


Abstract
Background: Métis are a culturally unique and distinct population, yet little research has evaluated their health separate from the broader Indigenous population. We sought to explore current literature regarding the health of Métis Peoples in Canada and identify potential trends and gaps.
Methods: Using the Arksey–O’Malley, 5-stage, scoping review method, we searched PubMed, MEDLINE, iPortal Indigenous Articles Portal Research Tool and pertinent reference lists using the terms “Métis,” “health” and “Canada.” Two reviewers conducted the initial searches independently, including English articles from 2012 to 2022, and focused on only Métis populations’ health within Canada. We described characteristics of the articles and themes for discussion.
Results: Of the 572 articles we identified, we included a total of 28 articles in this scoping review, of which 16 were quantitative, 9 were qualitative and 3 used mixed methods. Thirteen articles used consultation with Métis communities as part of their methods, and 8 extracted data from national surveys. One article focused on children, while all other articles focused on adults. Nine articles used data from across Canada, 6 were based in Ontario, 5 in Alberta and 4 each in British Columbia and Manitoba. Themes included health, well-being and spirituality; mental health and substance use; health conditions and risk factors; access to adequate health resources; and experiences in health care.
Interpretation: Métis-specific health research is lacking in Canada, with a gap in volume, subject matter and diversity in the demographics studied. This review illustrates the need for more research with strong community engagement to further explore Métis health and health service needs.
The Métis are 1 of 3 federally recognized Indigenous Peoples in Canada, with ancestral ties to First Nations of the Red River region and fur traders in the late 18th century.1 Métis Peoples make up over one-third of the 1.7 million Indigenous Peoples in Canada and almost 2% of Canada’s entire population.2 The Métis are a distinct Indigenous group — with their own culture, traditions, language, nationhood and way of life — who have faced ongoing impacts of colonialism in Canada, including forced removal of children to residential and mission schools, overrepresentation of Métis children in the child welfare system and land displacement strategies that have attempted to disconnect Métis from their lands.1,3–5 Métis populations continually experience jurisdictional gaps in Canada, with many funded programs for Indigenous Peoples specifically including First Nations groups and excluding Métis.4,6 Métis also face federal exclusion from the Non-Insured Health Benefits program, a federal government program that entitles registered First Nations and Inuit Peoples to some health benefits regarding prescription drugs, counselling, medical equipment and dental care.7,8 Literature suggests that Métis people, like other Indigenous groups, have poorer health outcomes than the general Canadian population, while also occupying a unique space of feeling caught between general and First Nations–specific services.9
Most of the literature available on Indigenous health aggregates health outcomes among First Nations, Inuit and Métis Peoples into a homogenous group.10 As each group is culturally distinct, there is a need to explore each community and Nation individually. For Métis Peoples in particular, previous work has suggested that they can feel excluded and discriminated against in mainstream and Indigenous-specific health services.3 It is therefore imperative to scan the existing literature to better understand the needs of Métis communities and improve their experiences accessing health care services. 9,11 Métis Peoples are often excluded from dedicated research, so this scoping review offers a unique opportunity to examine the health and breadth of health services and experiences among Métis Peoples living in Canada. Findings from this review may unmask potential health disparities faced by this specific population and support the ongoing effort to disaggregate heterogenous groups at an individual community level, from unique Métis communities as we discuss here, but also individual First Nations and Inuit communities.
Methods
Study design
This study design is based on the guidelines outlined by Arksey and O’Malley12 and further characterized by Levac and colleagues,13 and the PRISMA Extension for Scoping Reviews.14 Accordingly, we identified the research question, identified relevant articles, selected the articles; charted data and collated and reported data. Our primary research question was, “What is currently known about Métis health and health services in Canada, and what gaps in knowledge exist?”
Eligibility criteria
We selected articles that were focused on only Métis populations’ health in Canada. We excluded all articles with a broader focus that included other Indigenous communities (e.g., First Nations, Inuit). With a focus on contemporary literature and the ethical principles of the Tri-Council Policy Statement 2, we then selected only articles that were published between 2012 and 2022. We excluded systematic reviews, scoping reviews, editorials, commentaries, guidelines, policies, and other grey literature, in favour of focusing on peer-reviewed primary literature. Although systematic and scoping reviews were excluded,15–18 we scanned reference lists in these reviews for eligible articles. We also excluded any non-English language articles.19
Search strategy
We conducted a comprehensive search, including published references, of articles published from January 2012 to December 2022. We used PubMed, MEDLINE, iPortal Indigenous Articles Portal Research Tool and relevant reference lists with the search terms “Métis”, “health” and “Canada.” One author and Métis scholar (G.L.) identified additional sources based on expertise. We conducted searches in May 2022 and again April 2023. We consulted a librarian with expertise in health research to guide strategy development. The full search strategy for PubMed is provided in the Appendix 1, available at www.cmajopen.ca/content/11/5/E884/suppl/DC1.
