


Abstract
Background: In Canada, all provinces implemented vaccine passports in 2021 to reduce SARS-CoV-2 transmission in non-essential indoor spaces and increase vaccine uptake (policies active September 2021–March 2022 in Quebec and Ontario). We sought to evaluate the impact of vaccine passport policies on first-dose SARS-CoV-2 vaccination coverage by age, and area-level income and proportion of racialized residents.
Methods: We performed interrupted time series analyses using data from Quebec’s and Ontario’s vaccine registries linked to census information (population of 20.5 million people aged ≥ 12 yr; unit of analysis: dissemination area). We fit negative binomial regressions to first-dose vaccinations, using natural splines adjusting for baseline vaccination coverage (start: July 2021; end: October 2021 for Quebec, November 2021 for Ontario). We obtained counterfactual vaccination rates and coverage, and estimated the absolute and relative impacts of vaccine passports.
Results: In both provinces, first-dose vaccination coverage before the announcement of vaccine passports was 82% (age ≥ 12 yr). The announcement resulted in estimated increases in coverage of 0.9 percentage points (95% confidence interval [CI] 0.4–1.2) in Quebec and 0.7 percentage points (95% CI 0.5–0.8) in Ontario. This corresponds to 23% (95% CI 10%–36%) and 19% (95% CI 15%–22%) more vaccinations over 11 weeks. The impact was larger among people aged 12–39 years. Despite lower coverage in lower-income and more-racialized areas, there was little variability in the absolute impact by area-level income or proportion racialized in either province.
Interpretation: In the context of high vaccine coverage across 2 provinces, the announcement of vaccine passports had a small impact on first-dose coverage, with little impact on reducing economic and racial inequities in vaccine coverage. Findings suggest that other policies are needed to improve vaccination coverage among lower-income and racialized neighbourhoods and communities.
The COVID-19 pandemic led to unprecedented interventions, including both generalized and targeted restrictions. Once vaccines became widely available in 2021 in high-income countries, many governments implemented proof-of-vaccination policies to further mitigate the pandemic’s impacts on population health and the economy.1 Often termed “vaccine passports,” these policies required demonstration of vaccination status or a valid exemption to access non-essential activities and spaces, including restaurants, bars, movie theatres, concerts and extracurricular activities.
All Canadian provinces and the Yukon territory introduced vaccine passports in 2021 and discontinued them by April 2022. Quebec and Ontario — the 2 most populous provinces and Canadian epicentres of the pandemic2–4 — were among the first to announce vaccine passports, implementing them in September 2021 and discontinuing them in March 2022. Provincial governments stated that these policies aimed to reduce SARS-CoV-2 transmission and prevent re-closure of non-essential venues primarily by limiting contacts of individuals who had not yet been vaccinated in non-essential venues and by increasing vaccination coverage.5–7
The ethical and practical implications of vaccine passports have been debated,1,8–11 yet evidence on their effectiveness at incentivizing SARS-CoV-2 vaccination uptake remains limited. Studies in Europe and Canada found that introducing vaccine passports led to increases in vaccination coverage, but this impact depended on age and prior coverage.12–14 These studies have been limited by their use of provincial- or national-level data, which restricts exploration of heterogeneity by age and precludes examining the effects of vaccine passports according to social determinants of health. Given that the COVID-19 pandemic has disproportionately affected communities experiencing social and economic marginalization,4,15 it is essential to examine whether vaccination policies — including vaccine passports — resulted in socioeconomic disparities in vaccination.
Using vaccine registry data linked to area-level census information, we evaluated the impact of vaccine passports on first-dose vaccination coverage in Quebec and Ontario using an interrupted time series methodology. For each province, we estimated the impact of the vaccine passport by age, and 2 area-level social determinants: income and proportion racialized.
Methods
In Quebec and Ontario, vaccination of the general adult population (age ≥ 18 yr) and youth aged 12–17 years began in May 2021 with BNT162b2 (Pfizer–BioNTech), mRNA-1273 (Moderna) or ChAdOx1 (Oxford–AstraZeneca).16–19 COVID-19 proof-of-vaccination policies (herein “vaccine passports”) were announced on Aug. 5 (Quebec) and Sept. 1 (Ontario) and came into full force on Sept. 15 (Quebec) and Sept. 22, 2021 (Ontario).6,7,20 Non-essential activities and venues targeted by these policies (e.g., restaurants, bars, movie theatres and concerts) were similar in both provinces, and restrictions applied to those aged 13 (Quebec) or 12 (Ontario) years and older. The study period was from July 3, 2021 (to align with the end of school year) to 5 weeks after the end of the vaccine passports’ impact period (i.e., Oct. 23, 2021, for Quebec and Nov. 13, 2021, for Ontario).
Data sources and measures
We obtained vaccination data from the Registre de vaccination du Québec and Ontario’s COVaxON system,21,22 which include individuals’ dose administration date, age, and address or dissemination area of residency. Data were aggregated at the dissemination-area level — the smallest standard geographic area for which census information is available (average 400–700 residents).23 We included all individuals aged 12 years and older (vaccine-eligible population at the time of the announcement, 20.5 million people across both provinces). Age was categorized based on vaccination priority (12–17, 18–29, 30–39, 40–49, 50–59 and ≥ 60 yr). We computed weekly vaccination rates by dissemination area and age group (first doses administered per 100 000 people without a first dose). We evaluated first-dose coverage because it may better capture people’s response to vaccination mandates, whereas second-dose coverage depended primarily on time since first dose and changes in the recommended dosage interval (initially 16 weeks, shortened during the summer of 2021).24–27
We obtained dissemination area–level after-tax income, per-person equivalent from the Postal Code Conversion File Plus Version 7A/7D,28 and the proportion racialized (based on self-reported “visible minority”) from the latest available Canadian Census (2016) at the time of analysis.29 Income was ranked at the census metropolitan area or census agglomeration level (to account for within-province variability in cost of living) from lowest to highest, and proportion racialized was ranked at the provincial level from highest to lowest. This ordering was chosen such that the first quintile would align with observed data on the highest incidence of COVID-19 cases.4,15 The ranking balanced the population in each quintile (Appendix 1, Supplementary Table S1, available at www.cmajopen.ca/content/11/5/E995/suppl/DC1).
Study design
Analyses were stratified by province. We estimated the impact of the vaccine passport through an interrupted time series analysis, which assumes that the preintervention temporal trend (and postimpact period in the case of temporary changes) can be used to estimate a counterfactual scenario.30,31 We allowed for temporary changes in level and slope of the vaccination rate as a result of the policy announcement. Based on previous evidence12,14 and best-fit comparisons, the change was assumed to last for 6 weeks in both provinces: Aug. 14 to Sept. 18, 2021 (Quebec) or Sept. 4 to Oct. 9, 2021 (Ontario). Quebec’s date was lagged by 1 time unit because inspection of the raw data suggested that changes in the weekly rate were only detectable 1 week after the announcement, likely because of the announcement timing and decreased vaccination during weekends.
We replicated the main analyses restricting to dissemination areas in the Montréal and Toronto census metropolitan areas (re-ranking dissemination areas by social determinants of health).32,33 These cities are the largest census metropolitan areas of each province, have sociodemographic profiles that differ from the rest of their province, and were important epicentres of SARS-CoV-2 transmission.
Statistical analysis
Our statistical modelling approach consisted of 2 steps. First, we used negative binomial regressions with a natural spline to capture pre-announcement trends of dissemination area–level vaccination rates, adjusting for baseline vaccination coverage (i.e., July 3, 2021; categorical, 10-percentage-point intervals from < 50% to ≥ 90%).34,35 Second, we used model coefficients to obtain counterfactual vaccination rates and coverage. We computed absolute impacts of vaccine passports (observed minus counterfactual coverage) 11 weeks after the announcement (Quebec: Oct. 23, 2021; Ontario: Nov. 13, 2021). We calculated the relative increase in number of first-dose vaccinations administered between the announcement and the end of the study period.
We investigated heterogeneity in the impact of vaccine passports by age12 and area-level social determinants of health associated with higher SARS-CoV-2 infection burden.4,15 We fit 3 models in which the vaccine passport impact could vary by age, area-level income or area-level proportion racialized. To further examine trends by social determinants of health, we fit 2 models with interaction terms between age and area-level income or proportion racialized. We evaluated impact heterogeneity by assessing trends in absolute and relative impacts of the vaccine passport by age and social determinants of health. To examine how passports affected inequities in vaccination coverage, we focused on absolute impacts.
Since heterogeneities in the impact of vaccine passports could be influenced by differences in baseline vaccination coverage, we re-fit the first 3 models with an interaction term between baseline coverage and the impact of the vaccine passports. We re-estimated absolute impacts while holding baseline coverage constant (i.e., setting the baseline variable for all dissemination areas to the same value).
Confidence intervals (CIs) were obtained using 1000 bootstrap replicates, using census tracts as the resampling unit to account for geographical and temporal correlations. The 95% CIs were computed by taking the 2.5th and 97.5th percentiles.
Sensitivity analyses
We explored how alternative modelling choices affected model fit and results by re-parametrizing the age model.36 Briefly, we assessed if the start of the study period influenced conclusions by changing the time-series start (± 1 wk), assessed the robustness of results to different impact period lengths (5 or 7 wk), and examined different model specifications for the temporal trend. Fits were compared based on Akaike information criterion, Bayes information criterion and visual assessment.
Based on previous research,14 we also explored (Quebec only) whether including log-case counts in the model changed model fit or effect estimates, as they may influence individuals’ COVID-19 risk perception and decision to get vaccinated.
All analyses were carried out in R V.4.1.0, using packages “fixest” and “splines.”37–39 Full details on our modelling approach, model equations and sensitivity analyses can be found in Appendix 1.
Ethics approval
Ethics approvals were obtained from the Institutional Review Board of Faculty of Medicine and Health Sciences of McGill University in Quebec (A06-M52–20B) and the Health Sciences Research Ethics Board of University of Toronto in Ontario (no. 39253).
Results
In both provinces, first-dose SARS-CoV-2 vaccination coverage was 82% in the eligible population (age ≥ 12 yr) when the vaccine passport was announced. Coverage was highest among people aged 60 years and older (94% Quebec; 87% Ontario), and coverage for youth aged 12–17 years was 68% in Quebec and 76% in Ontario. Eleven weeks after vaccine passports were announced, vaccination coverage had increased by 5 percentage points in each province (Table 1; Appendix 1, Supplementary Table S2).
Population sizes and first-dose SARS-CoV-2 vaccine coverage for select time points in Quebec and Ontario, 2021
Pre-announcement vaccination coverage in the lowest-income dissemination areas was 9 and 7 percentage points lower than in highest-income dissemination areas in Quebec and Ontario, respectively (similar inequalities in Montréal and Toronto). There were also disparities by proportion racialized: coverage in dissemination areas with the highest-proportion racialized was 4 percentage points and 8 percentage points lower than in the areas with the lowest-proportion racialized in Quebec and Montréal, respectively. In Ontario, the reverse was found — vaccine coverage was 3 percentage points higher in the highest-proportion racialized than in the areas with the lowest-proportion racialized, and there was little difference in Toronto (< 1 percentage point; Appendix 1, Supplementary Table S3).
Observed pre- and post-announcement vaccination rates
Before the announcement of vaccine passports, weekly first-dose vaccination rates were stable in Quebec and declining in all age groups in Ontario (Figure 1). Increased vaccination rates were observed in both provinces in the week that followed the policy announcement, especially among younger age groups (12–17 and 18–29 yr). Comparable increases occurred across income and proportion racialized quintiles. These increases were sustained over 6 weeks. Similar patterns were observed for Montréal and Toronto (Appendix 1, Supplementary Figure S1).

Weekly vaccination rates in Quebec (A–C) and Ontario (D–F). Observed (points) and modelled (blue and green) vaccination rates over time are shown. Predicted vaccination rates were obtained from 3 different regression models where the vaccination rate and the impact of the vaccine passport were allowed to vary by age group (A, D), dissemination area–level income quintile (B, E), or dissemination area–level proportion racialized quintile (C, F). 95% confidence intervals were estimated via bootstrap with 1000 replicates. Note: Announ. = announcement of the vaccine passport, Implem. = implementation of the vaccine passport.
Interrupted time series: estimated impact of vaccine passports on coverage by age
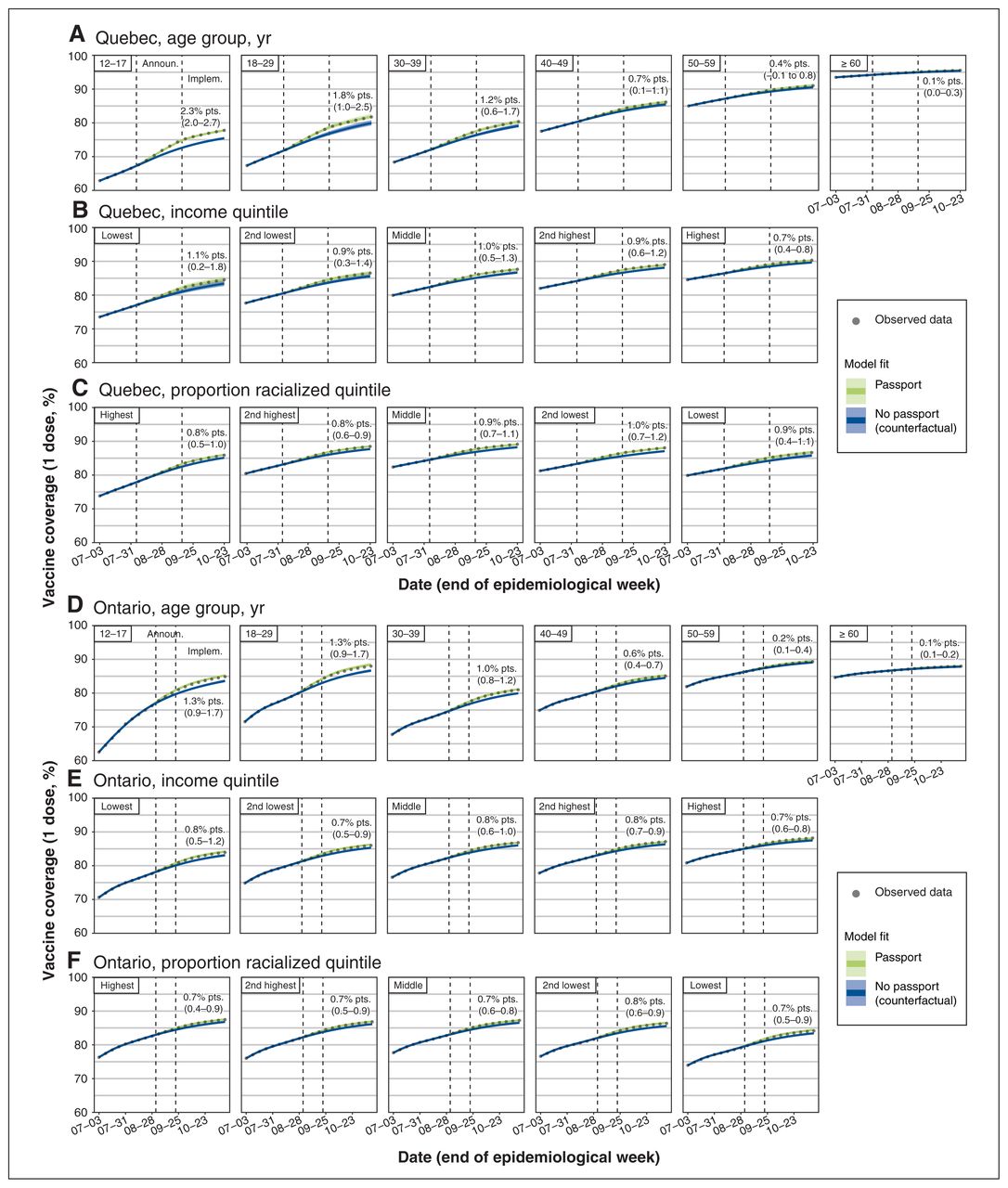
In the absence of the vaccine passports, we estimate first-dose vaccination coverage would have been 0.9 percentage points lower (95% CI 0.4–1.2) in Quebec by Oct. 23, 2021, and 0.7 percentage points lower (95% CI 0.5–0.8) in Ontario by Nov. 13, 2021. In relative terms, vaccine passports led to increases in the number of first doses administered over 11 weeks of 23% in Quebec (95% CI 10%–36%) and 19% in Ontario (95% CI 15%–22%; Figure 2).

First-dose SARS-CoV-2 vaccine coverage in Quebec (A–C) and Ontario (D–F). Observed (points) and modelled (blue and green) vaccine coverage over time are shown. Predicted vaccine coverage was obtained from 3 different regression models where the vaccination rate and the impact of the vaccine passport were allowed to vary by age group (A, D), dissemination area–level income quintile (B, E), or dissemination area–level proportion racialized quintile (C, F). Estimates and 95% confidence intervals (CIs) of the impact of the vaccine passport (observed coverage minus modelled counterfactual) are shown at the right of each panel. 95% CIs were estimated via bootstrap with 1000 replicates. Note: Announ. = announcement of the vaccine passport, Implem. = implementation of the vaccine passport, pts. = points.
The largest impact of the vaccine passport was observed in the group aged 12–17 years in Quebec, where vaccine coverage was estimated to be 2.3 percentage points higher (95% CI 2.0–2.7) than it would have been without a vaccine passport. In Ontario, the corresponding impact was an increase of 1.3 percentage points (95% CI 0.9–1.7). The smallest effects were estimated in the group aged 60 years and older, in which the impact was around 0.1 percentage points in both provinces (Figure 2A and Figure 2D). Similar age patterns were observed on the relative scale (Appendix 1, Supplementary Table S3). In Montréal and Toronto, effect sizes for each age group (except 12–17 yr in Toronto) were equivalent to provincial-level estimates (Appendix 1, Supplementary Figure S2). Observed age trends for the absolute impact remained when holding baseline coverage constant across dissemination areas (Appendix 1, Supplementary Figure S3).
Modification of the estimated impact of vaccine passports on vaccine coverage by age and social determinants of health
When examining the impact by income quintile, we found little evidence of heterogeneity in Quebec. In this province, the vaccine passport increased vaccine coverage in the lowest-income dissemination areas by 1.1 percentage points (95% CI 0.2–1.8) compared with 0.7 percentage points (95% CI 0.4–0.8) in the highest-income dissemination areas, corresponding to relative increases of 21% (95% CI 4%–40%) and 27% (95% CI 15%–36%), respectively (Figure 2B; Appendix 1, Supplementary Table S3). When stratifying by age, the estimated impact of vaccine passports was generally larger in lower-income dissemination areas in most age groups (no clear trend in the 18–29 yr group). However, uncertainty was large and CIs overlapped across quintiles (Figure 3A).

Impact of vaccine passport on first-dose coverage of SARS-CoV-2 vaccine (in percentage points) across age and by dissemination area level of income and proportion of racialized residents in Quebec (A, B) and Ontario (C, D) by the end of the study period. The impact of the vaccine passport (observed vaccination coverage minus the modelled counterfactual coverage in the absence of a vaccine passport) was estimated from 2 different regression models in which the vaccination rate and the impact of the vaccine passport were allowed to vary by the interaction of age and either dissemination area–level income quintile (A, C), or dissemination area–level proportion racialized quintile (B, D). 95% confidence intervals (in parenthesis) were estimated via bootstrap with 1000 replicates.
The impact was comparable across income quintiles in Ontario at 0.7 to 0.8 percentage points (Figure 2D), although relative increases in vaccinations ranged from 19% (95% CI 10%–29%) in the lowest-income dissemination areas to 32% (95% CI 25%–40%) in the highest-income dissemination areas (Appendix 1, Supplementary Table S3). The lack of heterogeneity in the absolute impact remained with age stratification — the estimated vaccine passport impact was larger in younger age groups but similar across income quintiles within each age group (Figure 3C).
For the proportion racialized, effects were homogeneous at the dissemination area level. In Quebec, the estimated increase in vaccine coverage was around 0.7 to 1.0 percentage points across quintiles of proportion racialized, with no clear trend (Figure 2C). The relative impact ranged from increases in vaccination of 12% (95% CI 7.5%–18%) in dissemination areas with the highest proportion racialized to 29% (95% CI 10%–41%) in the dissemination areas with the lowest proportion racialized (Appendix 1, Supplementary Table S3). Within age groups, the impact was larger in dissemination areas with lower proportion racialized, except for the group aged 12–17 years, in which the impact was larger in dissemination areas with a higher proportion of racialized residents. Although CIs overlapped across some quintiles, uncertainty was smaller than in the income analyses (Figure 3B).
In Ontario, the dissemination area–level impact was also similar regardless of the proportion of racialized residents. The absolute effect of vaccine passports was 0.7–0.8 percentage points in all quintiles, and relative impacts ranged from increases of 19% to 24% (Figure 2F; Appendix 1, Supplementary Table S3). As in Quebec, there was more heterogeneity when stratifying by age, and the impact was bigger in dissemination areas with a lower proportion of racialized residents. The effect was attenuated in older age groups, but the gradient remained in all age groups (Figure 3D).
The patterns by income and proportion racialized in Montréal and Toronto were equivalent to those of their respective provinces. One exception was the pattern in the vaccine passport impact by proportion racialized in Toronto, as there was a slight gradient only among people aged 12–29 years (Appendix 1, Supplementary Figures S2 and S4). When holding baseline vaccination coverage constant, the trends along social determinants of health remained for all cases except for income in Ontario, where there was a slight gradient in the impact of the vaccine passport (Appendix 1, Supplementary Figure S5).
Sensitivity analyses
In sensitivity analyses (age model), changing the time-series start by ±1 week did not substantially change the estimated impacts in Quebec and slightly lowered them in Ontario (Appendix 1, Supplementary Figure S6). In contrast, in models that assumed a different duration for the vaccine passports’ impact (5 or 7 wk), the effect was almost identical or slightly lower in both provinces, but model fit was poorer (Appendix 1, Supplementary Figures S7–S8). Lastly, when using the best nonspline alternative model specifications, the estimated impact of the vaccine passport was slightly higher in Quebec and lower in Ontario, compared with our spline-based approach. All impact estimates were higher in the simple log-linear model, but these methods had poor fit (Appendix 1, Supplementary Figure S9–S10).
Including a variable for reported COVID-19 cases did not meaningfully change the model fit or effect size estimates (Quebec only; Appendix 1, Supplementary Figure S11 and Appendix 1, Supplementary Table S4).
Interpretation
Vaccine passports increased first-dose SARS-CoV-2 vaccine coverage by approximately 1 percentage point in both Quebec and Ontario 11 weeks after the announcement, and first-dose vaccine coverage was above 80% (in the population aged ≥ 12 yr) at the time passports were announced. This translates to 23% (Quebec) and 19% (Ontario) more vaccinations. The impact of vaccine passports was largest among younger age groups (< 40 yr), and differences in impact by area-level income or proportion of racialized residents were relatively small and with overlapping uncertainty, suggesting that vaccine passports had a limited impact on reducing socioeconomic disparities in vaccination coverage. Additional strategies and incentives should be considered to increase coverage and reduce disparities.
In both provinces, there were inequalities in the preannouncement vaccination coverage by dissemination area–level income. However, there was only a small gradient in the impact of the vaccine passport in Quebec (i.e., higher impact in lower-income dissemination areas) and confidence intervals overlapped. In Ontario, there was little heterogeneity in the impact of vaccine passports by dissemination area–level income. Taken together, these results suggest that there was little heterogeneity by area-level income in the impact of vaccine passports.
The fact that there were inequalities in baseline vaccine coverage by dissemination area–level proportion of racialized residents in Quebec, but not Ontario, could be attributed to different vaccination policies. Quebec’s vaccine prioritization focused mostly on age and essential workers, whereas Ontario eventually implemented a “hotspot strategy,” which directed more vaccine-related resources to geographical areas with higher cumulative incidence of COVID-19 — which, on average, had a higher proportion of racialized residents.40,41 Although estimates were uncertain, larger absolute effects were observed in neighbourhoods with lower proportions of racialized residents in age-stratified analyses in both provinces. Thus, vaccine passports may have had slightly larger impacts in predominantly white neighbourhoods despite their higher baseline coverage, a heterogeneity that was masked by differences in age structure and that could result in increased disparities in lower-coverage jurisdictions.
Our effect size estimates are lower than those previously reported from Europe and Canada.12–14 Two studies that evaluated vaccine passports in Italy, France and Germany found absolute increases in vaccine coverage of 5–13 percentage points.13,14 In these countries, however, passports were announced when the fraction of people without a first dose was much larger (30%–35% v. < 20% in our study). In Canada, a study reported slightly higher effects for vaccine passports in Quebec (3.1 percentage points) and Ontario (1.9 percentage points).14 In contrast to our approach, the authors assumed that vaccine passports would have a permanent effect beyond 6 weeks and did not account for the continuous reduction in size of the population without first dose, potentially overestimating the impact of vaccine passports. Overall, these differences reinforce the importance of context when considering the potential utility of vaccine passports. These policies may have more important impacts on coverage if implemented when vaccination uptake is still low, as observed in some European countries. However, once vaccine coverage has reached a higher threshold, such as in Quebec and Ontario, additional strategies should be considered. For example, a synthetic control study in New York City estimated that a suite of policies — proof-of-vaccination policies, employer-based mandates and cash incentives — increased adult coverage by 6 percentage points despite already high coverage (83%).42
Our results should also be interpreted by considering vaccine acceptance and hesitancy as a continuum between total acceptance and total refusal.43,44 First, vaccine passport policies may have had the biggest impact on those open to vaccination but for whom it was not a priority. This could partly explain the observed age effect: younger people may have decided to get vaccinated or moved their vaccinations forward in time to maintain access to non-essential settings and activities targeted by vaccine passports. Second, there was a large “early adopter” effect by the time vaccine passports were announced. Indeed, most residents in Canada expressed positive attitudes toward SARS-CoV-2 vaccinations45 and there were various community-based efforts to improve engagement, awareness and access (e.g., community ambassador programs and mobile vaccination clinics). The group not yet vaccinated by the time of the announcements may have largely been composed of individuals experiencing long-standing, systemic and persistent barriers to vaccination or vaccine mistrust. To increase vaccine acceptance and uptake in historically marginalized communities, different strategies are needed given that vaccine mandates such as passports are not designed to address the underlying causes of hesitancy and medical mistrust, including causes stemming from systemic racism in the health care system.46–48 These interventions could include tailored promotional campaigns, combating disinformation and a strengthening of outreach and community-led vaccination campaigns.46,49,50 For future mass vaccination campaigns (e.g., for SARS-CoV-2 boosters and future pandemics), prepandemic literature on vaccine mistrust indicates that successful uptake necessitates meaningful involvement of communities in planning and implementation, better tailoring of promotional campaigns to groups at risk of low uptake, and strengthening of multicomponent approaches.51
Strengths of our study include the use of detailed dissemination area–level information on vaccinations in Canada’s largest provinces. We also conducted a range of sensitivity analyses that provided credence to our estimates. Lastly, we investigated heterogeneity of impact by age and area-level social determinants of health — known drivers of inequalities in COVID-19 burden.
Limitations
Various limitations should be considered when interpreting these results. First, concurrent events (e.g., return to school, university- and college-based mandates in Ontario, and a vaccine lottery in Quebec that offered vaccinated individuals a chance to win cash prizes) may have biased estimates of effectiveness upwards. However, school-related events would only partly affect age groups younger than 30 years, and there is mixed evidence on the impact of vaccine lotteries for SARS-CoV-2 vaccination.52,53
We used area-level measures of income and racialization, meaning that inferences on the role of individual-level income or racialization could be subject to ecological fallacy.
Our results assume that the effect of vaccine passports is temporary, in line with previous research on the subject,12,14 but this is mitigated by focusing on the first 3 months after the announcement.
Although vaccination eligibility had opened to individuals older than 12 years more than 5 weeks before the start of the study period, some people may have still faced difficulties booking vaccine appointments (e.g., limited appointments, access to child care and transportation).
Lastly, this study does not address other ways in which vaccine passports could affect SARS-CoV-2 transmission (e.g., reduced mixing between people of different vaccination status).
Conclusion
In Quebec and Ontario, vaccine passports increased SARS-CoV-2 vaccination coverage, but absolute gains were small given that the provinces already had relatively high vaccination coverage. The impact of vaccine passports was largest among younger age groups in both provinces. However, the effect of vaccine passports varied little by neighbourhood-level social determinants of health. Ultimately, policies that account for how social determinants shape barriers to vaccination may be necessary to further increase vaccination coverage and meaningfully reduce inequities in COVID-19-related morbidity and mortality.
Acknowledgements
The authors thank Geneviève Cadieux for her helpful feedback on previous versions of these analyses.
Footnotes
Competing interests: David Buckeridge reports past contractual agreements with Institut national d’excellence en santé et en services sociaux. Marc Brisson reports grants from Canadian Institutes of Health Research; Medical Research Council, UK; the Bill and Melinda Gates Foundation; the Centers for Disease Control and Prevention; Fonds de Recherche du Québec - Santé/Fonds pour la formation des chercheurs et l’aide à la recherche; the World Health Organization (WHO); the Public Health Agency of Canada; the Québec Ministry of Health and Social Services, and the Institut national de santé publique du Québec (INSPQ). Michael Hillmer reports grants from Public Health Agency of Canada and Canadian Institutes of Health Research, and is a board member for Canada Health Infoway and Canadian Institute for Health Information. Caroline Wagner reports funding through the Natural Sciences and Engineering Research Council of Canada Emerging Infectious Diseases Modelling Initiative for studying COVID-19 epidemiology in Quebec (co-applicant on the grant CANMOD). Dr. Wagner presented to WHO Strategic Advisory Group of Experts on Immunization twice about aspects related to SARS-CoV-2 vaccination. Stefan Baral is on a data safety monitoring board for a National Institutes of Health–funded study focused on suicide prevention among LGBT youth, which includes payments for meetings. Mathieu Maheu-Giroux reports a research grant from Gilead Sciences, contractual agreements with the WHO and the Joint United Nations Programme on HIV/AIDS, and past contractual agreements with Institut national d’excellence en santé et services sociaux and INSPQ.
This article has been peer reviewed.
Contributors: Mathieu Maheu-Giroux, Sharmistha Mishra and Jorge Luis Flores Anato designed the study. Jorge Luis Flores Anato, Huiting Ma, Mackenzie Hamilton, Mathieu Maheu-Giroux, Sharmistha Mishra and Reed Beall contributed to the conception of the analytical strategy. Huiting Ma, Mackenzie Hamilton and Jorge Luis Flores Anato contributed to data management. Jorge Luis Flores Anato carried out all statistical analyses. Yiqing Xia, Sam Harper, David Buckeridge, Marc Brisson, Michael Hillmer, Kamil Malikov, Aidin Kerem, Reed Beall, Caroline Wagner, Étienne Racine, Stefan Baral and Ève Dubé provided substantial input to interpret the results. Jorge Luis Flores Anato drafted the manuscript. All authors contributed to data interpretation and revision of the final manuscript. Sharmistha Mishra and Mathieu Maheu-Giroux contributed equally.
Funding: This study was funded by the Canadian Institutes of Health Research. The funder had no role in the study design, analysis or preparation of this article. Mathieu Maheu-Giroux’s research program is funded by a Canada Research Chair (Tier 2) in Population Health Modeling, and Sharmistha Mishra’s research program is funded by a Canada Research Chair (Tier 2) in Mathematical Modeling and Program Science.
Data sharing: The analysis code is available at https://github.com/pop-health-mod/vaccine-passport-release. The authors had access to data from the vaccination registries used in this study under agreements with the Institut national de santé publique du Québec and Ontario’s Ministry of Health. These data are not available for public release. The census data used in this study can be downloaded from Statistics Canada at https://www150.statcan.gc.ca/n1/en/catalogue/98-316-X2016001.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/5/E995/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.