


Abstract
Background: Early identification of people with diabetes or prediabetes enables greater opportunities for glycemic control and management strategies to prevent related complications. To identify gaps in screening for these conditions, we examined population trends in receipt of timely glucose testing overall and in specific clinical subgroups.
Methods: Using linked administrative databases, we conducted a retrospective cohort study of people aged 40 years and older without diabetes at baseline. Our primary outcome was up-to-date glucose testing, defined as having received testing at least once in the 3 years before each index year from 2010 to 2017, using linked administrative databases of people residing in Ontario, Canada. We calculated rates of up-to-date testing by age group, sex, ethnicity (South Asian, Chinese, general population) and comorbidities (hypertension, hyperlipidemia, cardiovascular disease).
Results: Over the 8-year study period, up-to-date glucose testing rates were stable at 67% for men and 77% for women (both relative risk 1.00 per year; 95% confidence interval 1.00–1.00). Testing rates were significantly lower in men than in women (all age groups p < 0.001) and lower in younger than older age groups (except those aged ≥ 80 yr). South Asian people had the highest testing rates, although among people aged 70 years or older, testing was highest in the general population (p < 0.001). Among people with hypertension, hyperlipidemia and cardiovascular disease, annual testing rates were also stable, but only 58% overall among people with hypertension.
Interpretation: We found lower glucose testing rates in younger men and people with hypertension. Our findings reinforce the need for initiatives to increase awareness of glycemic testing.
Diabetes mellitus is a major cause of morbidity and mortality, accounting for 1.5 million deaths worldwide in 2012 and attributable to 11.9% of deaths in Canada in 2009.1–3 The prevalence of diabetes has also been steadily increasing, with an estimated 3.4 million Canadians or 9.3% of the population affected in 2015.4–6 By 2025, the prevalence is predicted to rise 44% to 5 million Canadians, or 12.1% of the population.5 With considerable advances in glycemic control measures and management strategies — such as early lifestyle modifications and novel pharmacologic interventions — which have the potential to reduce morbidity and mortality, screening for diabetes is cost-effective.7–10 However, despite advocacy for early diagnosis and intervention, 11 diabetes often goes unnoticed and appropriate interventions are delayed as a substantial proportion of individuals who ultimately receive diagnoses may be asymptomatic in the initial phases for many years.12,13
In Canada, the prevalence of undiagnosed diabetes is estimated to be 1.1%–3.1%.14 Diabetes Canada and the Canadian Cardiovascular Harmonized National Guidelines Endeavour (C-CHANGE) guidelines thus recommend that all adults aged 40 years and older be screened every 3 years, and those at very high risk regardless of age (e.g., with cardiovascular disease or cardiac risk factors, and some ethnic groups) be screened every 6 to 12 months to ensure early diagnosis and initiation of appropriate interventions to reduce morbidity and mortality.15,16
Several studies have described trends in prediabetes and diabetes incidence and prevalence in the general adult population, but few have assessed screening practices in the context of clinical practice guidelines.4,17–21 To identify potential gaps in testing by age, sex or ethnicity, our objective was to examine temporal trends in the proportion of adults in Ontario, Canada, who were 40 years and older without a diabetes diagnosis and who received blood glucose testing (including glycosylated hemoglobin [HbA1c]) in the previous 3 years, making them up to date with screening recommendations.15,16 We also examined trends among adults with hypertension, hyperlipidemia and cardiovascular disease.
Methods
Study design and population
We conducted a retrospective, population-based cohort study of the entire population of Ontario eligible for the province’s publicly available health insurance plan (Ontario Health Insurance Plan [OHIP]) using multiple population-based health administrative databases. We identified residents without known diabetes between 2008 and 2017 from the Ontario Registered Persons Database (RPDB), which contains demographic information about eligibility for OHIP, including birth date, sex and residential postal code.
We examined glucose testing rates among both the overall population of adults and a subcohort of individuals with hypertension, hyperlipidemia and a history of cardiovascular disease.15,16 For the overall population, we created annual study cohorts from 2010 to 2017 of individuals eligible for OHIP and aged at least 40 years for the entire 3 years before. Thus, individuals entered the cohort at a minimum age of 40 years, but evaluation of up-to-date glucose testing began at age 43 years.
