


Abstract
Background: Pre-exposure prophylaxis (PrEP) for HIV is underutilized. We aimed to identify barriers to use of PrEP and strategies that may facilitate its uptake.
Methods: Gay, bisexual and other men who have sex with men, aged 19 years or older and living in Ontario and British Columbia, Canada, completed a cross-sectional survey in 2019–2020. Participants who met Canadian PrEP guideline criteria and were not already using PrEP identified relevant barriers and which strategies would make them more likely to start PrEP. We described the barriers and strategies separately for Ontario and BC.
Results: Of 1527 survey responses, 260 respondents who never used PrEP and met criteria for PrEP were included. In Ontario, the most common barriers were affordability (43%) and concern about adverse effects (42%). In BC, the most common reasons were concern about adverse effects (41%) and not feeling at high enough risk (36%). In Ontario, preferred strategies were short waiting time (63%), the health care provider informing about their HIV risk being higher than perceived (62%), and a written step-by-step guide (60%). In BC, strategies were short waiting time (68%), people speaking publicly about PrEP (68%), and the health care provider counselling about their HIV risk being higher than perceived (64%), adverse effects of PrEP (65%) and how well PrEP works (62%).
Interpretation: Concern about adverse effects and not self-identifying as having high risk for HIV were common barriers, and shorter waiting times may increase PrEP uptake. In Ontario, the findings suggested lack of affordability, whereas in BC, strategies involving health care providers were valued.
Pre-exposure prophylaxis (PrEP) for HIV using tenofovir disoproxil fumarate–emtricitabine is highly effective at reducing the risk of HIV infection1–3 and has been approved for daily use in Canada since 2016. However, despite a significant increase in the number of PrEP users in the past years,4,5 it is estimated that far more people could benefit from using PrEP.6,7 Barriers to PrEP uptake exist at the individual, interpersonal, community and structural level.8 At the individual level, lack of awareness, perceived lack of efficacy, concern about adverse effects and low HIV risk perception are common. At the interpersonal level, there is fear of risk compensation (increase in risk-taking behaviours as a result of a decrease in perceived risk) and stigma from peers, family and friends. At the community level, barriers include mistrust of the pharmaceutical industry and medical establishment, and inadequate access to health care providers experienced in working with sexual or gender minorities. In addition, providers’ lack of awareness or training, lack of referral pathways, concern about risk compensation and concern about patient adherence can be barriers.9,10 Finally, at the structural level, issues of affordability (e.g., in Ontario PrEP is not fully funded), institutionalized racism and discrimination, and structural stigma play a major role in the disparate access to and limited uptake of PrEP.8,11–18
All such barriers are potentially modifiable, with some requiring more individual-focused actions, such as education and health promotion with individuals who could benefit from PrEP, and others operating at the policy level, such as full public funding for PrEP. To decide what methods and strategies could help individuals who are at risk of HIV infection to access PrEP, it is necessary to describe the key determinants and the barriers to access and use. Relevant methods could be empowerment, improving perceived relevance, influencing the reference group or redesign of services;19–21 and the strategies that can translate such methods into actions include counselling, peer education, information provision, having role models and the availability of guides, among others.19–21 An important component of such intervention planning is to consider end users’ (in this case, potential PrEP users’) preferences regarding what strategies might have an impact on their decision to initiate PrEP. The aims of this analysis were to identify the barriers to PrEP use among gay, bisexual and other men who have sex with men (GBM) who have never used PrEP and who met Canadian guideline criteria,6 to identify strategies most likely to influence their decision to start using PrEP and to explore differences between Ontario and British Columbia, Canada.
Methods
This is a descriptive study based on an open voluntary survey of nonusers of PrEP identified from the PrEP Implementation Project (PRIMP). The PrEP Implementation Project is a multicomponent study investigating strategies for increasing PrEP uptake among urban GBM in Ontario and BC. One component is an open voluntary cross-sectional survey, which recruited participants from Toronto, Ottawa and Hamilton in Ontario, and Vancouver and Victoria in BC. These cities were selected because they are the largest urban centres in the 2 largest English-speaking provinces in Canada, and also because of their differential medication-coverage policies (PrEP is universally covered in BC but not in Ontario). In BC, antiretroviral medications for HIV treatment and prevention (including PrEP) are publicly funded by the BC HIV Drug Treatment Program administered by the BC Centre for Excellence in HIV/AIDS,22 a program available to all residents. This program is widely known among providers at sexual health clinics but not to the same extent among other health care providers. Other medications are covered through BC PharmaCare, a provincially funded program for residents, which covers a percentage of medication costs (70%–100%, depending on income and amount paid out of pocket).23 In Ontario, PrEP is covered by the Ontario Drug Benefit in certain circumstances (e.g., people aged < 25 or > 65 yr, and people who are part of the Ontario Disability Support Program, among others).24,25 Across Canada, approximately 60% of individuals have private medication coverage through employment. 26 Among insurers, there is considerable variation in the requirements and the extent to which drugs are subsidized, which has led some scholars to describe the current system as inefficient and as a “confusing patchwork.”27,28 Furthermore, other groups, such as international students or visitors, do not have comprehensive medication coverage.
Participants
Recruitment took place between July 2019 and August 2020. Potential participants were recruited via various means, including English-language posters and information cards distributed in sexual health clinics, advertisements on popular GBM dating apps (Grindr and Scruff), and via social media (Facebook) promotion by collaborating community organizations. Responses were automatically stored into REDCap housed on secure servers at the University of British Columbia, and questions were adapted based on responses to other items using branching logic. The survey was tested for usability and technical functionality, and allowed participants to navigate back and forth. The survey was further pilot-tested for understandability and appropriateness of language by members of the PRIMP Community Advisory Board.
Participants were eligible for inclusion in the PRIMP survey if they were 19 years of age or older; identified as a cisgender man, transgender man or transgender woman; were able to communicate in English; reported sex with a man in the past 6 months; and provided consent. Volunteers or employees of any community health services organization were excluded. Participants were offered a Can$10 gift card as compensation for their time.
For the present analysis, we included GBM who had never used PrEP at the moment of the survey and who were considered eligible for PrEP according to the Canadian guidelines for PrEP,6 given that they represent the group that could benefit the most from understanding barriers and facilitators to PrEP uptake. Eligibility for PrEP, as per the guidelines, was defined as condomless anal sex in the past 6 months plus any of the following: infectious syphilis, rectal gonorrhea, rectal chlamydia, repeated use of nonoccupational postexposure prophylaxis, or scoring 11 or greater on the High Incidence Risk Index for Men Who Have Sex with Men (HIRI-MSM).29 The HIRI-MSM score is a metric used to determine HIV risk based on number of sexual partners, condomless anal sex with HIV-positive or-negative partners, age and drug use.29
Variables
We asked participants about their reasons for not using PrEP and what strategies would influence their decision to start PrEP, using a predefined list (Appendix 1, available at www.cmajopen.ca/content/11/3/E560/suppl/DC1). This list was developed by consensus among the study investigators based on extensive previous experience working with GBM in the context of sexual health clinics and PrEP clinics in Canada, and a review of published literature.11,13 The list of barriers and mitigation strategies included items at the individual, interpersonal and structural levels, as described above.
For the reasons for not using PrEP, participants were asked to select all options that applied to them. For strategies that could influence their decision to start PrEP, they were asked to state whether each strategy would make them more likely to start PrEP or less likely, or if it would not have any impact. The latter 2 options were merged into 1 category since the number of individuals indicating strategies making them less likely to start PrEP was very low. The survey also included questions about sociodemographic variables and sexual health. All the variables used to determine PrEP eligibility, according to the Canadian guideline for PrEP described above, were measured individually in the survey.
Sample size
Sample size for the PRIMP survey was calculated based on the expected number of participants needed to estimate proportions of the overall sample reporting PrEP awareness, acceptability and usage with reasonable precision, based on previous surveys.30,31 This resulted in a sample size of 250 participants in each city (1250 in total) to estimate these proportions with adequate precision. However, the present subanalyses include only respondents who had never used PrEP who met criteria for PrEP according to the Canadian guideline for PrEP.6
Data analysis
Data are presented for the entire study subsample and stratified by province. For continuous variables, mean and standard deviation or median and interquartile range (IQR) are presented, depending on their distribution. Categorical data are presented as counts and percentages. We analyzed and present available data for each individual variable.
Ethics approval
This study was reviewed and approved by the research ethics boards of Clinical Trials Ontario, Unity Health Toronto, University Health Network, Toronto Public Health, University of Toronto, York Region, University of British Columbia and University of Victoria (REB 18-346). Study data are stored on a secure, password-protected server at St. Michael’s Hospital in Toronto.
Results
In total, 260 participants who had never used PrEP and met criteria for PrEP were included in the analysis (17% of the overall PRIMP sample) (Figure 1). Of the respondents, 184 were from Ontario (140 from Toronto, 31 from Ottawa and 13 from Hamilton), and 76 were from BC (65 from Vancouver and 11 from Victoria). The median age was 31 (IQR 26–38) years, and 61% had at least a bachelor’s degree. In both provinces, most were White (57%). Private drug insurance (59%) and out of pocket (27%) were the most common forms of paying for medications (Table 1).
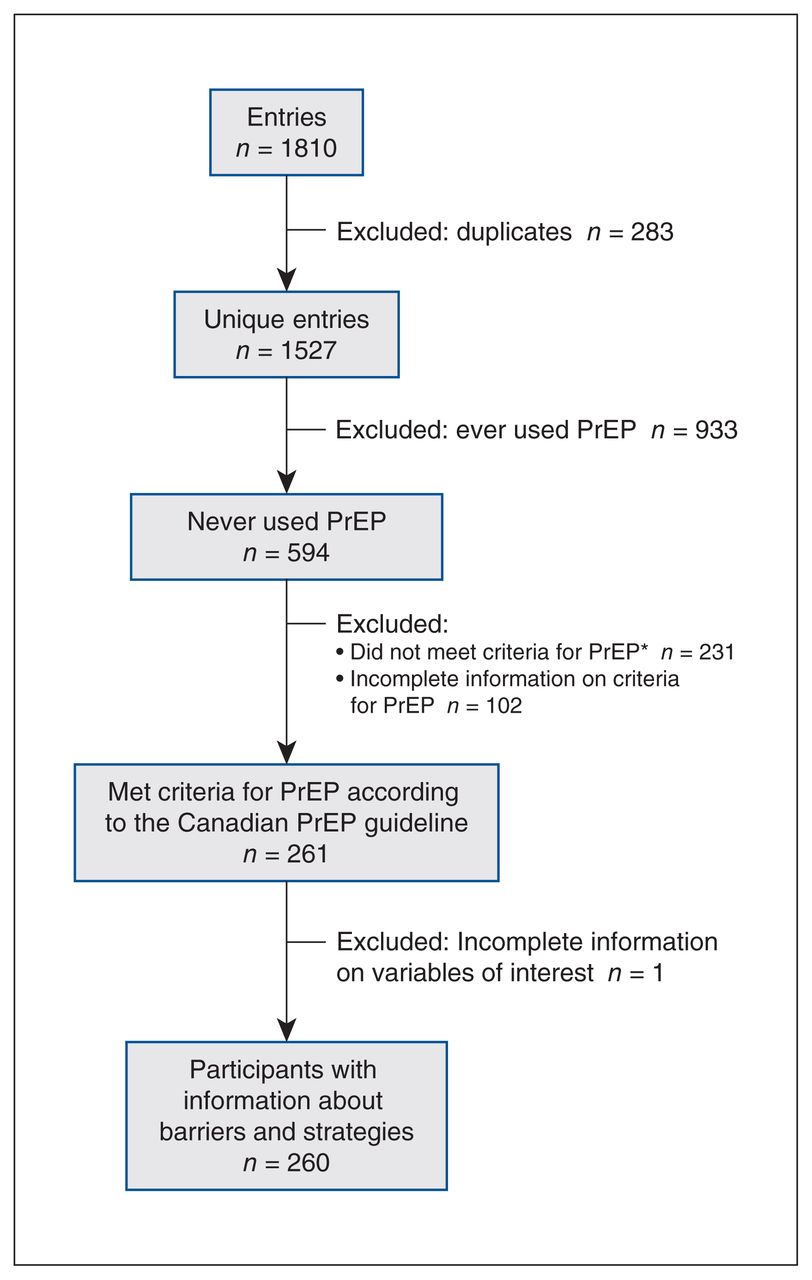
Flowchart of survey participants. *Mean HIRI-MSM score = 6.3 (standard deviation 4.0). Note: HIRI-MSM = High Incidence Risk Index for Men Who Have Sex with Men, PrEP = pre-exposure prophylaxis.
Sociodemographic characteristics of study participants, in total and stratified by province
Descriptive and comparative analyses of PrEP eligibility are shown in Table 2. The proportion of participants who were eligible for PrEP was 55% in Ontario and 48% in BC. Eligibility for PrEP was determined as per the Canadian guideline for PrEP, by reporting condomless anal sex in the past 6 months and 1 or more of the following: a prior diagnosis of bacterial sexually transmitted infection (syphilis, rectal gonorrhea or rectal chlamydia) in 99 (38% of the sample), prior recurrent nonoccupational postexposure prophylaxis use in 15 (6%) and HIRI-MSM score of 11 or greater in 256 (98%).
High Incidence Risk Index score, sexually transmitted infections and use of postexposure prophylaxis among study participants, in total and stratified by province*
In Ontario, the most common reason for not using PrEP was cost (43%), unlike in BC, where cost was reported as a barrier by 16% (Table 3). Other common reasons were concern about adverse effects (42% in Ontario and 41% in BC) and not feeling at high enough risk (27% in Ontario and 36% in BC). Unwillingness to take a pill regularly was also common in BC (24%) (Table 3).
Reasons for not using pre-exposure prophylaxis among study participants, in total and stratified by province
Strategies that might influence participants’ decision to start PrEP are shown in Table 4. In Ontario, these were short waiting time (63%), health care providers informing them about their HIV risk being higher than perceived (62%) and a written step-by-step guide on how to access PrEP (60%). In BC, these were short waiting time (68%), people speaking publicly about PrEP (68%), and their health care provider counselling them about their HIV risk being higher than perceived (64%), adverse effects of PrEP (65%) and how well PrEP works (62%).
Strategies that would more likely influence the decision to start pre-exposure prophylaxis among study participants, in total and stratified by province
Interpretation
In this community-based sample of GBM in 5 large cities in Ontario and BC, we found that around half of respondents who had never used PrEP met evidence-based criteria for PrEP initiation (55% in Ontario and 48% in BC). Concern about adverse effects, affordability and not feeling at high enough risk were the most common barriers to PrEP uptake. Short waiting time was the most preferred strategy to increase PrEP uptake. Other strategies included health care providers informing clients about their HIV risk being higher than perceived, and counselling about adverse effects of PrEP and how well PrEP works, written guides and people speaking publicly about PrEP. The largest observed difference between the provinces was affordability as a reason for not using PrEP.
Despite a reportedly similar distribution of type of medication coverage in both provinces, affordability was much more commonly reported as a barrier to PrEP in Ontario than in BC. In Ontario, 43% of participants identified cost as a reason for not accessing PrEP (in contrast to 16% in BC). According to the literature, only 23% of PrEP users in Ontario access it through the province’s public drug programs, which some residents may be eligible for on the basis of age or income.4 In contrast, in BC, PrEP is publicly funded if clinical criteria based on the Canadian guideline for PrEP are met,22 through a special program distinct from the public drug insurance used for most other medications, making it one of only a few provinces or territories in Canada where PrEP is fully funded.22,32–34 Nevertheless, affordability was cited as a barrier to PrEP uptake in 16% of BC respondents, possibly owing to lack of awareness about the existence of the BC Centre for Excellence in HIV/AIDS PrEP program, reasons related to immigration status, costs associated with accessing the medication (e.g., travel costs to attend appointments or to pick up the prescription) or interprovincial portability policies.35
Concern about adverse effects was the most common reason for not using PrEP in the overall sample. This finding suggests that more public education is required regarding PrEP’s generally favourable adverse effect profile, perhaps emphasizing that the most common regimen of PrEP, tenofovir disoproxil fumarate–emtricitabine, does not carry a risk of serious adverse events higher than placebo.1–3 In this regard, the main tolerability issue associated with PrEP is gastrointestinal upset, which tends to be mild and resolves spontaneously within the first month (reported by 2%–14% of users, according to the literature).36 In addition, although more long-term data are needed, the asymptomatic renal and bone toxicities of tenofovir disoproxil fumarate–emtricitabine include slight elevations in creatinine (in 18% of users, according to the literature)37 and modest decreases in bone mineral density that are generally reversible with drug discontinuation and can generally be monitored and managed clinically.1,36–39 The adverse effect profile is similar for on-demand tenofovir disoproxil fumarate–emtricitabine (2 pills before sexual activity and 1 pill per day for 2 days after).3 Furthermore, a more recent form of PrEP, emtricitabine–tenofovir alafenamide, has shown a slightly better safety profile than tenofovir disoproxil fumarate–emtricitabine in terms of creatinine levels and bone density.2 Whereas concerns about adverse effects might be mitigated by providing more information about PrEP, the collective memory of adverse effects related to HIV treatment and medical mistrust may be important contributing factors to such concerns.15,16
Not feeling at high enough risk was common among the study participants. Whereas some of the respondents who had never used PrEP were, in fact, at low risk of HIV infection, including those in monogamous relationships or those with consistent condom use,6,40 many GBM may underestimate their risk.6 This misalignment between the potential user’s and the clinician’s perspectives has been previously described in the literature as one of the main barriers to PrEP uptake41 but requires deeper study.
Participants in both provinces reported that short waiting times may increase their likelihood of starting PrEP. Our data show that the median waiting time from the moment a person decides to go on PrEP until they get a prescription ranges between 7 days and 2 months.42 Further, potential users may feel discouraged if they cannot access PrEP directly from their primary care provider, especially if there is already some hesitancy to start PrEP. Although not without limitations, interventions such as telemedicine or decentralization of access to PrEP through engagement of other health care professionals, pharmacists, HIV testing sites or community organizations could reduce waiting times.43
In BC, a large proportion of participants reported that having their health care provider informing them about how well PrEP works, counselling them about adverse effects and informing them about their HIV risk being higher than perceived would positively influence their decision to start PrEP. The latter was also commonly reported in Ontario.
Universal PrEP access across Canada is urgently required to address fundamental barriers to health equity. Despite the various programs to cover the cost of PrEP medications, individuals at risk who do not qualify for publicly funded programs for lower income groups may find themselves unable to access PrEP. Furthermore, understanding and navigating the medication coverage system in Canada can be confusing and discourage eligible GBM from using PrEP.27 Costs of deductibles and pharmacy dispensing fees may have a further impact on the ability to access PrEP. Even in the setting of universally funded PrEP such as in BC, perceived cost may be a barrier if individuals are unaware of its availability. This may have been particularly true in our sample of GBM who had never used PrEP. However, eliminating cost barriers alone is unlikely to result in a dramatic increase in uptake, unless other barriers are also addressed, as discussed below.
Our findings indicate that strategies aiming to improve PrEP uptake must be multicomponent, acknowledging practical challenges such as transportation barriers, and must build health care providers’ skills in patient counselling. Such counselling should acknowledge diversity of sexual behaviour and sexual identity among GBM, assess and address potential users’ concerns, encourage joint risk-reduction plans and provide follow-up. Short interventions containing some of these elements have been associated with an increase in providers’ abilities to discuss HIV prevention at HIV clinics.44 In contrast, stand-alone interventions such as informing high-risk GBM of their calculated risk, without further counselling, are not sufficient to increase PrEP uptake.45 Our findings also indicate the need for more innovative social marketing strategies. People speaking publicly about PrEP, and messaging about PrEP on social media and other channels using digital platforms could perhaps have a positive effect. Qualitative research could shed light on specific strategies for achieving these goals, and such work is underway as part of our PRIMP study initiative.
Limitations
Our findings may not be generalizable to smaller urban centres or rural areas, where other types of barriers may be more relevant. For instance, our sample was ethnically more diverse, had more years of formal education and reported a history of STIs more often than other samples in Canadian surveys among GBM.46 This is expected, since our sample comes from large urban centres, and participants were recruited from sexual health clinics and through advertisements on specific Internet platforms. Therefore, our results may not be representative of people not engaged in care, for whom we would anticipate that barriers such as cost would be even more important, or less active on social media, who possibly experience more difficulties accessing PrEP or information about PrEP. In addition, it is likely that those choosing to answer the survey differ from those who did not, although the degree of difference in HIV risk between responders and nonresponders is unknown. It would have been informative to ask current and former PrEP users what strategies were effective at motivating them to use PrEP. We do not believe that providing compensation for participating in the survey had a large influence on the final sample, as we do not believe the honorarium provided had an important effect on accepting risks derived from taking the survey that they would not have accepted otherwise. Finally, our study was not sufficiently powered to identify differences between subgroups; further studies are needed to explore differences in the role of affordability and acceptability of strategies to increase PrEP uptake on the basis of variables like ethnicity and socioeconomic status.
Conclusion
Concern about adverse effects and not feeling at high enough risk were common barriers in both provinces. In Ontario, the findings suggested structural issues such as affordability and accessibility. In BC, strategies involving health care providers were often valued. Future interventions must consider barriers on various levels, including potential users’ knowledge about and attitudes toward PrEP, the capacity of health care providers to provide information and prescribe PrEP, and what policies for medication coverage are in place.
Acknowledgement
The authors acknowledge that the land where this research took place is the traditional territory of many nations and is now home to many diverse First Nations, Inuit and Métis peoples.
Footnotes
Competing interests: Mark Hull reports funding from Gilead Life Science for an investigator-initiated study, paid to his institution. Dr. Hull is a member of a data safety monitoring board for the trial “M2HepPreP: a multi-site multi-setting RCT of integrated HIV prevention and HCV care for PWID.” Darrell Tan reports grants from AbbVie and Gilead to his institution for investigator-initiated research, and support to his institution from GlaxoSmithKline for participation in industry-sponsored clinical trials. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Oscar Pico-Espinosa analyzed the data and led the writing of the manuscript. Darrell Tan is the principal investigator of the PrEP Implementation Project (PRIMP) study. Darrell Tan, Mark Hull, Paul MacPherson, Daniel Grace and Nathan Lachowsky planned the study rollout. Saira Mohammed and Robinson Truong coordinated the data collection. Mark Gaspar analyzed the qualitative component of the PRIMP study and gave input for the interpretation of the data. All authors revised the manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This project received funding from the Canadian Institutes of Health Research. Darrell Tan is supported by a Tier 2 Canada Research Chair in HIV Prevention and STI Research. Daniel Grace is supported by a Canada Research Chair in Sexual and Gender Minority Health.
Data sharing: Data are confidential.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/3/E560/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.