Article Text

Statistics from Altmetric.com
People of non-European origin form around 7% of the total UK population. Most of these are of South Asian (that is, from the Indian subcontinent) or Black African (that is, from the Caribbean and West Africa) descent. For these migrants, as for virtually all population groups living in the western world, cardiovascular disease (CVD) is the main cause of death. But there are striking ethnic differences in CVD risk. Disease presentation may differ, challenging diagnostic skills, and therapeutic requirements and responses may also not be uniform. The study of ethnic differences in CVD has provided valuable aetiological clues, not just for ethnic minority groups but also for the majority population.
ISCHAEMIC HEART DISEASE IN SOUTH ASIANS
Migrants of South Asian descent worldwide have elevated risks of morbid and mortal events because of ischaemic heart disease (IHD).1 In the UK, mortality from IHD in both South Asian men and women is 1.5 times that of the general population (fig 1⇓),2 and South Asians have not benefited to the same extent from the general decline in deaths caused by IHD over the last few decades. These ethnic differences are greatest in the youngest age groups.

Standardised mortality ratios (SMR) for heart disease and stroke in South Asians and African Caribbeans compared to Europeans, age 20–69, from 1989–92. Adapted from Wild and McKeigue,2 with permission from the BMJ Publishing Group.
These ethnic differences have been extensively studied, and while classical risk factors, such as smoking, blood pressure, obesity, and cholesterol vary substantially between subgroups of South Asians—such that in some cases, levels are equivalent to, or lower than, a comparable European population—levels of glucose intolerance, central obesity (as measured by waist to hip ratio), fasting triglyceride, and insulin are uniformly elevated compared to Europeans (table 1⇓).3 As the elevated risk of IHD is shared by all South Asian subgroups, it is clear that it is the latter group of factors which are likely to account for the susceptibility of South Asians to IHD. These factors are key features of the insulin resistance syndrome, a group of metabolic disturbances including hyperinsulinaemia, hyperglycaemia, and associated frank diabetes, and dyslipidaemia, characterised by elevated triglyceride and a reduction in high density lipoprotein (HDL) cholesterol concentrations.4 Cohort studies in other populations exploring the predictive power of insulin resistance have been conflicting, and while analysis of cross sectional data suggest that insulin resistance could account for much of the enhanced IHD risk in South Asians, definitive evidence, in the form of cohort data relating baseline measures of insulin resistance to IHD outcomes, is currently lacking.
Coronary heart disease risk factors in South Asian men by subgroup, compared with native British men. Reproduced from McKeigue et al,3 with permission
The potential importance of insulin resistance in the aetiology of coronary heart disease in South Asians has prompted researchers to explore clues as to the exact mechanisms of such an association. Attention has focused on inflammation, infection, haemostatic factors, and endothelial dysfunction. C reactive protein (CRP) concentrations are elevated in South Asians, caused at least in part by a greater degree of central adiposity which promotes CRP expression.5 CRP is highly correlated with fasting and post-load insulin, and independently predicts the risk of IHD. PAI-1 and homocysteine concentrations are also raised in South Asians, and endothelial function is impaired; these may also contribute to the elevation in IHD risk, either related to or separately from their associations with insulin resistance.5–,7
The reasons for the enhanced susceptibility to insulin resistance are disputed. It is likely that a predisposition to coronary atherosclerosis is exacerbated by exposure to western lifestyles, currently either as a consequence of urban migration within the Indian subcontinent, or of emigration.8 Thus a genetic predisposition to insulin resistance could be postulated,9 although no factor has as yet been isolated. Poor in utero development, resulting in low birth weight, in particular coupled with catch up growth in early childhood, has been associated with a greater prevalence of insulin resistance in South Asians.10 Both genetic and environmental explanations for this phenomenon have been proposed.11,12
Other factors, separate from insulin resistance, which may further account for the ethnic susceptibility to IHD include lipoprotein Lp(a), concentrations of which are thought to be largely genetically determined. Circulating Lp(a) is substantially raised in South Asians compared to Europeans,8 and separately, raised Lp(a) has been shown to increase the risk of IHD events, especially in the presence of raised low density lipoprotein (LDL) cholesterol. Again though, prospective data are lacking on the contribution that Lp(a) makes to the enhanced risk of IHD in South Asians. Dietary factors, such as the consumption of clarified fat (ghee), play a role in the dyslipidaemia observed in South Asians, with a dose–response relation between increasing ghee consumption, and raised levels of trans fatty acids and lower levels of linoleic and linolenic acid in adipose tissue, all of which adversely affect the risk of IHD.
