


Article Figures & Tables
Figures
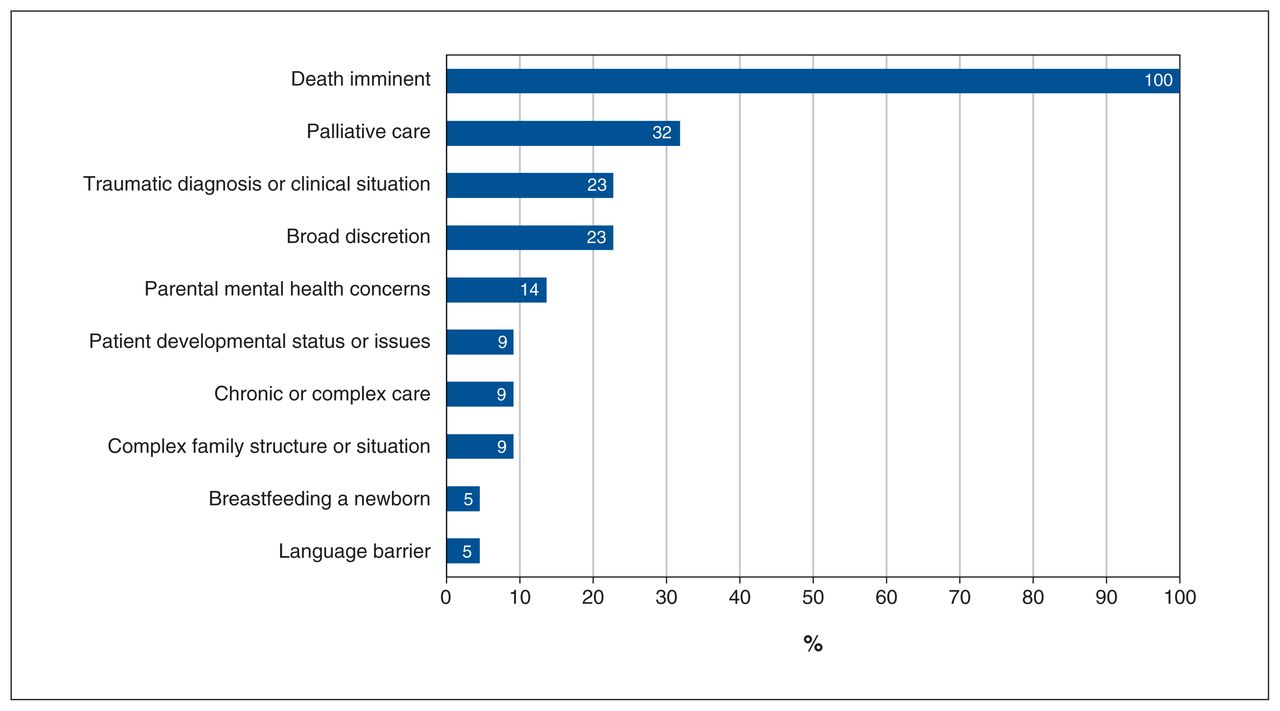
- Figure 1:
Stated reasons for granting exceptions to restrictions, where an exception was an increase in the number of family members present at a single time, or increased frequency of switches (n = 24 respondents).