Using the Diabetes Canada and C-CHANGE guidelines, we defined up-to-date testing as having received blood glucose or HbA1c testing at least once during those 3 years.15,16 For the subcohorts of individuals with hypertension, hyperlipidemia and cardiovascular disease, for whom screening is recommended every 6 to 12 months, we examined annual testing between 2008 and 2017.15,16
Data sources
We identified individuals with a diabetes diagnosis through linkage to the Ontario Diabetes Database (ODD), which is a database of all Ontario residents with physician-diagnosed diabetes, created using the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD) of all acute care hospital admissions and the OHIP Claims database. 22 The OHIP database contains information from physician claims and diagnostic and community laboratory services in Ontario.23,24 The negative predictive value of the ODD has been validated at 97.6%.22
Similarly, we identified individuals with hypertension from the Ontario Hypertension Database, a validated database of Ontario residents with physician-diagnosed hypertension.25 We identified individuals with hyperlipidemia from the OHIP database, using an algorithm of at least 2 physician claims with a diagnosis of hyperlipidemia within 2 years before the study year, and determined history of cardiovascular disease from the CIHI-DAD; codes for cardiovascular diseases are shown in Appendix 1 (available at www.cmajopen.ca/content/10/3/E772/suppl/DC1).26
For ethnicity, we used a validated surname algorithm to classify individuals into 3 groups, based on likely ethnicity: Chinese, South Asian and all others in the general population. 27 We determined rural or urban residence and neighbourhood income quintile through linkage of each individual’s postal code to Statistics Canada Census data.28 We used the Client Agency Program Enrolment (CAPE) database, maintained by the Ontario Ministry of Health to track patient enrolment with primary care providers, to identify individuals rostered to a primary care physician in a group practice.29 We classified as virtually rostered those individuals who were not formally rostered to a physician in CAPE but received most of their primary care services from a particular physician.
Outcomes
To identify people receiving glucose testing, we used the OHIP database, which provides health services data on all residents of the province, and the Ontario Laboratories Information System, and included HbA1c, serum or plasma glucose, and oral glucose tolerance testing. The Ontario Laboratories Information System is a province-wide, centralized repository of laboratory results from tests conducted in Ontario, which began in 2007.30 Because OHIP claims do not differentiate between fasting and nonfasting blood glucose tests, we were unable to restrict to fasting tests as recommended in Canadian guidelines, although diagnoses can be made using random tests in situations of overt hyperglycemia.15 Details of codes used to identify glucose testing are shown in Appendix 1.
We excluded tests performed while a person was in hospital because our focus was on testing in the primary care setting, and restricted OHIP claims to tests ordered by family physicians. We also excluded tests performed on pregnant women, as they undergo glycemic testing for specific pregnancy-related indications. All data sets were linked using unique, encoded identifiers and analyzed at ICES (formerly Institute for Clinical Evaluative Sciences).
Statistical analysis
We calculated absolute rates of up-to-date testing for 2010 to 2017 overall and for test type by sex, 10-year age bands up to age 80 years or older, and ethnicity. We compared characteristics of individuals up to date with testing versus not for the latest (2017) cohort using means and standard deviations for age and number of physician visits, and proportions for categorical variables. To examine factors associated with being up to date with testing, we additionally performed logistic regression, adjusting for age, sex, rural residence, neighbourhood income quintile, ethnicity, hypertension, hyperlipidemia and cardiovascular disease, which have been identified in previous studies of health services access and outcomes.31,32
In post-hoc analyses, we calculated up-to-date testing rates in those who were and in those who were not rostered formally or virtually to a primary care physician as a proxy for access to a physician. Post hoc, we stratified analyses by rostering to primary care physician. We also examined annual testing rates for individuals with hypertension, hyperlipidemia and cardiovascular disease by sex and age group. We compared testing rates between groups using Poisson regression, modelling the number of individuals tested as a linear function of year and population, and the natural logarithm of the number of eligible individuals as the offset. We also ran separate models for each predefined subgroup to examine temporal trends. Because an individual’s test in 1 year contributes to the outcome for the following 2 years (i.e., were nonindependent), we performed bootstrapping with 1000 samples to estimate 95% confidence intervals (CIs) and p values. We conducted all analyses using SAS version 9.4 (SAS Institute) and considered 2-sided p values < 0.05 to be significant.