Risk factors for IHD within South Asians
However, this does not mean that conventional risk factors are unimportant in South Asians. The risk of IHD in current smokers, for example, is four times that of a never smoker in a given South Asian population, a similar elevation in risk to that observed in Europeans. Thus, within South Asians, conventional risk factors are of immense importance in predicting absolute risks of IHD, but factors accounting for between ethnic group differences (that is, relative risks) are quite different. Because of the elevated absolute risk, and because the interrelationships between, for example, total cholesterol, HDL cholesterol, and triglyceride may differ in South Asians, conventional risk calculations may be misleading, so that the threshold at which lipid lowering therapy should be instituted may also be lower than current guidelines would suggest.
Differences between South Asians and Europeans in anatomical coronary disease
The South Asian disadvantage in terms of IHD does not simply involve risk factor status. Coronary vessels are generally smaller than in Europeans, and although appropriate for the smaller body frame, increase the technical difficulty of invasive techniques. The type of coronary atherosclerosis may also differ by ethnicity. A reappraisal of angiography studies indicates that, compared to Europeans, South Asians in the UK are more likely to have triple vessel disease, several lesions on angiography (odds ratio 2.05, 95% confidence limit 1.07 to 3.93), and non-discrete lesions (odds ratio 3.06, 95% confidence limit 1.46 to 6.42).13 As South Asians were considerably younger than Europeans in this study, it is likely that for a given age, the ethnic difference would be considerably greater. The angiographic patterns described in South Asians are similar to those observed in diabetes, and as diabetes is more common in South Asians, this could account for the ethnic difference in coronary atherosclerosis. However, an analysis stratified by diabetes status indicated that ethnic differences were not wholly dependent on diabetes status. The diabetic pattern of coronary atherosclerosis is associated with particularly adverse outcomes, but whether this holds true for the patterns observed in South Asians is not known.
Access to health care for IHD in South Asians
There is evidence that for both acute and chronic disease, South Asian people are less likely to receive appropriate and timely care. In both instances, South Asians have to wait significantly longer before being brought to the attention of a specialist, and are less likely to receive diagnostic and intervention services, despite being more likely to have disease.
The reasons for these delays are likely to be complex. When given an identical chest pain scenario, South Asians are equally likely to indicate that the pain is related to the heart, and 2–3 times more likely to state that they would seek immediate medical assistance compared to Europeans. In the primary care setting, South Asian people are more likely to be referred for investigation of upper gastrointestinal disorders, but less likely to have a positive result compared to Europeans. Distinguishing gastrointestinal and cardiovascular causes for upper body discomfort may be more challenging in South Asians, and may result in delays in obtaining appropriate care. That the history given by South Asians on admission to hospital with an acute myocardial infarction is more likely to be classified as non-typical compared to Europeans supports this hypothesis. In addition, a study of angiography outcomes showed that while revascularisation was the intended management for equivalent proportions of South Asians and Europeans, fewer South Asians actually received the intervention.14 This effect was particularly striking in older people, women and those of lower socioeconomic status, suggesting that difficulties in understanding and navigating the health care system may be responsible for lower uptake rates.
ISCHAEMIC HEART DISEASE IN AFRICAN CARIBBEANS
In striking contrast, African Caribbeans in the UK have a significantly lower risk of heart disease compared to the majority population (fig 1⇑).2 This is particularly true in men, where both morbidity and mortality from heart disease is about half that of the general population. The reduction observed in women is of the order of 20–30%, still a clinically important difference. Heart disease remains a rarity in sub-Saharan Africa, and rates in the Caribbean also appear low. Interestingly, data on African Americans from the USA are conflicting. In the early part of the last century, ethnic differences in IHD risk were similar to those observed now in the UK, however, more recent reports suggest that IHD rates are similar to or even greater than US whites. This appears to be in part explained by the degree of acculturation and miscegenation, as birthplace within or outside the USA was a strong determinant of mortality risk in African Americans dying in New York City.