Study selection and quality appraisal
Two reviewers (K.-L.G., K.G.H.) independently screened and selected titles and abstracts from peer-reviewed articles, and 1 additional reviewer with context expertise (G.L.) reviewed the list of articles and hand-picked any additional article that fit the study criteria (2 articles added). A spreadsheet was shared among reviewers, and 2 reviewers (K.-L.G., K.G.H.) independently extracted data. Two reviewers (K.-L.G., K.G.H.) then undertook a full-text review and revised the list of included articles until they reached full agreement. Reviewers resolved inconsistencies or disagreements in inclusion through discussion and with involvement of a third reviewer (S.B.).
Data analysis
We coded articles in Microsoft Excel according to article metrics decided by the reviewers. We extracted information on methodology, study aims (as defined by the authors), location, participant ages, findings, implications, use of community consultation (i.e., consultations with the relevant communities in study design, in execution or in contextualizing extracted data, such as creating an advisory panel, partnering with a Métis organization or other forms of consultation with Métis communities) and use of national data (e.g., Census data, Aboriginal Peoples Survey), as described by Levac and colleagues.12 If article methodology primarily involved interviews, focus groups or talking circles, and the main findings were presented as themes, then we defined the article’s methods as qualitative. If the methodology primarily focused on metrics such as extracted records or cross-sectional methods evaluating prevalence rates and quantifiable data, we defined the article as quantitative. If both elements were incorporated, we defined it as mixed methods.
After extracting these predetermined fields, each reviewer (K.-L.G., K.G.H.) assigned a main topic and message to each article, which were grouped into overarching themes that relate to aspects of Métis health and discussed by reviewers until consensus was achieved on a final set of themes. We resolved disagreements on identified themes by formal discussion until consensus was reached. We tallied themes by each article in Excel.
Ethics approval
The review did not involve human subjects research and therefore did not require ethics approval by our institutional review board.
Results
The search yielded 574 entries from PubMed, MEDLINE, and iPortal, and the content expert. After applying the inclusion and exclusion criteria, we identified 28 unique articles for the final analysis.20–45 Figure 1 illustrates the search results.
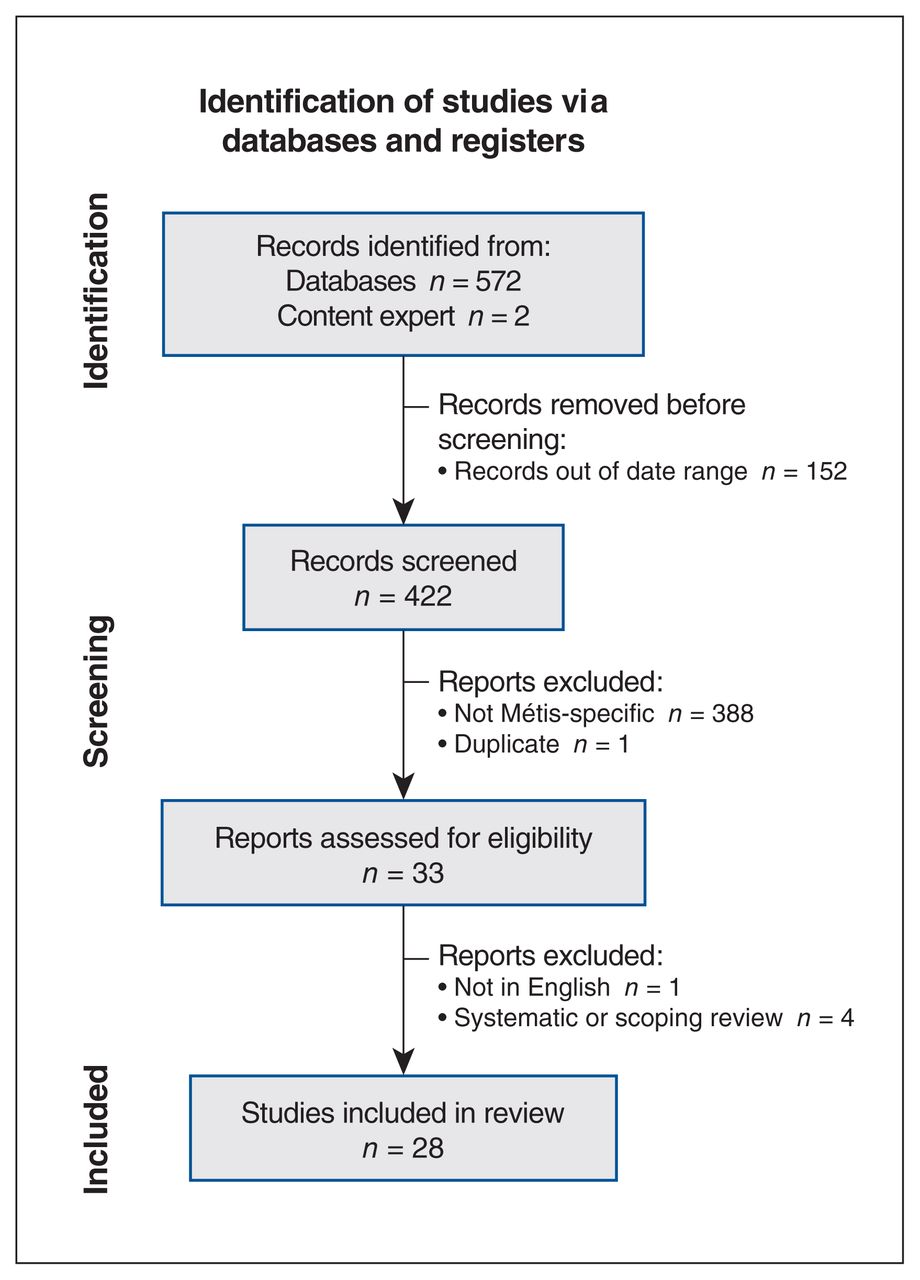
Search results.
Methodology of selected articles
Table 1 illustrates the characteristics for each selected article. Collation and summary of included articles revealed interesting trends in Métis-related research. Of the 28 articles, 16 were quantitative, 9 were qualitative and 3 used mixed methods. Quantitative articles covered vast topics, but tended to lean toward health conditions and risk factors. The qualitative articles largely centred on mental health and substance use; health, well-being and spirituality; and Métis experience in health care services. The mixed-methods articles focused on access to health services and on health, well-being and spirituality.