Tables
Characteristic No. (%) Hospital type Stand-alone children’s hospital 5 (26) Children’s health unit in a larger, mixed hospital 11 (58) Women and children’s hospital 3 (16) PICU type Medical–surgical 11 (58) Level 2 medical–surgical† 2 (11) Cardiac 2 (11) Mixed medical–surgical–cardiac 6 (32) No. of beds < 10 5 (26) 10–19 10 (53) ≥ 20 4 (21) Ages admitted, yr Birth to 16 2 (11) Birth to 17 3 (16) Birth to 18 14 (74) - Table 2:
Family presence policies early in the COVID-19 pandemic (March–May 2020) for all Canadian PICUs — results of literature search*
Hospital, city, province Policy information source Document type(s) No. of people at bedside Switching practice to enable second parent or support† Approach to minor-age siblings Approach to other non-parent family and visitors‡ Response to family or visitors with infectious symptoms or risk§ In-hospital mobility¶ Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Janeway Children’s Health and Rehabilitation Centre, St. John’s, Newfoundland and Labrador Health authority Website, social media NS NS NS Not allowed or only at end of life Not allowed NS NS IWK Health, Halifax, Nova Scotia Hospital Website 1 NS NS Not allowed or only at end of life NS Screened NS CHU de Québec–Université Laval, Québec City, Quebec Hospital Website 1 NS NS Not allowed or only at end of life Not allowed NS NS CIUSSS de l’Estrie–CHU Sherbrooke, Sherbrooke, Quebec Health authority Website NS NS NS NS NS Not allowed NS Montreal Children’s Hospital; Montréal, Quebec Hospital Website 2 (strict) NS Unnecessary Not allowed or only at end of life Not allowed NS NS CHU Sainte-Justine, Montréal, Quebec Hospital Website 2 (strict) NS Unnecessary Not allowed or only at end of life Not allowed Not allowed NS Kingston Health Sciences Centre, Kingston, Ontario Hospital Original policy, website NS NS NS Not allowed or only at end of life Not allowed Screened NS Children’s Hospital of Eastern Ontario, Ottawa, Ontario Hospital Website 2 (strict) NS Restricted times or frequencies Not allowed or only at end of life Not allowed Screened NS The Hospital for Sick Children, cardiac, Toronto, Ontario Hospital Website 1 NS NS Not allowed or only at end of life Not allowed Screened NS The Hospital for Sick Children, medical–surgical, Toronto, Ontario Hospital Website 1 NS NS Not allowed or only at end of life Not allowed Screened NS McMaster Children’s Hospital, Hamilton, Ontario Hospital Website NS 1 NS NS NS NS NS Children’s Hospital–London Health Sciences Centre, London, Ontario Hospital News release 1 NS NS Not allowed or only at end of life Not allowed Not allowed NS Children’s Hospital–Health Sciences Centre, Winnipeg, Manitoba Hospital Website 1 NS NS At manager’s discretion NS NS NS Jim Pattison Children’s Hospital, Saskatoon, Saskatchewan Health authority Original policy, website, news release, poster 1 1 Not allowed Not allowed or only at end of life Not allowed Not allowed Not allowed to leave PICU room Stollery Children’s Hospital, cardiac, Edmonton, Alberta Health authority Original policy, website NS NS NS Not allowed or only at end of life NS Not allowed NS Stollery Children’s Hospital, medical–surgical, Edmonton, Alberta Health authority Original policy, website NS NS NS Not allowed or only at end of life NS Not allowed NS Alberta Children’s Hospital, Calgary, Alberta Health authority Original policy, website NS NS NS Not allowed or only at end of life NS Not allowed NS BC Children’s Hospital, Vancouver, British Columbia Hospital Website 2 (strict) NS Unnecessary Not allowed or only at end of life NS Screened NS Victoria General Hospital, Victoria, British Columbia Health authority Website 1 1 Restricted times or frequencies Not allowed or only at end of life NS Not allowed NS No. not specified (%) – – 7 (37) 16 (84) 13 (68) 2 (11) 9 (47) 5 (26) 18 (95) Note: NS = not specified, PICU = pediatric intensive care unit.
For full data, see Appendix 4, available at www.cmajopen.ca/content/10/3/E622/suppl/DC1.
↵* Abstracted and abbreviated from publicly accessible documents.
† Refers to a PICU or hospital practice in which the number at the bedside is limited to enable 1 caregiver to leave and be replaced by a different caregiver. In this table, switches were designated as “unnecessary” if both parents or 2 caregivers could be present at the same time.
↵† Including siblings over age 18 years.
↵§ Including respiratory infectious symptoms or suspected SARS-CoV-2. ”Screened” indicates that family members were screened for infection, without indication of the action taken if a visitor screened positive.
↵¶ Refers to whether caregivers were allowed to leave the PICU room and move around the hospital for any reason, including accessing basic needs.
Family presence policy No. (%) of respondents Before the pandemic March 2020 August–December 2020 Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Shared policies between PICU and all pediatric care areas Yes 11 (46) 20 (83) No 7 (29) 3 (13) Unsure 6 (25) 1 (4) Agreement, no. of pairs (% agreement)† 2 (50) 5 (100) No. of support people at bedside 1 0 (0) 21 (88) 23 (96) 5 (21) 12 (50) 2 (strict) 8 (33) 3 (13) 1 (4) 19 (79) 12 (50) 2 (flexible) 11 (46) 0 (0) 0 (0) 0 (0) 0 (0) Unlimited 5 (21) 0 (0) 0 (0) 0 (0) 0 (0) Agreement, no. of pairs (% agreement)‡ 5 (0) 5 (80) 5 (100) 5 (100) 5 (60) Switches to enable other parent’s presence§ Unnecessary (multiple visitors permitted) 24 (100) 3 (13) 1 (4) 19 (79) 12 (50) Not allowed 0 (0) 7 (30) 13 (57) 0 (0) 3 (13) Any time 0 (0) 4 (17) 2 (9) 1 (4) 2 (8) Restricted times or frequencies 0 (0) 9 (39) 7 (30) 4 (17) 7 (29) Agreement, no. of pairs (% agreement)‡ 5 (100) 4 (50) 4 (75) 5 (100) 5 (40) Timing of parental presence 24/7 13 (54) 19 (79) 22 (92) 20 (83) 23 (96) Parents always allowed, but only 1 may stay if sleeping 6 (25) 2 (8) 1 (4) 2 (8) 1 (4) Parents must leave overnight 2 (8) 1 (4) 1 (4) 0 (0) 0 (0) Parents must leave during rounds or handover 3 (13) 2 (8) 0 (0) 2 (8) 0 (0) Agreement, no. of pairs (% agreement)‡ 5 (80) 4 (80) 5 (100) 5 (80) 5 (100) Nonparent family members and visitors may switch into bedside¶ Unnecessary (family and visitors unlimited) 6 (25) 0 (0) 0 (0) 0 (0) 0 (0) Not allowed 0 (0) 23 (96) 23 (96) 15 (65) 19 (83) Any time 12 (50) 0 (0) 0 (0) 3 (13) 0 (0) Restricted times or frequencies 6 (25) 1 (4) 1 (4) 5 (22) 4 (17) Agreement, no. of pairs (% agreement)‡ 5 (60) 5 (100) 5 (100) 4 (50) 4 (50) Sibling presence Unrestricted 12 (50) 0 (0) 0 (0) 1 (4) 0 (0) Not allowed, or only at end of life 1 (4) 24 (100) 24 (100) 17 (71) 23 (96) With restrictions (e.g., time, duration, age) 9 (38) 0 (0) 0 (0) 6 (25) 1 (4) At RN discretion 2 (8) 0 (0) 0 (0) 0 (0) 0 (0) Agreement, no. of pairs (% agreement)‡ 5 (80) 5 (100) 5 (100) 5 (100) 5 (100) Note: PICU = pediatric intensive care unit, RN = registered nurse.
↵* Unless otherwise indicated.
↵† Physician chief and operations manager pairs from the same unit who did not indicate “unsure.”
↵‡ Physician chief and operations manager pairs from the same unit for which both provided an answer to the given variable.
↵§ Early pandemic: n = 23.
↵¶ Mid-pandemic: n = 23.
Family presence practice No. (%) of respondents Before the pandemic March 2020 August–December 2020 Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Rounds practices† In-person 24 (100) 13 (59) 5 (23) 21 (95) 7 (33) Virtual or telephone 0 (0) 5 (23) 8 (36) 1 (5) 7 (33) Nonparticipation 0 (0) 4 (18) 9 (41) 0 (0) 7 (33) Agreement, no. of pairs (% agreement)‡ 5 (100) 3 (66) 3 (33) 4 (100) 3 (66) Rounds location§ Adjacent to room (e.g., bedside) 24 (100) 17 (74) 16 (70) 22 (100) 21 (100) Distant location (e.g., conference room) 0 (0) 6 (26) 7 (30) 0 (0) 0 (0) Agreement, no. of pairs (% agreement)‡ 5 (100) 4 (100) 4 (75) 4 (75) 3(100) Ability to leave PICU room¶ Unrestricted 24 (100) 17 (71) 0 (0) – – Not allowed to leave 0 (0) 0 (0) 7 (29) – – Restricted: toilet 0 (0) 1 (4) 11 (46) – – Restricted: stress/procedures 0 (0) 0 (0) 4 (17) – – Restricted: eating 0 (0) 0 (0) 2 (8) – – Encouraged not to leave room, not mandated 0 (0) 6 (25) 3 (13) – – Agreement, no. of pairs (% agreement)‡ 5 (100) 5 (100) 5 (80) – – Ability to leave hospital¶ Unrestricted 24 (100) 21 (88) 3 (13) – – Restricted frequency (e.g., once per shift, once per day) 0 (0) 0 (0) 4 (17) – – Restricted: smoking 0 (0) 1 (4) 5 (21) – – Restricted: switches 0 (0) 2 (8) 7 (29) – – Never 0 (0) 1 (4) 8 (33) – – Agreement, no. of pairs (% agreement)‡ 5 (100) 5 (80) 5 (60) – – Note: PICU = pediatric intensive care unit.
↵* Unless otherwise indicated.
↵† Early pandemic: n = 22; mid-pandemic: n = 22 respondents for patients who tested negative for SARS-CoV-2, n = 21 for patients with confirmed or suspected SARS-CoV-2 infection.
↵‡ Physician chief and operations manager pairs from the same unit for which both provided an answer to the given variable.
↵§ Early pandemic: n = 23; mid-pandemic: n = 22 for patients who tested negative for SARS-CoV-2; n = 21 for patients with confirmed or suspected SARS-CoV-2 infection.
↵¶ Respondents could indicate more than 1 reason for leaving (e.g., toilet, eating, switches and smoking).
- Table 5:
Approach to policy exceptions and decision-making authority — survey responses (n = 24)
Factor No. (%) of respondents Approach to policy exceptions* Exceptions enabled by policy 10 (42) Processes understood but not formalized 4 (17) No initial policy or process, but developed over study period 7 (29) No policy 3 (13) Agreement, no. of pairs (% agreement)† 5 (100) Decision-making authority PICU (physician, manager or charge nurse) 9 (38) Hospital director 8 (33) Infection prevention and control or emergency operations 6 (25) Hospital executive 1 (4) Agreement, no. of pairs (% agreement)† 5 (40) Note: PICU = pediatric intensive care unit.
↵* Exceptions referred to enabling deviation from policy in certain circumstances. Examples of exceptions were: allowing more people at the bedside; allowing siblings; allowing more frequent switches of parents or other family members.
↵† Physician chief and operations manager pairs from the same unit for which both provided an answer to the given variable.
- Table 6:
PICU in-room masking requirements and screening for parents and support people — survey responses (n = 24)
Factor No. (%) of respondents March 2020 August–December 2020 Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Patients without SARS-CoV-2 infection Patients with confirmed or suspected SARS-CoV-2 infection Masking in patient room Always 4 (17) 11 (46) 10 (42) 15 (62) Never 17 (71) 11 (46) 8 (33) 3 (12) When a health care provider is present 2 (8) 2 (8) 6 (25) 6 (25) If child is infectious 1 (4) NA 0 (0) NA Agreement, no. of pairs (% agreement)* 5 (80) 5 (100) 5 (80) 5 (80) SARS-CoV-2 screening for parents and support people† Preadmission questionnaire 20 (83) – – – Hospital or PICU entry screening questionnaire 20 (83) – – – Daily PICU symptom screening 8 (33) – – – Temperature check 3 (13) – – – Admission swab 1 (4) – – – Agreement, no. of pairs (% agreement)* 5 (60) – – –
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.