A cursory comparison of CVD risk factors in the UK shows striking similarities between African Caribbeans and South Asians, with an increased risk of glucose intolerance and diabetes, and raised fasting and post-load insulin, indicating a greater degree of insulin resistance.15 However, very low density lipoprotein (VLDL), small dense LDL, and triglyceride concentrations are substantially lower in African Caribbeans than in Europeans, and the latter does not increase to the same extent in the presence of glucose intolerance (fig 2⇓).16 Further, African Caribbean men are less centrally obese than their European counterparts. These findings are inconsistent with the paradigm of insulin resistance, where glucose intolerance is associated with dyslipidaemia, characterised by raised triglyceride concentrations, and with central obesity. It is unclear why this disassociation between the hyperglycaemic and dyslipidaemic effects of insulin resistance should occur in African Caribbeans, and to date no further explanations have been forthcoming. Mortality data are not yet available to determine whether these low triglyceride values could wholly account for the African Caribbean protection from IHD. Crude calculations suggest that the combination of raised HDL cholesterol and low rates of smoking observed in this population could account for a 25% reduction in risk; however, blood pressure is substantially raised, as will be discussed later, and this would serve to increase the risk of IHD by 25%, effectively cancelling out the impact of HDL cholesterol and smoking.

Risk factors for IHD within African Caribbeans
This does not mean that IHD is a rarity in African Caribbeans in the UK. Despite a halving in relative risk, heart disease remains one of the single most important causes of death in this population, and thus requires investigation in terms of aetiology and interventions. Again, as with South Asians, it is likely that conventional risk factors will predict risk of IHD within African Caribbeans.
Access to health care for IHD in African Caribbeans
Inequalities in access to care for CVD, and efficacy of interventions, have not been studied in this population in the UK. Extensive work in the USA, where economic considerations play a much greater role in the likelihood of receiving high quality care, show clearly that African Americans are at a disadvantage, even when they come to the attention of the health services.
STROKE IN SOUTH ASIANS
South Asians also have risks of stroke that are raised 1.5 fold compared to Europeans in the UK (fig 1⇑).2 Stroke has been less well studied in South Asians compared to IHD. Blood pressure is raised in some but not all subgroups of South Asian descent (table 1⇑), and it is likely that the adverse consequences of insulin resistance may play a role in the aetiology of stroke in this population, but again this question has not been examined. Data on presentation and health care interventions are equally scant.
STROKE IN AFRICAN CARIBBEANS
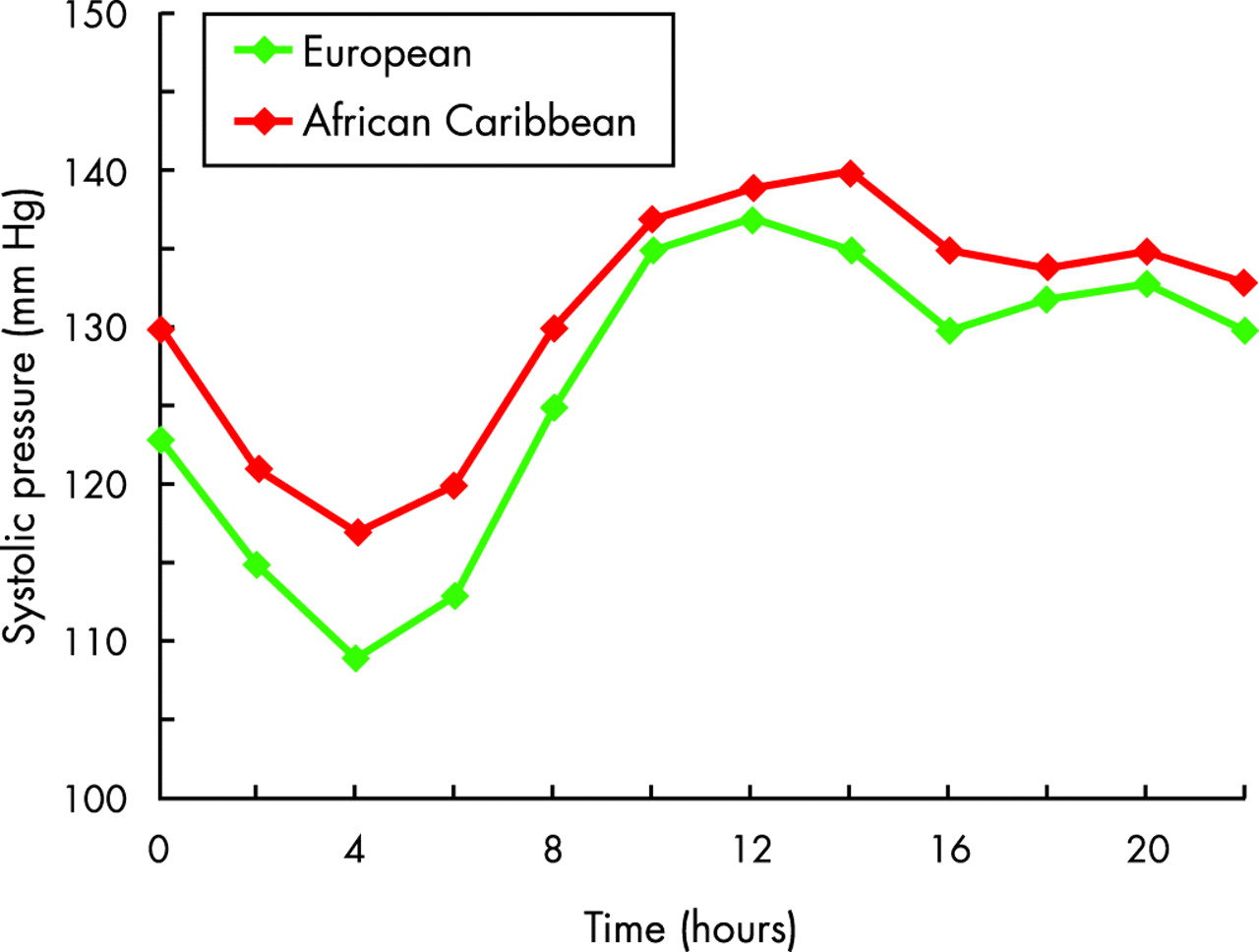
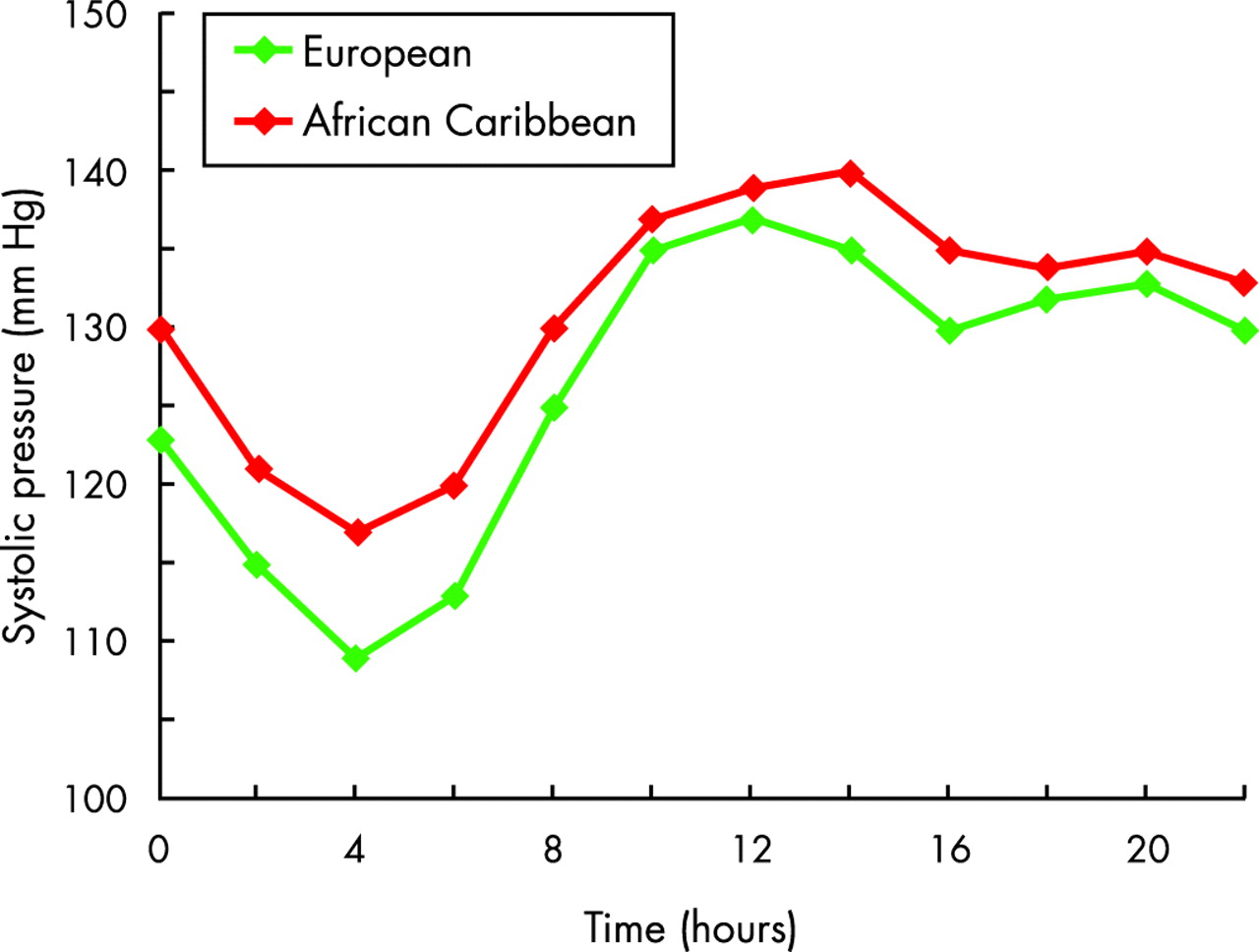
In contrast to the risks of IHD, African Caribbeans have risks of stroke that are 1.5–2.5 times greater than the general population (fig 1⇑).2,17 The majority of strokes are thrombotic, as observed in Europeans.17 However, post-stroke survival is better in African Caribbeans, presumably because of the protection from IHD.17 Stroke risks are greater in women than in men, and are reflected in ethnic differences in blood pressure, with mean resting systolic blood pressure being 6 mm Hg greater in African Caribbean men, and 17 mm Hg greater in African Caribbean women, compared to their European counterparts.15 It is likely that blood pressure elevations alone may be sufficient to account for the increased risk of stroke in women, but other explanations must be sought for men. In addition to raised resting blood pressure, nocturnal dipping of blood pressure is attenuated in African Caribbeans compared to Europeans, so that for a given level of resting blood pressure, African Caribbeans are exposed to significant elevations of “whole day” blood pressure (fig 3⇓).15 Further, there is evidence that the degree of target organ damage, be it stroke, left ventricular hypertrophy, end stage renal disease, and retinopathy, are also greater than would be expected given the level of resting and ambulatory blood pressure, and that other factors, as yet unidentified, may play a role.
{kind=link}
{kind=link}
{kind=link}
Ambulatory systolic blood pressure in African Caribbeans and Europeans. Reproduced from Chaturvedi et al,15 with permission.
HYPERTENSION AND ANTIHYPERTENSIVE THERAPY IN AFRICAN CARIBBEANS
The type of hypertension also differs, being of the low renin type, and also being more salt sensitive than other populations, particularly in the context of a low potassium intake. Further, it is evident that the type of target organ damage differs by ethnicity. African Caribbeans are likely to exhibit concentric as opposed to eccentric remodelling of the left ventricle as a consequence of hypertension. This former pattern appears to have a greater risk of mortality.