Description of selected studies for scoping review on Métis health in Canada from 2012 to 2022*
Of the 28 articles, 13 described consultation with the community for study design or contextualization of data, which is critical in research involving Indigenous communities in Canada, as outlined by First Nations principles of Ownership, Control, Access, and Possession (OCAP) and guidance from the Canadian Institutes of Health Research.46,47 Qualitative and mixed-methods articles had strong engagement with Métis communities throughout their methodology, whereas only 1 quantitative article included engagement with community. Eight articles used data from national level surveys, such as the Aboriginal Peoples or the Canadian Census, and did not involve any community engagement in the extraction, analysis or interpretation of the data.
Location of selected articles
We mapped representative geographical regions for each article. Nine articles reflected Canada-wide data and did not break down results according to geographic region. Six articles represented Ontario-specific Métis populations, 2 of which focused on the Toronto area. Five articles focused on Alberta, 4 focused on British Columbia and 4 focused on Manitoba. There were no dedicated articles for any other province or territory.
Ages of participants
Although all selected articles focused on Métis populations in Canada, only 1 article specifically investigated children and youth, based on how caregivers responded in the 2006 Aboriginal Peoples Survey with respect to their child. Two articles focused on an age range that included adults and children; 20 of the selected articles involved only adults, 1 focused only on older adults and the remaining 4 did not specify ages of participants in their methods.
Identified themes
We analyzed the selected articles for themes based on the topic matter, with 5 themes generated, namely health, well-being and spirituality; mental health and substance use; health conditions and risk factors; access to adequate health resources; and experiences in health care. These are summarized and described in Table 2.
Themes emerged from data coding analysis stage, accompanied by theme definitions and summaries*
The main findings of the included articles are summarized in Table 1. Several articles focused on health-related outcomes, such as prevalence of diseases (e.g., cancer) or incidence of smoking, and found that health outcomes for Métis populations in the regions identified tended to be worse than for non-Indigenous populations. In qualitative articles where Métis perspectives and experiences were sought, the key message included that Métis people felt they faced discrimination in both Indigenous and non-Indigenous service streams and a need for more Métis-specific and culturally sensitive services. Several articles linked strengths in the health and well-being of Métis people to their support network, cultural connectedness and spirituality.
