagnostic categories have been used in previous publications.11 This classification scheme prioritizes diagnoses from sources known to have higher levels of validity (i.e., hospital records) over those with lower levels of validity (i.e., outpatient visits). If individuals had 2 or more records at a given level of severity (e.g., 2 MHA hospitalizations), we used the diagnosis from the most recent record. For example, if an individual had an MHA outpatient visit (diagnosis: substance use disorder) in August 2019, an MHA hospitalization (diagnosis: psychotic disorder) in July 2019 and an MHA hospitalization (diagnosis: mood disorder) in November 2018, we assigned the individual to the psychotic disorder group. This algorithm resulted in 2 measures of severity, a resource utilization–based measure (i.e., MHA hospitalization, MHA emergency department visit, MHA outpatient visit or none12,13) and a diagnosis-based measure, which are both known to be related to the level of psychiatric severity (i.e., MHA hospitalizations and psychosis and substance disorders being the most severe). Outpatient visits related to MHA are defined using a validated algorithm.14 The severity gradient has been used in multiple prior studies to use health service utilization as a proxy for psychiatric illness severity.12,13,15
Covariates
We measured age, sex, rural or urban residence, homelessness and neighbourhood income quintile. Homelessness, common among those with severe mental illness and a barrier to vaccination, was captured using flags or indicators in DAD, SDS, OMHRS, NACRS and RPDB (Appendix 3, available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1).16 Neighbourhood-income quintiles are based on average household income adjusted for household and community size. Comorbidities were measured using the Johns Hopkins collapsed Aggregated Diagnosis Groups.17 More information on study variables can be found in Appendix 1.
Statistical analysis
We first conducted descriptive analyses assessing vaccination prevalence across the diagnostic categories. We ran modified Poisson regression models, which use robust standard errors to correct for the binomial rather than Poisson response.18 We initially adjusted only for sex and age, and then adjusted for sex, age, rurality, homelessness and income quintile, and then conducted a fully adjusted model also incorporating comorbidities. The modified Poisson regression model estimates ratios of the prevalence of less than full vaccination between defined groups. Income was the only variable with missing data (0.3%), and individuals with missing data were excluded during the modelling. All analyses were conducted using SAS version EG 7.1.
We conducted sensitivity analyses. First, we tested whether the associations between our exposures (diagnostic groups and mental illness severity) and vaccination prevalence held when we changed the outcome to comparing no vaccination with 1 or more vaccinations. To test the specificity of our diagnostic subgroups, we conducted 2 separate analyses. In the first, we determined whether the association between the psychotic disorder subgroup and vaccination was similar to one that identifies all individuals with a diagnosis of schizophrenia19 based on a validated algorithm. Similarly, we determined if the association between substance use disorders and vaccination was similar to the association found with alcohol-related hospital admissions defined by CIHI.20
Ethics approval
The use of data in this study is authorized under section 45 of Ontario’s Personal Health Information Protection Act and is exempt from ethics board review.
Results
After inclusion and exclusion criteria were applied, we had a final sample size of 11 900 868 (Figure 1).
Study flow chart. Note: DOLC = date of last contact.
Twenty-three percent of all Ontarians were not fully vaccinated (2 vaccine doses) by Sept. 17, 2021. The proportion of individuals not fully vaccinated was higher among those with substance use (37.7%) or psychotic disorders (32.6%) than among individuals with no mental disorders (22.9%) (Appendix 4, available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1). These results were similar to those for individuals with an alcohol-related hospitalization (36.5%) or a validated schizophrenia diagnosis (37.5%). The proportion of fully vaccinated individuals with anxiety (76.5%), mood (78.5%) and other disorders (77.9%) was similar to that in the population with no mental disorders. Vaccination prevalence by severity of prior health service utilization revealed that individuals with prior mental health–related outpatient visits had a slightly lower prevalence of partial or no vaccination (21.1% v. 23.2%), whereas individuals with a prior history of mental health–related emergency department visits (35.4%) and hospitalizations (36.4%) had a higher prevalence of partial or no vaccinations (Appendix 4). This pattern of vaccination prevalence by health service use severity was similar within each diagnostic category (Appendix 4).
In the youngest age category (age 19–29 yr), the proportion of individuals less than fully vaccinated was higher than for the overall population (Appendix 4). Being less than fully vaccinated was more common among individuals with homelessness, those with higher-acuity mental health service, and those living in lower-income neighbourhoods.
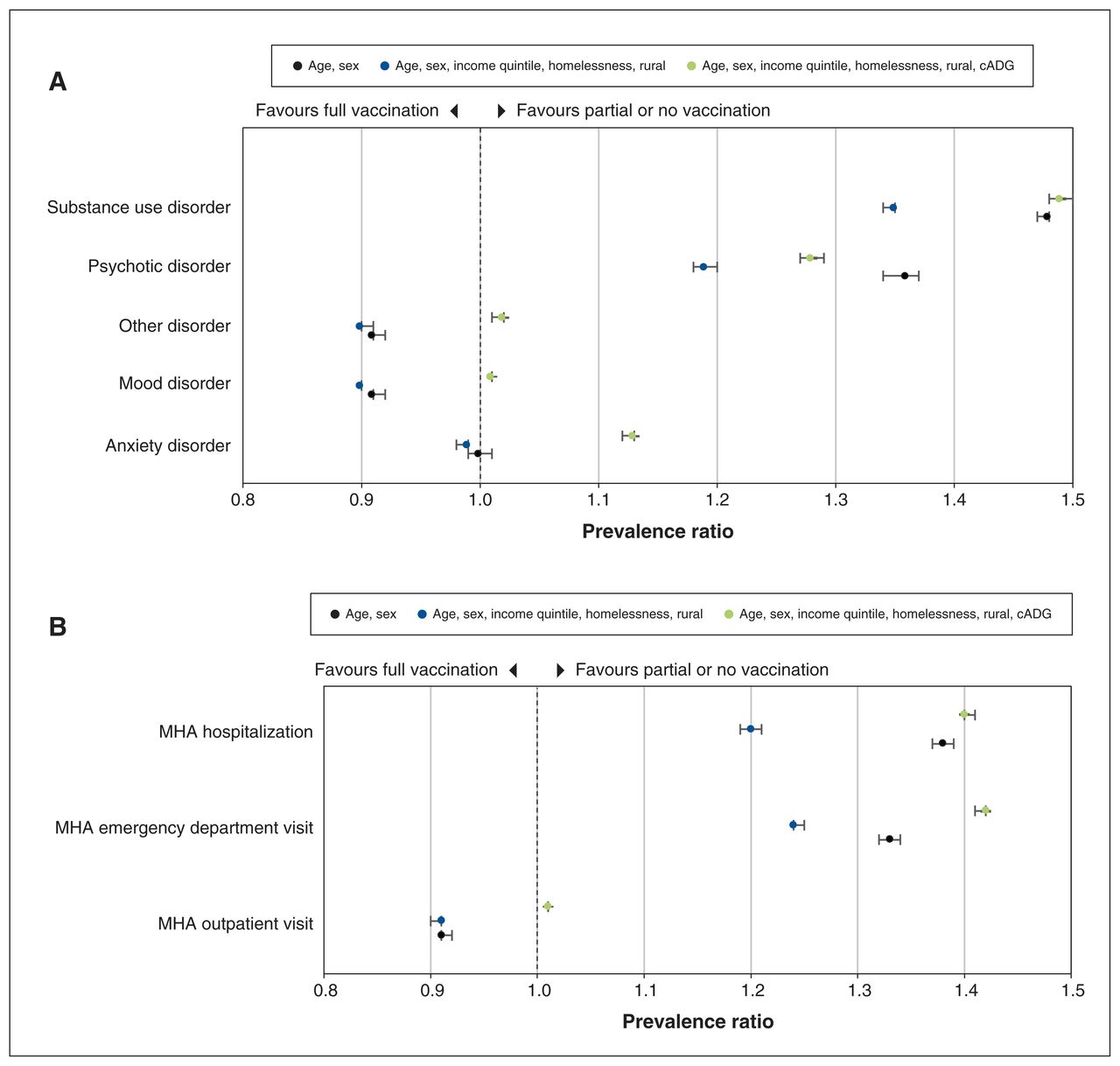
After adjustment for sex and age, individuals with mood, anxiety and other disorders were less likely to be partially vaccinated or unvaccinated than individuals with no mental disorders, whereas those with psychotic disorders (adjusted prevalence ratio 1.36, 95% confidence interval [CI] 1.34–1.37) and substance use disorders (adjusted prevalence ratio 1.48, 95% CI 1.47–1.48) were more likely to be partially vaccinated or unvaccinated (Figure 2A, Table 1). Further adjustment for neighbourhood income quintile, homelessness and rurality attenuated the association between vaccination and psychotic disorders (adjusted prevalence ratio 1.19, 95% CI 1.18–1.20) and substance use disorders (adjusted prevalence ratio 1.35, 95% CI 1.34–1.35), but did not change the association between vaccination and anxiety, mood or other disorders. With further adjustment for comorbidities via cADGs, the association between psychotic (adjusted prevalence ratio 1.28, 95% CI 1.27–1.29) and substance disorders (adjusted prevalence ratio 1.49, 95% CI 1.48–1.50) and being unvaccinated increased, and the association with mood and other shifted closer to the null. After adjustment for age and sex, individuals with a prior history of a mental health–related emergency department visit (adjusted prevalence ratio 1.33, 95% CI 1.32–1.34) or hospital admission (adjusted prevalence ratio 1.38, 95% CI 1.37–1.39) were more likely to be partially vaccinated or unvaccinated, and this high likelihood was attenuated with the inclusion of neighbourhood income quintile and homelessness (Figure 2B, Table 1). Further adjustment for comorbidities via cADGs increased the association between MHA-related emergency department visits (adjusted prevalence ratio 1.42, 95% CI 1.41–1.42) and hospital admissions (adjusted prevalence ratio 1.40, 95% CI 1.40–1.41) and being unvaccinated, and the association with outpatient visits became null.
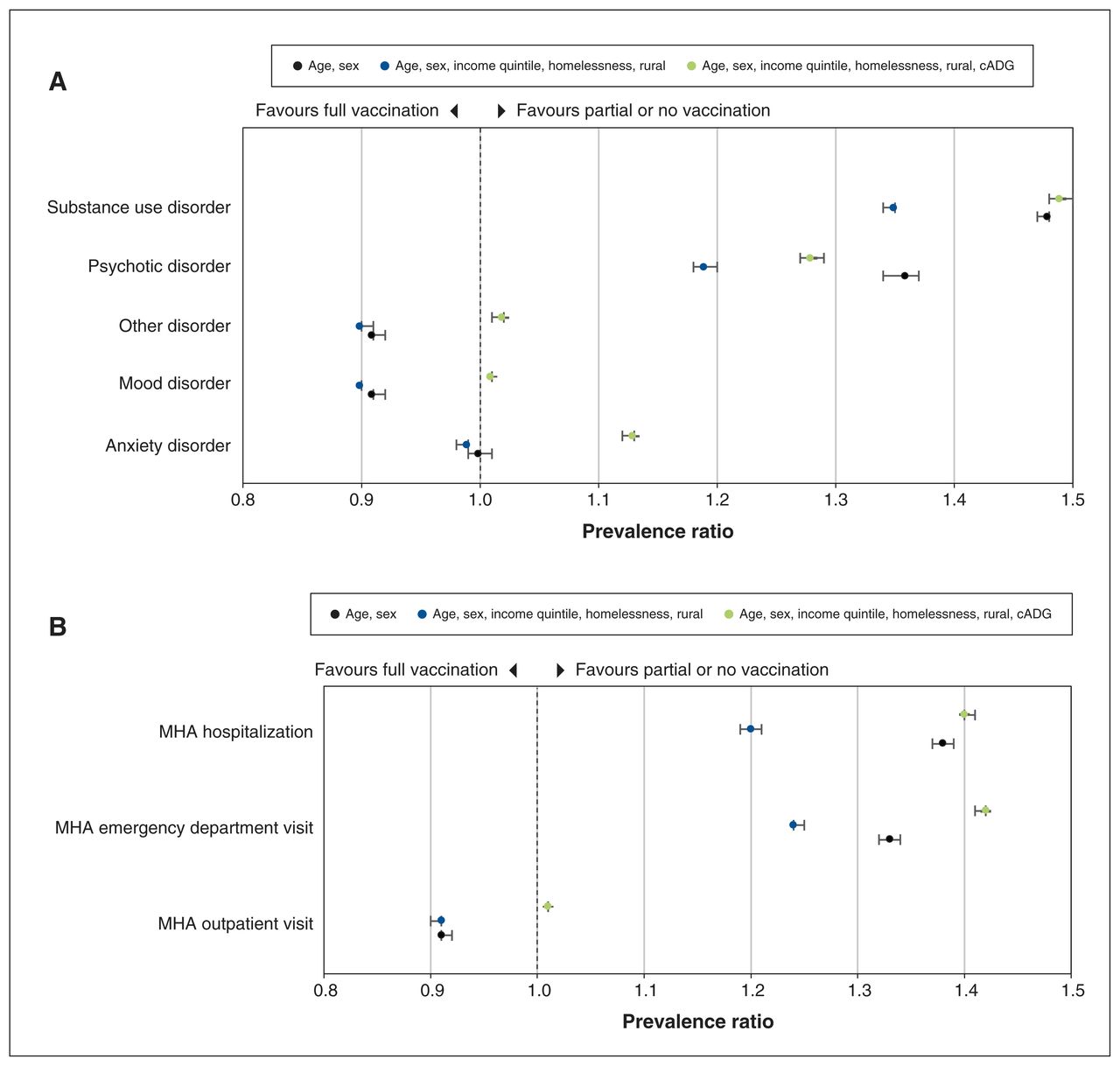
Relative prevalence* of partial and no vaccination by (A) diagnostic category and (B) mental health and addiction (MHA) severity. *Relative prevalence estimated using modified Poisson regression models, with no mental health disorders as the reference category. Note: cADG = collapsed Aggregated Diagnosis Group.
Modified Poisson regression models assessing the association between mental health and addictions service use history and the prevalence of partial or no vaccination against SARS-CoV-2 in Ontario, Canada
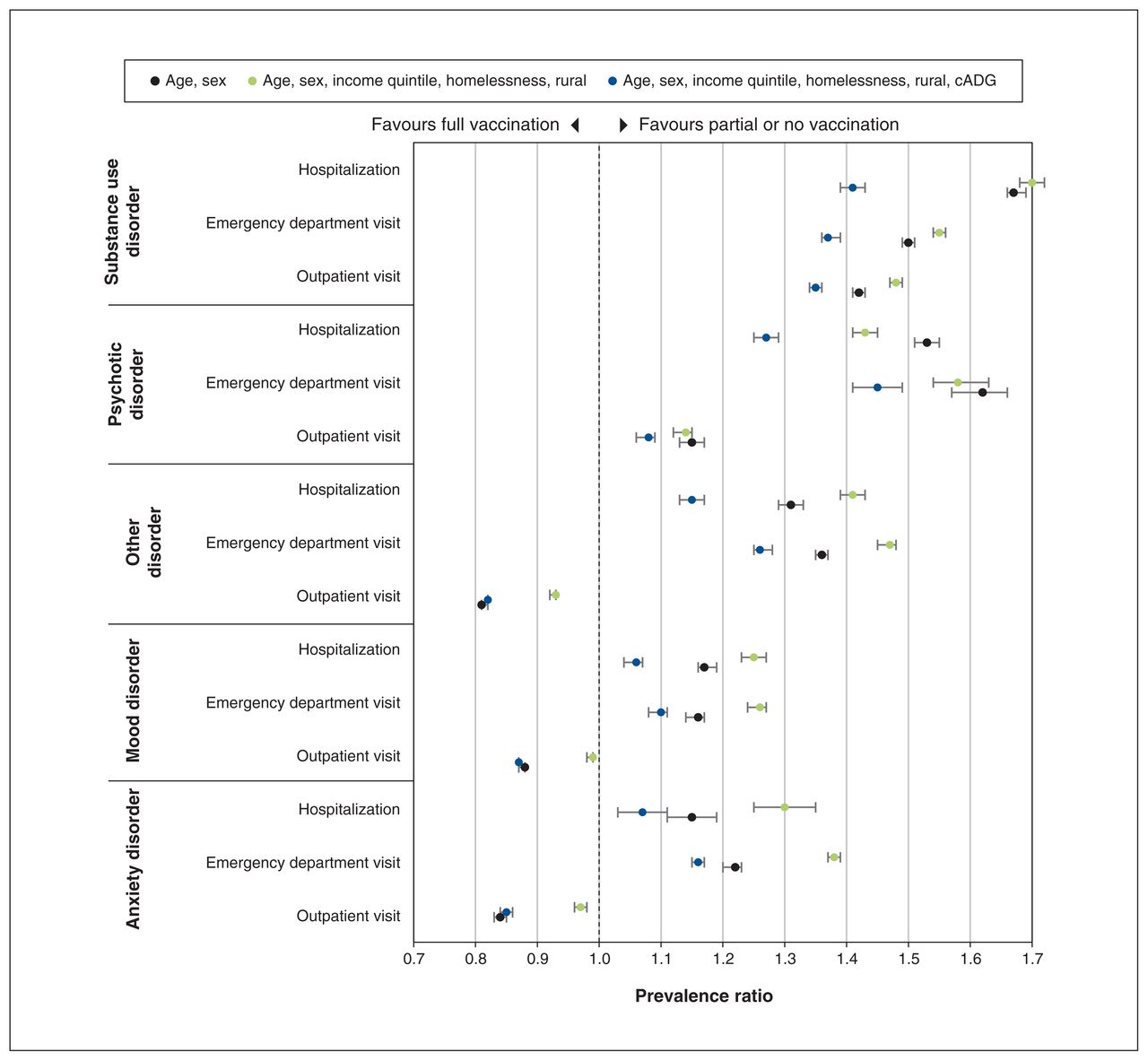
The effect of prior mental health service utilization severity within each diagnostic category on vaccination status is presented in Figure 3. A history of service use related to substance use or psychotic disorder was associated with higher prevalence of being partially vaccinated or unvaccinated across all severity categories. A history of service use related to mood, anxiety and other disorders was associated with a slightly higher prevalence of being partially vaccinated or unvaccinated among individuals with a history of emergency department visits and hospitalizations. However, a history of service use related to these disorders in the outpatient category was associated with a lower prevalence of being partially vaccinated or unvaccinated; these results were attenuated after adjustment for comorbidities.
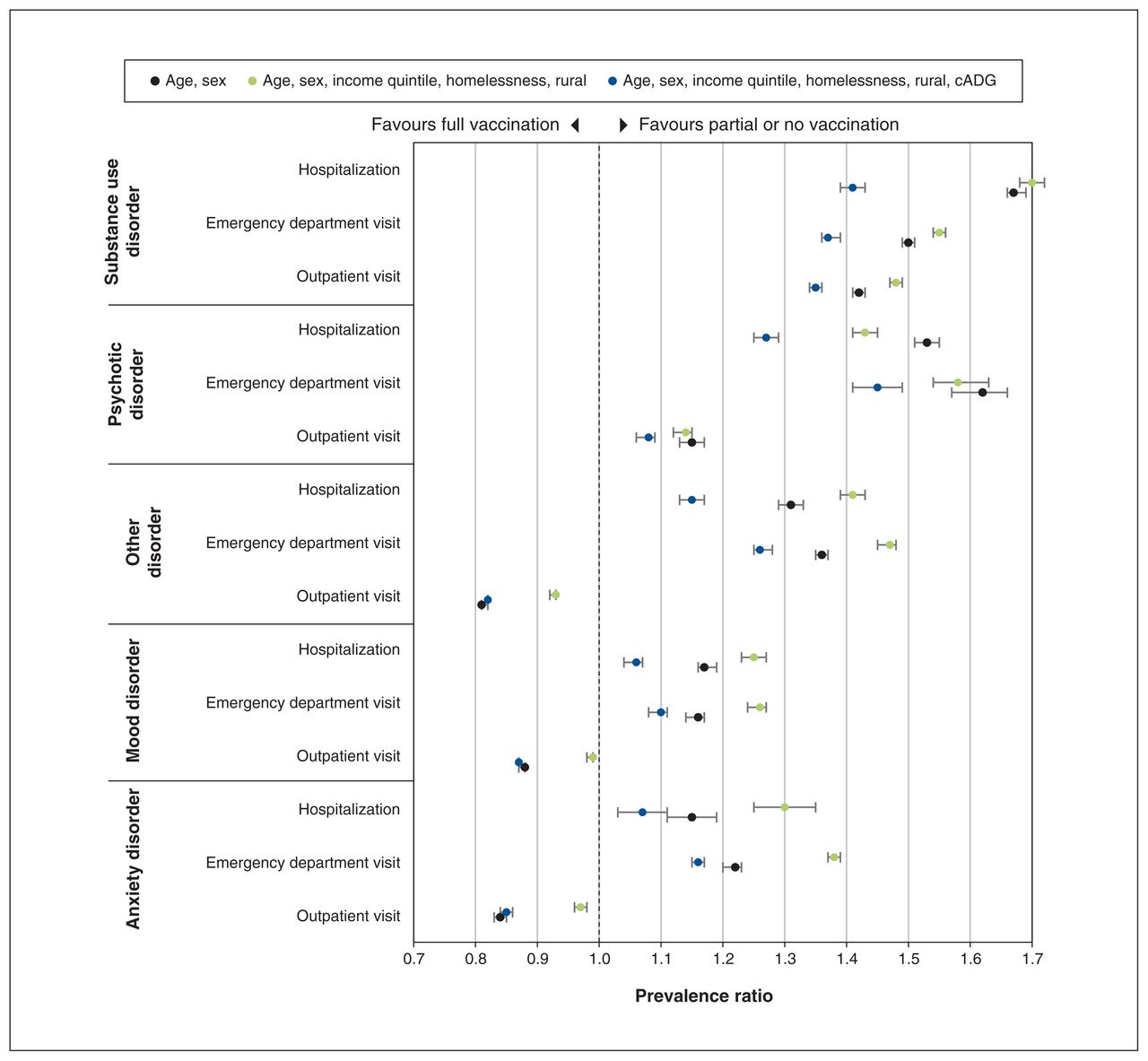
Relative prevalence* of partial and no vaccination by mental health and addiction diagnosis, stratified by health service utilization severity. *Relative prevalence estimated using modified Poisson regression models, with no mental health disorders as the reference category. Note: cADG = collapsed Aggregated Diagnosis Group.
In a sensitivity analysis with the definition of being vaccinated changed to having received 1 or more doses, the results were very similar to those in our main analyses (Appendix 5, available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1). The sensitivity analyses comparing the general population with individuals with schizophrenia and with individuals with alcohol-related disorder revealed vaccination prevalence ratios similar to our main findings for these diagnostic groups (Appendix 6, available at www.cmajopen.ca/content/11/6/E1066/suppl/DC1).
Interpretation
We found that more than one-third of individuals with a history of service use related to psychotic and substance use disorders were not fully vaccinated by Sept. 17, 2021. Individuals in the youngest age groups with a history of service use related to psychotic disorders and substance use disorders had an even lower prevalence of being fully vaccinated. Lower vaccination prevalence was also observed among individuals experiencing homelessness, those with a history of higher-acuity mental health or addictions service utilization, and those living in lower-income neighbourhoods. The lower vaccination prevalence observed among individuals with a history of service use related to substance use or psychotic disorders was only partially attenuated after adjustment for homelessness and income, suggesting that the low vaccination prevalence observed in these clinical populations may not be fully explained by sociodemographic factors known to decrease the likelihood of being vaccinated.
Our study also found that service use severity was associated with lower vaccination prevalence compared with individuals with no history of service use related to mental illness. The impact of health service utilization severity differed by diagnostic category, with individuals with substance use and psychotic disorders having lower vaccination prevalence across all severity categories. Individuals in the outpatient category related to mood, anxiety and other disorders were more likely to be vaccinated than individuals with no mental disorders. It is unclear why such individuals were more likely to be vaccinated, but this likely reflects the fact that people who seek care in outpatient services have greater comorbidity and are more likely to seek care generally, including vaccination during the pandemic.
Given the risk of early death among individuals with psychotic3 and substance use disorders,21 and the concern about the negative impact of SARS-CoV-2 on individuals with severe mental illnesses,22 the lower vaccination prevalence among these vulnerable individuals is concerning. In Ontario, these populations were not targeted, although individuals living in shelters were targeted. The lower vaccination prevalence among younger individuals with substance-related or psychotic disorders is particularly concerning. There is evidence that such low vaccination prevalence can be improved. In a Belgian study, authors found that among patients receiving services in mental health settings, vaccination uptake, when systematically and routinely offered, is as high as in the general population.23 In Ontario, neighbourhood-level data were used in near real time to tailor vaccine strategies to increase vaccination in neighbourhoods with low rates of vaccination.24 Given the evidence that when individuals with severe mental illnesses are offered vaccination they are likely to accept and that data can be used to target populations that are not accessing vaccinations at the rate of the general population, our findings suggest that individuals with severe mental illnesses, such as those with psychotic and substance use disorders, may similarly benefit from targeted vaccination programs.
Limitations
This study has several limitations. Our diagnostic categories have not been validated. Although they likely categorize individuals into broad diagnostic categories accurately, we cannot rule out misclassification. We conducted sensitivity analyses for the 2 diagnostic groups with low vaccination prevalence (psychotic and substance use disorders). We obtained similar results for the 2 different approaches to identifying individuals with substance use disorders and psychotic disorders, suggesting that the rate of misclassification is likely not a significant source of bias. Further, the diagnostic groups and severity categories are based on having received health services. As such, the diagnostic groups are biased based on access to health services; our finding of low vaccination prevalence among individuals with substance use disorders may be an underestimate given high rates of poor access to health care observed in this population,25 which future studies should address.
Similarly, we used a severity gradient exposure variable based on type of service utilization (hospital admission, emergency department visit and physician visit) that has not been validated. Assignment to a severity category (e.g., hospital admission) requires only 1 service encounter; illness severity is also likely reflected by the frequency of encounters in each given service type.
Identifying homelessness using health administrative data sources has low sensitivity and high specificity; the impact of homelessness on vaccination prevalence is likely underestimated in our study. Race and ethnicity are important determinants of vaccination status26 but are unavailable within the data used for this study. Future studies should incorporate alternative measures of homelessness and incorporate measures of race and ethnicity.
We excluded individuals residing in long-term care settings because this population had different vaccination schedules. This excluded group is important and worthy of separate investigation.27
We required individuals to be eligible for insured services in Ontario only as of Sept. 17, 2021. There is a possibility that individuals within the study sample may have been eligible for coverage, and therefore vaccinations, only immediately before our study date and thus would have been included in our study but not eligible for vaccinations. This is likely a rare situation and unlikely to occur with greater frequency in our MHA-related groups versus controls.
Finally, our data linkage rate was high overall (93.6%). However, the linkage rate may be lower in marginalized populations, which may underestimate vaccination prevalence in these populations.
Conclusion
We observed low vaccination prevalence among individuals with a history of substance use and psychotic disorders, but not among the other psychiatric diagnostic categories we studied. We also observed low vaccination prevalence among our younger age category and among individuals experiencing homelessness, those with more severe mental illness and individuals living in lower-income neighbourhoods. The low vaccination prevalence observed among individuals with substance use or psychotic disorders was only partially explained by sociodemographic variables known to be associated with low vaccination prevalence (e.g., homelessness and low income). Efforts to ensure that individuals with substance use or psychotic disorders have access to vaccinations, while challenging, are critical to reduce the risk of death and other adverse consequences of SARS-CoV-2 infection in this high-risk population.
Acknowledgement
The authors acknowledge Public Health Ontario for access to case-level vaccination data.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Paul Kurdyak conceptualized and designed the study, interpreted the results and drafted the initial manuscript. Michael Lebenbaum, Laura Rivera, Damon Scales and Astrid Guttmann conceptualized and designed the study and interpreted the results. Aditi Patrikar designed the study, analyzed the data and interpreted the results. Hong Lu analyzed the data and interpreted the results. All authors revised the article, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. This work is supported by the Ontario Health Data Platform (OHDP), a Province of Ontario initiative to support Ontario’s ongoing response to COVID-19 and its related impacts.
Data sharing: The data set from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors on request, understanding that the computer programs may rely on coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/6/E1066/suppl/DC1.
Disclaimer: Parts of this material are based on data and information compiled and provided by the Ontario Ministry of Health, the Canadian Institute for Health Information and Public Health Ontario. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of ICES, the OHDP, or the funding or data sources; no endorsement is intended or should be inferred.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.