Ethics approval
The use of the data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a research ethics board.
Results
We identified about 5.5 million individuals in each 3-year study cohort. Mean age was approximately 57 years and 47% were men. Chinese people comprised about 6% and South Asian people about 3% of each cohort.
Testing by age and sex
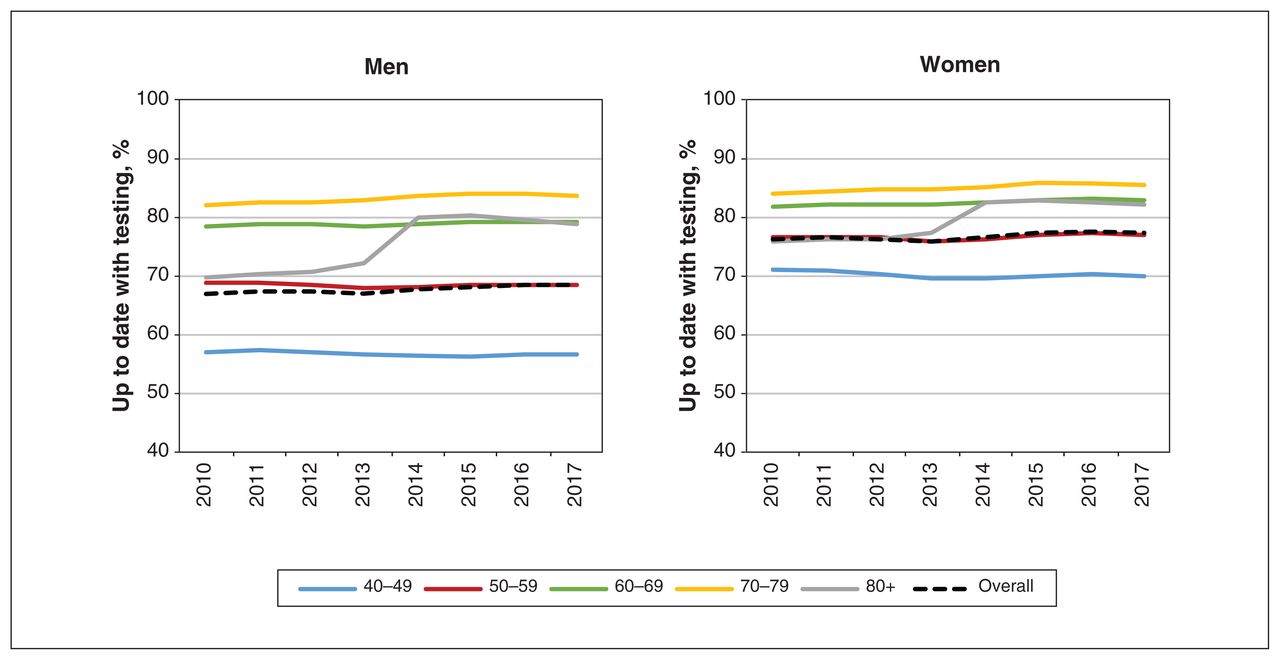
Figure 1 and Appendix 2 (available at www.cmajopen.ca/content/10/3/E772/suppl/DC1) show rates of up-to-date glucose testing by age group and sex overall and by test type, respectively. Over time, we observed overall glucose testing rates to be stable at 67% among men and 77% among women (both relative risk [RR] 1.00 per year; 95% CI 1.00–1.00), although we also observed increases in HbA1c testing concomitant with decreases in serum or plasma glucose testing.

Up-to-date glucose testing rates among adults aged 40 years or older in Ontario, by age (years), 2010–2017. “Up to date” is defined as at least 1 glycosylated hemoglobin, plasma or serum glucose or oral glucose tolerance test in the previous 3 years, and excludes people who received a diabetes diagnosis before the study period.
Across all age groups, rates were higher among women than men (all p < 0.001). We observed the greatest absolute differences between men and women in the 40–49-year age group, where 57% of men were up to date with testing, compared with 70% of women. For individuals younger than 80 years, rates of up-to-date glucose testing increased with age for both men and women (combined 63% among the 40–49-year age group v. 84% among the 70–79-year age group). Among individuals aged 80 years and older, rates up to 2013 were stable at about 70% among men and 76% among women. Thereafter, rates rose sharply to relatively new stable rates of 80% and 82%, respectively, and was attributable to increases in both HbA1c and glucose testing (Appendix 2).
Testing by ethnicity
Age- and sex-stratified results by ethnicity showed similar trends to age- and sex- stratified results in the overall population (Figure 2). A greater proportion of women were up to date with testing than men (all ethnic groups, p < 0.001), as were older age groups compared with younger age groups, except for Chinese and South Asian people aged 70 years or older. Overall, South Asian people had the highest glucose testing rates (about 77%; RR 1.06, 95% CI 1.06–1.06, general population as reference), followed by the general (72%) and Chinese populations (about 69%; RR 0.96, 95% CI 0.95–0.96, general population as reference). However, among adults aged 70 years and older, testing was markedly higher in the general population than among the South Asian and Chinese groups (p < 0.001 for both), but among men younger than 60 years, South Asian people had higher up-to-date testing rates than their Chinese and general population counterparts (p < 0.05 for both).

Up-to-date glucose testing rates among (A) men and (B) women aged 40 years and older in Ontario, by ethnicity, 2010–2017. “Up to date” is defined as at least 1 glycosylated hemoglobin, plasma or serum glucose or oral glucose tolerance test in the previous 3 years, and excludes people who received a diabetes diagnosis before the study period. Groups are displayed in order of increasing overall rates of testing in 2017.
Up-to-date testing
Characteristics of those up to date with testing in 2017 are shown in Table 1 and Appendix 3 (available at www.cmajopen.ca/content/10/3/E772/suppl/DC1). Older age, being female, living in a high-income neighbourhood, having a regular primary care physician and visiting a physician more often were all associated with a greater likelihood of being up to date with testing (p < 0.001). Individuals with hypertension or a history of cardiovascular disease were also more likely to have been tested in the previous 3 years than those without (> 85%).
Characteristics of being up to date or not up to date with glucose testing among people aged 40 years and older in Ontario, 2017
Additional analyses
We conducted post-hoc analyses to characterize our findings further. First, when we examined people rostered to a primary care physician separately from those who were not, those who were rostered were more likely to be up to date with testing (about 77% v. about 21%; Appendix 4, available at www.cmajopen.ca/content/10/3/E772/suppl/DC1). However, we observed mild increases among nonrostered, older age groups (particularly people aged 80 years and older) between 2012 and 2017.
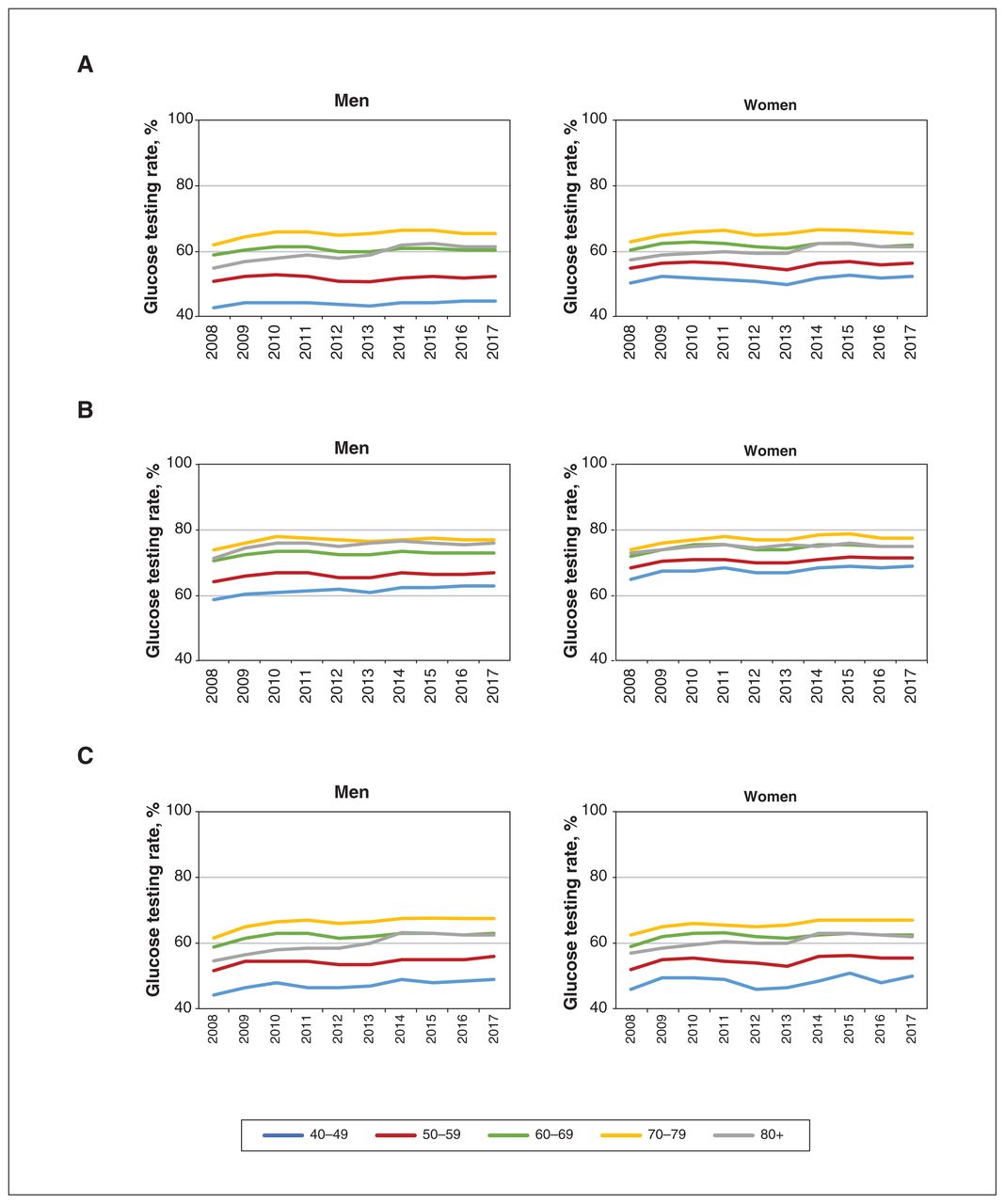
In analyses of important clinical subgroups, annual testing rates among individuals with hypertension, hyperlipidemia and cardiovascular disease were stable during the study period (Figure 3; about 58%, 70% and 60%, respectively). Testing rates were higher among older than younger adults, and among women than men, especially among younger age groups. Among those with hypertension, about 65% of men and women aged 70–79 years were tested annually compared with 44% and 51% of men and women aged 40–49 years, respectively. Among men and women aged 70–79 years with cardiovascular disease, about 66% were tested annually compared with less than 50% of men and women aged 40–49 years; and among those with hyperlipidemia, annual testing rates were almost 80% among adults aged 70 years and older compared with 61% and 67% of men and women aged 40–49 years, respectively.

Annual glucose testing rates among high-risk populations in Ontario 2008–2017: (A) people with hypertension, (B) people with hyperlipidemia and (C) people with cardiovascular disease. “Glucose testing” is defined as at least 1 glycosylated hemoglobin, plasma or serum glucose or oral glucose tolerance test and excludes people who received a diabetes diagnosis before the study year or were admitted to hospital during the study year. “Cardiovascular disease” is defined as a history of hospital admission for myocardial infraction, stroke or heart failure, or previous percutaneous coronary intervention or coronary artery bypass graft surgery.
Interpretation
In this study of contemporary trends in rates of up-to-date glucose testing over the last decade, we found that the proportion of people up to date as recommended by Canadian practice guidelines15,16 has been stable among both men and women, across different age and ethnic groups, and among subpopulations of individuals with hypertension and hyperlipidemia. We identified important gaps in recommended testing among young men and older Chinese and South Asian people. Annual testing rates were also suboptimal among individuals with hypertension, hyperlipidemia and cardiovascular disease.
Notable among those aged 80 years and older was the increase in up-to-date testing rates between 2013 and 2014, possibly attributable to Diabetes Canada’s 2013 release of a new guideline encouraging use of HbA1c testing.33 Although screening in this population is of questionable benefit and recommended on an individual basis, without the need for prior fasting, testing became more convenient for this population, which may not tolerate fasting.34 In addition, in this older population, much focus may be on the management of existing chronic conditions and comorbidities. As such, primary preventive care such as diabetes screening may have been overlooked until the guideline’s release brought greater attention to the importance of glycemic testing, particularly among people without a regular primary care physician.
Our results are consistent with earlier studies of glucose testing and diabetes screening.35,36 Lee and colleagues’ cross-sectional study of electronic medical records found that fewer than 50% of rostered patients received screening over a 36-month period, and Wilson and colleagues reported that 63% of Ontarians aged 40 years and older without diabetes received blood glucose testing between 2003 and 2005.35–37 Findings of increasing uptake of HbA1c testing between 1995 and 2015 may contribute to our higher overall testing rates.36,38
Regarding ethnicity, higher testing rates have been reported among immigrants in Ontario than among the general population, with South Asian immigrants having the highest rates.35 Similar to our findings, older immigrants were also less likely to be tested than their general population counterparts. Whether this is a result of generation gaps in health-seeking behaviour, language barriers, health literacy or other reasons is unknown.39 In the United States, results from studies of ethnic groups have been mixed, with some reporting lower testing rates among several visible-minority groups compared with non-Hispanic white people,40,41 and another study finding no significant association between “high-risk” ethnicity and diabetes screening.42 Although differences between Canada and the US may be attributable to greater access through Canada’s publicly available health care system, further understanding of contributing factors to lower testing among older immigrants is required.
Studies have indicated that diabetes prevalence is on the rise globally, partly owing to increased survival.4–6 However, a recent systematic review suggests that diabetes incidence, which increased in many populations up to the mid-2000s, has since stabilized or declined in many regions.43,44 In Ontario, diabetes incidence increased 31% between 1997 and 2003,18 yet data from the Canadian Chronic Disease Surveillance System show a decrease in incidence between 2006/07 and 2013/14.45 Whether stabilization in glucose testing rates, as observed in this study, or preventive strategies and health initiatives have contributed to this decline requires further investigation. Regardless, our results suggest that further progress in implementing clinical practice guidelines could still be made.
Diabetes incidence has increased substantially among Chinese Canadian people, and a recent study found that immigrants in Ontario, especially South Asian and Southeast Asian people, convert from prediabetes to diabetes at earlier ages than people born in Canada.46,47 Combined with reports of undiagnosed diabetes contributing about 20% to overall type 2 diabetes prevalence rates, continued vigilance in diabetes screening is needed.14 In this study, we identified younger men (especially in the Chinese and general population groups), older Chinese and South Asian people, residents of low-income neighbourhoods, and those without a regular primary care physician or with hypertension or cardiovascular disease as potential targets to improve earlier diagnosis of diabetes.
Regular screening of vulnerable or at-risk populations is important for providing opportunities for early diagnosis and initiation of interventions, especially when the trajectory of the development of diabetes can be rapid, as has been observed in different ethnic groups.47 Earlier diagnosis, particularly among those with additional risk factors, such as hypertension and hyperlipidemia, could lead to earlier glucose control, thus delaying the onset of diabetic complications, including cardiovascular disease. However, improving screening for diabetes requires at-risk individuals to seek testing, physicians to order testing, and public health agencies and policy-makers to increase awareness of the need for testing.
Limitations
A strength of this study is the availability of multiple sources of routinely collected data, enabling us to examine trends in glucose testing among almost the entire adult population of Ontario. Nonetheless, our inability to delineate the reasons for testing is a limitation, as we recognize that some testing may be performed for reasons other than preventive care. Consequently, we used the term “glucose testing” rather than “diabetes screening” because we are unable to determine from our data sources whether a particular laboratory test was conducted for diabetes screening or another purpose, even though we considered only tests ordered for patients who were not in hospital and not pregnant.
Our analyses by ethnicity were also limited in that we could identify people who were only likely to be Chinese and South Asian, and although they are the 2 most populous ethnic groups (> 50% of all visible minorities) in Ontario, an investigation of other ethnic or racial groups was not possible. 48 In our multivariable analyses to identify characteristics associated with up-to-date testing, we were unable to account for some factors that may be associated with testing, such as education, obesity and physical activity. Finally, we examined primary care rostering post hoc and did not include it a priori in our analysis of predictors of up-to-date testing. However, we did include visit frequency and access to primary care physicians in these analyses.
Conclusion
Rates of up-to-date glucose testing as recommended by Diabetes Canada guidelines remained relatively stable between 2010 and 2017, at about 70%. However, lower rates among some age, sex and ethnic groups and among people with hypertension or hyperlipidemia are concerning, given the morbidity and mortality associated with diabetes if left undiagnosed and untreated. Although much effort has been made in addressing rising diabetes prevalence and incidence, only with appropriate diabetes screening can indicated diabetes management strategies be implemented for those who receive a diagnosis or who are determined to be at risk. Improving screening rates will require initiatives to ensure that health practices and policies to encourage testing reach underscreened populations such that they are enabled to receive testing.
Footnotes
Competing interests: Catherine Yu reports receiving research grants from the St. Michael’s Hospital Medical Services Association, St. Michael’s Hospital (Unity Health Toronto), the Ontario SPOR SUPPORT Unit and the Royal College of Physicians and Surgeons of Canada. Kim Connelly reports receiving research grants and payment for presentations from AstraZeneca, Servier, Boehringer Ingelheim, Eli Lilly, Novartis, Novo Nordisk and Merck. Dr. Connelly also reports serving on a Data Safety Monitoring Board or Advisory Board for AstraZeneca, Servier, Boehringer Ingelheim, Eli Lilly, Novartis, Novo Nordisk and Merck. Gillian Booth reports receiving grants or contracts from the Canadian Institutes of Health Research (CIHR), Juvenile Diabetes Research Foundation and the Thistledown Foundation. Karen Tu reports receiving payments (to institutions) from CIHR, St. Michael’s Hospital Foundation, The College of Family Physicians of Canada, Foundation for Advancing Family Medicine, Canadian Medical Association Foundation, North York General Hospital, Heart and Stroke Foundation of Canada, Heart and Stroke Foundation of Ontario, Department of Defense (United States), University of Toronto (Department of Family and Community Medicine), MaRS Innovation Fund, Canadian Dermatology Foundation, Canadian Rheumatology Association (Canadian Initiative for Outcomes in Rheumatology Care), PSI Foundation, Cancer Care Ontario, Toronto Rehabilitation Institute Chair Fund, University of Toronto Practice-Based Research Network, Arthritis Society, MS Society of Canada, The Canadian Vascular Network and the Ontario SPOR SUPPORT Unit Targeted IMPACT Award. Sheldon Tobe reports receiving a KMH clinic unrestricted grant and in-kind support for the Zero to Five study, and consulting fees from AstraZeneca (all paid to Sunnybrook Research Institute). Dr. Tobe also reports receiving payment from Amgen, Astra-Zeneca, Bristol Myers Squibb, Bayer, Boehringer Ingelheim, Janssen, Lilly, Novartis, Novo Nordisk, Pfizer and Sanofi Genzyme for the CHEPPLUS education program. Dr. Tobe has worked on a volunteer basis with the American Hypertension Specialists Certification Program. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work and the interpretation of data. Anna Chu, Baiju Shah, Mohammed Rashid and Douglas Lee acquired and analyzed the data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by a grant from the Canadian Vascular Network (CVN), which is funded by annual grants from the Ontario Ministry of Health (MOH) and Ministry of Long-Term Care (MLTC); and a Foundation grant (# FDN 148446) from the Canadian Institutes of Health Research (CIHR). Louise Sun is supported by the Ottawa Heart Institute Research Corporation and a Clinical Research Chair in Big Data and Cardiovascular Outcomes at the University of Ottawa. Douglas Lee is the Ted Rogers Chair in Heart Function Outcomes, University Health Network, University of Toronto and is supported by a Mid-Career Award from the Heart and Stroke Foundation. Karen Tu receives a Research Scholar Award from the Department of Family and Community Medicine, University of Toronto. Gillian Booth is the Canada Research Chair in Policy Solutions for Diabetes Prevention and Management. Husam Abdel-Qadir is supported by a National New Investigator Award from the Heart and Stroke Foundation of Canada. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by the funders is intended or should be inferred.
Data sharing: The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E772/suppl/DC1.
Disclaimer: Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI) and Ontario Health. The analyses, results, views, conclusions, opinions and statements expressed in the manuscript are those of the authors, and do not necessarily reflect those of the above agencies. No endorsement by CIHI or Ontario Health is intended or should be inferred. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding or data sources. No endorsement by ICES or the Ontario MOH and MLTC is intended or should be inferred.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.