The response of people of black African descent to antihypertensive treatment has been extensively studied, but the results are conflicting. Much of the data come from the USA, where African Americans share a susceptibility to hypertension and its sequelae. These studies initially suggested that people of black African descent are poorly responsive to angiotensin converting enzyme (ACE) inhibitors, largely as a consequence of the frequency of low renin hypertension. This finding has been contested by others, most notably in the AASK study where the calcium channel blocker limb was terminated early because of the greater beneficial effects with ACE inhibitors in African Americans. However, ALLHAT, the largest trial of hypertensive individuals to date with around 11 000 African Americans, demonstrated equivalence of thiazide diuretic with calcium channel blocker intervention in this population, with an indication that outcomes were poorer in the ACE inhibitor arm.18
HEART FAILURE IN SOUTH ASIANS AND AFRICAN CARIBBEANS
Rates of IHD and stroke have generally been falling in westernised populations, but heart failure rates are likely to increase, partly because of an aging population, and partly as a result of improved survival from myocardial infarction. There are several population based studies of heart failure in the UK, but these have included very few people of ethnic minority descent. A hospital based audit in Birmingham provides limited data,19 but must be treated with caution, as a hospital based study cannot fully take account of ethnic specific biases in referral and admission rates. However, a re-analysis of these data, using census estimates at the time of the study to provide the denominator, indicates that the risk of heart failure, compared to Europeans, in those aged 60–79 years was 3.1 (95% confidence limits 1.9 to 4.9) in African Caribbeans, and 5.2 (95% confidence limits 3.7 to 7.4) in South Asians. It is difficult to anticipate whether known ethnic differences in cardiovascular disease and diabetes risk, established primarily in middle aged populations, could account for such large ethnic differences in heart failure risk. The impact of, for example, the greater burden of IHD in South Asians on heart failure is difficult to estimate, in part because the ethnic difference in IHD at older ages has not been properly established, and in part because the impact of the interaction between hypertension, IHD, and diabetes on heart failure in this ethnic group is unknown. Extrapolations from observations in other ethnic groups may be misleading.
PERIPHERAL VASCULAR DISEASE IN SOUTH ASIANS AND AFRICAN CARIBBEANS
In contrast to IHD, peripheral vascular disease (PVD) has been poorly investigated in South Asians. In general, populations and individuals at high risk of IHD will also be at high risk of PVD, as often risk factors and disease mechanisms are shared. It is therefore striking that, in studies of both the general and diabetic populations in the UK and in India, PVD rates are substantially lower in South Asians than Europeans, with a 50–75% reduction in risk. Reported rates of hospital admission for PVD in South Asians in the UK were half those anticipated from population estimates (3% v 7%). There are concerns regarding the completeness and accuracy of such hospital derived data, and ethnic biases in likelihood of admission to hospital. Extrapolations from diabetic populations are valid, however, as ethnic differences in cardiovascular disease risk appear to reflect those in the general population, even in minority ethnic groups. Thus, in a population based study of people with diabetes, the prevalence of PVD, assessed by a history of claudication and palpation of peripheral pulses, was 25% in Europeans and 9% in South Asians (p = 0.02). This may be due to an under reporting of claudication in South Asians. However, the UK prospective diabetes study (UKPDS) reported that missing foot pulses, a more objective measure of PVD, were also two- and threefold more common in European women and men, respectively, than in South Asians.20
Ethnic differences in cardiovascular disease: key points
South Asians have increased risks of heart disease compared to Europeans, probably because of increased levels of insulin resistance and associated factors such as inflammation and endothelial dysfunction
African Caribbeans have low risks of heart disease compared to Europeans, even though insulin resistance rates are high. Ethnic differences in lipids and lipoproteins may account for this protection
Within each ethnic group, conventional risk factors, such as smoking and cholesterol, will still predict those at high risk
Modes of presentation and therapeutic needs may differ by ethnicity, calling for increased awareness of cultural differences in presentation, and for data on the impact of interventions in different ethnic groups
First generation migrants have now reached pensionable age as a group, so that cardiovascular disease conditions of older age, such as heart failure, will emerge as a dominant cause of ill health
Both ethnic groups have not enjoyed the decline in cardiovascular disease to the same extent as that observed in the UK. This supports renewed efforts for prevention at both primary and secondary levels
Given the concordance between coronary, cerebral, and peripheral atherosclerosis observed in other populations, the degree of disassociation observed in South Asians is puzzling and requires investigation.
Again, there are fewer data on PVD in African Caribbeans than in South Asians. In diabetes, according to the UKPDS, PVD appeared to be less frequent in African Caribbeans than Europeans.20 These low rates of PVD are congruent with the low risk of coronary heart disease found in African Caribbeans, but are in notable contrast to the high rates of stroke and hypertensive heart disease.
PREVENTION OF CARDIOVASCULAR DISEASE IN SOUTH ASIANS AND AFRICAN CARIBBEANS
Aspects of primary prevention differ in some respects in ethnic minority groups when compared with the general population. An emphasis on stopping smoking may be less relevant in some South Asian groups, particularly women, where smoking rates are strikingly low. While ghee consumption is clearly atherogenic, and should be specifically discouraged, consumption of saturated fat in general is not appreciably raised compared to Europeans. Similarly, diets of African Caribbeans in the UK are relatively healthy, although there appears to be a convergence towards the more unhealthy patterns observed in the general population in second generation African Caribbean migrants.21 For both ethnic groups, obesity control via dietary interventions and increased physical activity are likely to be critical in reducing CVD risk. It is important to recognise that definitions of obesity derived in European populations may be inappropriate for ethnic minority groups, where obesity distribution appears more important, and where differences in body frame invalidate conventional thresholds. Dietary advice should take account of specific foodstuffs consumed by these groups, and recommendations for increasing physical activity should be supported by the availability of women only facilities. There are as yet no studies in the UK of the long term efficacy of specific intervention programmes, and success is likely to depend upon societal change. Health behaviours and resulting disease risks may be very different in second and third generation migrants, where smoking rates and dietary intakes are converging towards those of the general population. In addition, studies in children suggest that ethnic differences in CVD risk are already present at a young age, with pronounced differences in insulin and triglyceride values. The challenge now is to ensure that prevention and treatment services are ready to respond to these demographic changes.
REFERENCES
Supplementary materials
. Web-only References
Available as a PDF (printer-friendly file)Files in this Data Supplement: