


Abstract
Background: Endometriosis, a prevalent condition among females of reproductive age, may be associated with increased risk of cardiovascular disease (CVD) through chronic inflammation and early menopause. The objective of this study was to estimate the association between endometriosis and subsequent risk of CVD.
Methods: We conducted a population-based cohort study using administrative health data from Ontario residents from 1993 to 2015. We compared the incidence of CVD and cardiovascular health outcomes between females with endometriosis and 2 age-matched females without endometriosis. The primary outcome was hospital admission for CVD. Secondary outcomes included in-hospital CVD events of interest and emergency department visits for CVD. We used Cox proportional hazards models to estimate adjusted hazard ratios (HRs) between endometriosis and CVD events.
Results: We identified 166 835 eligible patients with endometriosis and matched 333 706 patients without endometriosis. The mean age of those with endometriosis was 36.4 years. Patients with endometriosis had a higher incidence of hospital admission for CVD (195 admissions/100 000 person-years) compared with those without endometriosis (163 admissions/100 000 person-years). Similarly, the incidence of secondary CVD events was slightly higher among patients with endometriosis (292 cases/100 000 person-years) than among those without endometriosis (224 cases/100 000 person-years). Females with endometriosis had an increased risk of hospital admission (adjusted HR 1.14, 95% confidence interval [CI] 1.10–1.19) and secondary CVD events (adjusted HR 1.26, 95% CI 1.23–1.30).
Interpretation: In this large, population-based study, endometriosis was associated with a small increased risk of CVD events. Future studies need to investigate potential etiological mechanisms and strategies to decrease long-term CVD risk in patients with endometriosis.
Cardiovascular disease (CVD) is the leading cause of premature death for females in Canada.1 Efforts to decrease CVD incidence necessitate identification of risk factors in younger populations, including those unique to females, given the difficulty in diagnosis and management in this population.2 An emerging CVD risk factor is endometriosis, a chronic, multisystemic inflammatory condition that affects about 10% of the female population.3,4 Endometriosis typically manifests as pelvic pain and infertility, and can have a substantial negative impact on quality of life.5,6 Studies indicate that patients with endometriosis have an altered lipid profile and are at higher risk for atherosclerosis. 7–9 In addition to inherent risk factors associated with endometriosis, medical and surgical endometriosis treatments place patients at risk of CVD.
To date, limited data exist on the association between endometriosis and cardiovascular risk. The Nurses’ Health Study (NHS) II identified that patients with laparoscopically confirmed endometriosis had a higher risk of myocardial infarction, angiographically confirmed angina, and coronary heart disease than those without endometriosis.10 The NHS cohort was predominantly of higher sociodemographic status, educated and with greater access to medical care than the general population; thus, results may not be generalizable. More recently, 2 population-based cohort studies in the United Kingdom and in Taiwan found an increased risk of CVD among patients with endometriosis compared with those without endometriosis.11,12
We sought to contribute to the growing body of evidence of an association between endometriosis and CVD using a population-based cohort study linking health administrative data sets from a diverse population in Ontario, Canada.
Methods
Study design and data sources
We conducted a population-based matched cohort study using administrative health data though ICES (https://www.ices.on.ca). ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze deidentified health care and demographic data for health system evaluation and improvement. A description of all data sources used can be found in Appendix 1, Table A1, available at www.cmajopen.ca/content/11/2/E227/suppl/DC1.
Study population
We identified patients aged 18–50 years with a diagnosis of endometriosis (exposed) between 1993 and 2015 based on hospital or outpatient records. These patients were matched to 2 females with no diagnosis of endometriosis (unexposed) by age (birth year) and geographical location of residence by census subdivision. We used data from the Ontario Health Insurance Plan (OHIP) to identify patients with endometriosis, namely if they had at least 2 medical diagnostic codes within 1 year code 617 of the International Classification of Diseases, 9th Revision [ICD-9] for an outpatient diagnosis and codes ICD-9-617 or ICD-10-N80 for an in-hospital diagnosis) or 1 hospital admission for endometriosis. We considered patients to have had surgical confirmation of disease if they had qualified for a medical diagnosis and had a qualifying surgical procedure at any time during the study period (Appendix 1, Table A2).
Patients were eligible for inclusion if they were registered with OHIP for at least 2 years before cohort entry to ensure an appropriate lookback window for exclusion. Exclusion criteria included CVD parameters before index diagnosis, endometriosis diagnosis before the study window and missing census subdivision data. We classified patients as living in urban or rural areas,13 and as immigrants (within previous 30 years) or born in Canada with information from the Immigration, Refugees and Citizenship Canada data set. Income quintile was assigned using the Postal Code Conversion File and census data set. The first date of diagnosis of endometriosis served as the index date.
Covariates
We obtained patient demographic information, including age, obesity, hypertension, diabetes, previous childbirth and gynecologic conditions (i.e., pelvic pain, fibroids, premature ovarian insufficiency) from administrative data records of health care encounters and hospital admissions. We obtained date of birth, date of death and health insurance eligibility from the Registered Persons Database. We determined hypertension and diabetes diagnoses using validated ICES cohorts, the Ontario Hypertension cohort and the Ontario Diabetes Database, respectively. We determined previous childbirth in Ontario using the MOMBABY data set.14 We obtained inpatient medical visits from the hospital discharge abstracts database (DAD), outpatient visits from OHIP database (physician fee-for-service claims), emergent visits from the Canadian Institutes of Health Information’s National Ambulatory Care Reporting System database (NACRS) and same-day surgeries from the Same Day Surgery Database (SDS) (Appendix 1, Tables A2, A3 and A4).
Outcomes
The primary outcome was hospital admission for CVD (i.e., acute myocardial infarction, stroke, congestive heart failure, percutaneous coronary intervention, coronary artery bypass graft surgery, ischemic heart disease and cerebrovascular disease). Secondary outcomes included secondary, in-hospital CVD events of interest (i.e., cardiac catheterization, unstable angina, ischemic stroke, hemorrhagic stroke, transient ischemic attack, atrial fibrillation, abdominal aortic aneurysm, peripheral artery disease and cardiac stent) and emergency department visits for CVD (i.e., for any cause coded under CVD). Outcomes were based on measures from the Cardiovascular Health in Ambulatory Care Research Team (CANHEART) study,15 and included information from DAD, NACRS, SDS and OHIP, using ICD-9 and ICD-10 codes (Appendix 1, Table A5). Data on emergency department visits are reported on a separate cohort of patients, as NACRS outcomes were only available starting July 2000. We excluded emergency department visits for hypertension and diabetes which were used in the CANHEART study, from our composite outcome of emergency department visits, given that we included patients with diabetes and hypertension at baseline in the study. Follow-up began on the index date of accrual and continued until the earliest of the end of study (Dec. 31, 2017), the date of death or the date of loss of OHIP eligibility. In all time-to-event analyses, for those without the outcome of interest, censoring occurred on the earliest of the above dates.
Statistical analysis
We compared characteristics by exposure group using standardized differences. We considered standardized differences greater than 0.10 to show evidence of imbalance between exposure groups on that covariate.16 We estimated cumulative incidence, accounting for the competing risk of death. We assessed statistical significance of differences in cumulative incidence by exposure using the Gray test. For each outcome, we calculated crude incidence rates of primary and secondary outcomes by exposure group. We used univariate and multivariable Cox proportional hazards models to estimate crude and adjusted hazard ratios (HRs) for the presence of endometriosis. We used a robust variance estimator to account for correlation between matched participants. We assessed proportional hazard assumptions graphically using log of negative log of survival probability versus log time curves, as well as by evaluating interactions between time and the primary exposure (endometriosis). In the multivariate models, we adjusted for age, parity, hypertension, diabetes, obesity and immigration status, as these variables are known to affect CVD risk.17–22 We conducted a sensitivity analysis to evaluate whether results differed by type of endometriosis diagnosis (medical v. surgical). We used a test for interaction to assess if the presence of a diagnosis of premature ovarian insufficiency, defined as menopause before age 40 years (OHIP billing code for menopause, ICD-9-627), after endometriosis diagnosis, or if age at endometriosis diagnosis modified the association between endometriosis and cardiovascular outcomes. Finally, we evaluated whether the proportion of those who died from CVD differed by exposure using the χ2 test.
Ethics approval
Study ethics approval was obtained from the Queen’s University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board (file no. 6029490).
Results
We included a total of 500 559 females in the study cohort, 166 853 with a diagnosis of endometriosis and 333 706 without (Figure 1). Baseline cohort characteristics are presented in Table 1. The average age at index date was 36.4 years. Baseline sociodemographic characteristics were similar by exposure. A higher proportion of patients with endometriosis were nulliparous (65.3%) than those without (59.6%). The proportion of patients with obesity, diabetes or hypertension at baseline was similar by exposure group.

Creation of study cohort. Note: CVD = cardiovascular disease, OHIP = Ontario Health Insurance Plan.
Baseline cohort characteristics
A higher proportion of patients with endometriosis had diagnoses of pelvic pain (55.8% v. 26.6%) and fibroids (29.2% v. 10.4%) before their index diagnosis of endometriosis and during follow-up than patients without endometriosis. Patients with endometriosis were more likely to undergo bilateral oophorectomy (19.5% v. 2.7%) or hysterectomy (46.6% v. 7.6%), and to receive a diagnosis of premature ovarian insufficiency (24.5% v. 9.8%) than those without endometriosis (Table 2). The mean age at menopause was slightly lower in the endometriosis group than the unexposed (42.97 yr v. 46.18 yr).
Cohort characteristics before and during follow-up period
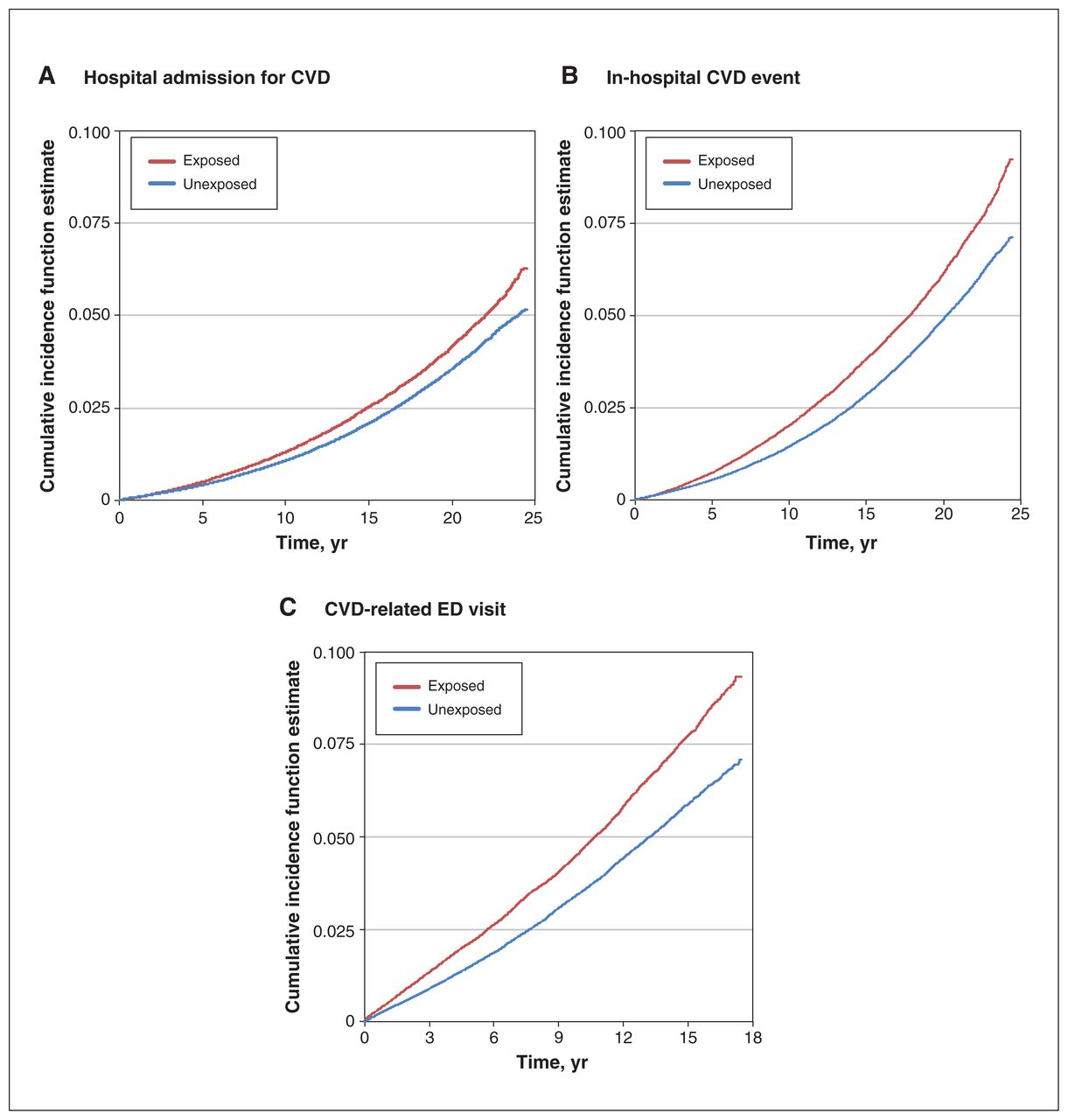
As shown in Figure 2, relative to females without endometriosis, those with endometriosis had a higher incidence of hospital admission for CVD, secondary CVD events and CVD-related emergency department visits. Detailed composite outcomes are found in Table 3. Patients with endometriosis had an increased risk of hospital admission for a major CVD event (adjusted HR 1.14, 95% confidence interval [CI] 1.10–1.19), secondary CVD event (adjusted HR 1.26, 95% CI 1.23–1.30) and CVD-related visits to the emergency department (adjusted HR 1.30, 95% CI 1.25–1.35), compared with those without endometriosis, when adjusted for parity, age, immigration status, hypertension, diabetes and obesity at baseline (Figure 2, Figure 3). In the sensitivity analysis, our results did not differ by method of diagnosis of endometriosis (medical v. surgical), suggesting no misclassification (Table 4). However, the risk of emergency department visits was higher in the medically diagnosed group (Table 4).

Incidence per 100 000 person-years and hazard ratios (HRs) for hospital admission for cardiovascular disease (CVD), in-hospital CVD events and CVD-related emergency department (ED) visits among females with endometriosis (exposed) and those without endometriosis (unexposed). Note: CI = confidence interval, Ref. = reference.
Cardiovascular disease–related outcomes among patients with and without endometriosis

Cumulative incidence estimates of (A) hospital admission for cardiovascular disease (CVD), (B) in-hospital CVD events and (C) CVD-related emergency department (ED) visits among females with endometriosis (exposed) and those without endometriosis (unexposed). The Gray test showed significant differences for all outcomes (p < 0.0001).
Sensitivity analysis for method of diagnosis of endometriosis
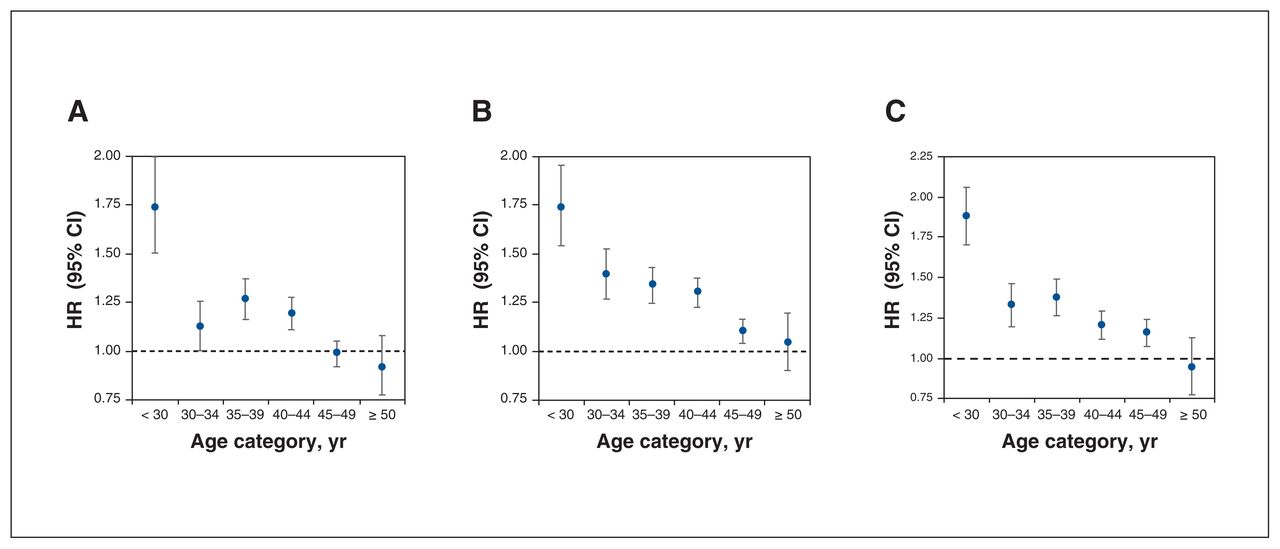
The presence of premature ovarian insufficiency did not modify the association between endometriosis and the studied outcomes (Appendix 1, Table A6). Adjusted models suggested that patient age at the time of endometriosis diagnosis affected the risk of any major outcome (hospital admissions for CVD, secondary CVD events of interest and CVD-related visits to the emergency department), with risk decreasing with increasing age of endometriosis diagnosis (Figure 4, Table 5).

Hazard ratios (HRs) comparing females with endometriosis (exposed) and those without endometriosis (unexposed) by age group for (A) hospital admission for cardiovascular disease (CVD), (B) in-hospital CVD events and (C) CVD-related emergency department (ED) visits. Note: CI = confidence interval.
Hazard ratios comparing females with endometriosis (exposed) versus those without endometriosis (unexposed)
The proportion of those who died from CVD did not differ between groups at 2.46% in the exposed group (1.78% among those with medical diagnoses, 2.60% among those with surgical diagnoses) and 2.47% in the unexposed group (p = 0.87).
Interpretation
Endometriosis was associated with a higher risk of hospital admission for CVD, secondary CVD outcomes and CVD-related emergency department visits. Risks of these adverse CVD outcomes were not different for patients whose endometriosis was diagnosed medically or surgically. Risk of CVD appears to be correlated with timing of endometriosis diagnosis, with higher risk among those who received their diagnoses at earlier ages.
Our findings agree with results from the NHS in the United States, which found that the risk of combined CVD outcomes was higher in a population with laparoscopically confirmed endometriosis relative to those without endometriosis (relative risk 1.62, 95% CI 1.39–1.89).10 Similarly, 2 recent population-based studies in Taiwan and the UK also found higher risks of CVD for women with endometriosis (HR 1.17, 95% CI 1.05–1.29 and HR 1.24, 95% CI 1.13–1.37, respectively).11,12 The higher relative risk in the NHS may be explained by the entirety of the exposed population in that study requiring a surgical diagnosis, which could indicate more severe disease. As in our cohort, both the NHS and the UK study found modification of this association by age, with the highest risk among those whose endometriosis was diagnosed when they were younger than 40 years.
Unfortunately, the delay in diagnosis of endometriosis is still a serious problem, and females may have endometriosis symptoms and, thus, be exposed to untreated inflammation and oxidative stress in the years before diagnosis. Analyzing the age of diagnosis is the closest available proxy measurement for length of exposure based on diagnostic coding with administrative health data. Prospective collection of individual patient data is required to more accurately determine longevity of symptoms and, hence, duration of exposure.
Our study cohort included a large number of participants, followed for a maximum of 22 years and consisting of a socioeconomically diverse population in the context of a publicly funded health care system, minimizing confounding from socioeconomic status.23,24 Although we did not collect data on ethnicity, our cohort is likely ethnically diverse, given that Canada has the highest proportion of foreign-born populations among the G8 countries (20.6%).25 The use of administrative health data sets to define endometriosis has been previously validated by comparing ICD codes with medical records in Sweden and Canada.26,27 Further, our study included females whose endometriosis was diagnosed not only by laparoscopy but also clinically. There is growing acceptance that a clinical diagnosis of symptomatic endometriosis is sufficient and, perhaps, more reliable than previously recognized. 28–30 Despite potential earlier diagnosis, earlier treatment or less severe disease, our results indicate that patients with medically diagnosed endometriosis are still susceptible to the same endometriosis-related risk factors for CVD.
Our study does not address the potential mechanism of the association between endometriosis and CVD. Whether inherent risks associated with dysregulated immune system are associated with both CVD and endometriosis, or whether endometriosis itself worsens CVD is yet to be determined. Associations could include dysregulated inflammation, increased reactive oxygen species and an unfavourable lipid profile.7,31 Additional factors may include treatment modalities used to manage endometriosis, including regular NSAID and opioid use.3,32–34
Given the role of surgical management in endometriosis, it was not surprising that, in our population, more patients with endometriosis had hysterectomies, oophorectomies and premature ovarian insufficiency than those in the unexposed group. As previously shown in the Women’s Health Initiative cohort,35 and the Canadian Longitudinal Study on Aging (CLSA),36 females who eventually undergo a hysterectomy have been shown to have a worse cardiovascular risk profile and higher incidence of CVD. This supports other studies that suggested hysterectomy and oophorectomy among younger females with endometriosis may increase the risk of coronary heart disease.10 Although premature ovarian insufficiency is a risk factor for CVD, it did not appear to modify the effect of endometriosis in our cohort. Patients with premature ovarian insufficiency may receive treatment such as hormone replacement therapy, which can reduce the risk of CVD. Further studies are required to determine whether treatment for premature ovarian insufficiency affects CVD risk among patients with endometriosis.
Although our findings suggest that patients with endometriosis have higher risk of CVD morbidity, risk of death from CVD occurs at an older age, which is outside the age range of follow-up in this study.37 Although death from CVD may occur later in life, CVD morbidity can remain substantial, even at younger ages.38 Studies with a longer follow-up duration are required to elucidate the long-term risk of CVD-related death in this population.
Limitations
We collected data through December 2015 to allow for follow-up for CVD outcomes. The association between endometriosis and CVD risk is unlikely to differ in more recent data, but clinical practice has changed since 2015 to improve earlier diagnosis of endometriosis; thus, recent data may be subject to less misclassification among those classified as not having endometriosis. Our study lacked information about modifiable lifestyle risk factors for CVD such as smoking, diet and exercise. Furthermore, we did not include information on stage of endometriosis or treatment used — including nonsteroidal anti-inflammatory drugs (NSAIDs), opioids or gonadotropin-releasing hormone agonists or antagonists, which may affect the risk of CVD — a limitation of administrative health data sets to study endometriosis.32,33,39,40 Similarly, indications for surgery (i.e., oophorectomy or hysterectomy) are not included in the data set, and although we assumed that, among those with endometriosis, these surgeries were completed for endometriosis, this is not confirmed. Finally, our data set measures were based on those used in the CANHEART study. Although these codes have been used previously, and are used by Statistics Canada, they have not yet been directly validated.41–46
Conclusion
Endometriosis is a multisystemic disease of chronic inflammation. Our findings suggest that this disease could be associated with an increased risk for earlier onset of CVD, and should be investigated as a potential sex-specific factor in CVD screening.
Footnotes
Competing interests: Olga Bougie reports funding from the Canadian Institutes of Health Research, the Society of Endometriosis and Uterine Disorders, SRI International and the Southeastern Ontario Academic Medical Organization. She also reports consulting fees from AbbVie and honoraria from Hologic, AbbVie and Bayer. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Jessica Blom, Maria Velez, Jessica Pudwell, Susan Brogly and Olga Bougie contributed to the conception and design of the work. All authors contributed to data analysis and interpretation. Jessica Blom drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by the Canadian Institutes of Health Research, Institute of Gender and Health (WHC-394408). The funder had no role in the study design, in the collection, analysis and interpretation of data, reporting, writing, or in the decision to submit the article for publication.
Data sharing: The data set from this study is held securely in coded form at ICES. Although data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS. The full data set, creation plan and underlying analytic code are available from the authors upon request, with the understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This document used data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation, and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File, which contains data copied under license from Canada Post Corporation and Statistics Canada. Parts of this material are based on data and information compiled and provided by the MOH and MLTC, the Canadian Institute of Health Information, the Ontario Health Insurance Program, and Immigration, Refugees and Citizenship Canada permanent resident (IRCC-PR) databases. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/2/E227/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.