Interpretation
This scoping review aimed to investigate the current literature on Métis-specific health and health services in Canada, and to identify potential gaps and trends in knowledge. Overall, we identified 28 peer-reviewed articles published in the last decade that focused specifically on Métis Peoples. We generated 5 prominent themes from these articles, namely health, well-being and spirituality; mental health and substance use; health conditions and risk factors; access to adequate health resources; and experiences in health care. More than half (n = 16) of the articles used quantitative methods, many of which drew from large, national-level surveys; 9 articles were qualitative and 13 consulted with Métis communities during the process. Most articles focused on adult populations, and both pan-Canadian and provincial focuses were present, although some regions were missing, notably Saskatchewan.
Our findings build on the previous work of Kumar and colleagues,48 which reviewed trends in Métis health literature in 1980–2009. Kumar and colleagues noted strengths in the literature, such as an increase in Métis-specific research from 1980 to 2009, a focus on a variety of health concerns (although these were largely physical health and risk factors), inclusion of both rural and urban Métis communities and an increase in the number of qualitative studies. They also noted many gaps in research including mental health and gender-specific literature, as well as work related to environment, genetics, policy and social determinants. Our review shows a continuation of many of these trends, including more research dedicated to Métis Peoples, more qualitative work and an increasing focus on mental health and substance use.
One of the primary gaps identified in our review included appropriate representation of Métis Peoples. According to 2016 Census data, Métis people reside in all provinces and territories, with most living in the provinces of Ontario, Alberta, Manitoba and BC.2 The geographic breakdown of the identified articles reflects this, but notably lacks representation in other areas where Métis reside, such as Saskatchewan. In addition, there is a notable gap in the recent literature around diverse subpopulations of Métis Peoples. Only 1 identified article investigated children and adolescents, based on the 2006 Aboriginal Peoples Survey responses by their caregivers. 24 No articles sought the perspectives of Métis youth, although youth aged 15–24 years make up 16% of the Métis population in Canada.49 Similarly, no literature explored the perspectives of Métis Elders, Métis identifying as part of 2SLGBTQIA+ communities or Métis people with disabilities. These subpopulations are likely to include unique perspectives and experiences with respect to their health and well-being.
A recurring issue among many articles in this review involved concerns around data quality, given reliance on potentially problematic sources. Nearly half of the selected articles used data from national surveys such as the 2006 Aboriginal Peoples Survey. Although this approach has some merit, namely in the volume and accessibility of data, these same articles did not participate in community consultations and lacked the perspective of the very communities they studied to help contextualize the findings or describe challenges that the Aboriginal Peoples Survey poses. There are also ethical considerations in using these types of data without community input regarding ownership and control of the data, as outlined in the First Nations principles of OCAP, as well guidance from the Canadian Institutes of Health Research and the Métis centre at the National Aboriginal History Organization.46,47,50 There are challenges with using Métis data from these sources as they allow respondents to self-identify, which results in data stemming from both the culturally distinct Métis Peoples, as we have described thus far, and people who interpret Métis to broadly mean “of mixed Indigenous and European ancestry,” which skews the data collection and results.51 However, the amount of research that meaningfully consults with Métis community members has increased, resulting in rich data that uncover the nuanced experiences of being Métis and actionable feedback that is relevant to improving health services for Métis Peoples.52
Limitations
This review did not include a search of grey literature, which could have provided additional findings and trends worth noting. We excluded literature that evaluated multiple Indigenous communities and presented Métis data as potentially disaggregated; however, this was intentional to avoid overlapping messaging among several Indigenous communities, which may have biased results, was deemed out of scope and was against our purpose of focusing on completely disaggregated data, dedicated to only Métis outcomes. We did not include non-English language articles in the review (n = 1), given the high cost of professional translation services and time commitment required. We recognize that this may potentially bias our results, exclude key findings or limit the generalizability of our findings.
Conclusion
Findings suggest a lack of Métis-specific research in Canada, but that there is an overall increase in the number of studies on this topic. Nearly half of these articles were data extractions from large surveys and lacked elements of community engagement in their methodology, thus potentially excluding key perspectives and contextualization of findings. The themes of mental health and substance use and of health, well-being and spirituality were prominent over the last decade, suggesting a priority area of research and intervention. This review highlights the need to continue health research dedicated to and collaborating with diverse Métis communities and Métis subpopulations so that health services can be improved to be more accessible and welcoming to Métis Peoples, and so that dedicated health services can be tailored to the needs of Métis Peoples.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Krysta-Leigh Gmitroski is a Métis medical student and citizen of both the Manitoba Métis Federation and Métis Nation British Columbia; she conceived and designed the study. All of the authors contributed to data acquisition, analysis and interpretation. Krysta-Leigh Gmitroski and Katherine Hastings drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was not funded.
Data sharing: This review used aggregate, published data that are publicly available. No additional data are available for sharing.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/5/E884/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools





