Article Text

Abstract
Background: Identification of hereditary predisposition to cancer has limited significance if not followed by efficient cancer prevention in the family. Probands are traditionally left to inform their relatives about the increased risk, but distant relatives may remain uninformed. An approach to contacting directly at-risk persons assumed to be unaware of their increased cancer risk was taken. With cancer prevention as the ultimate goal, the study was aimed at investigating attitudes towards and psychosocial consequences of this novel strategy.
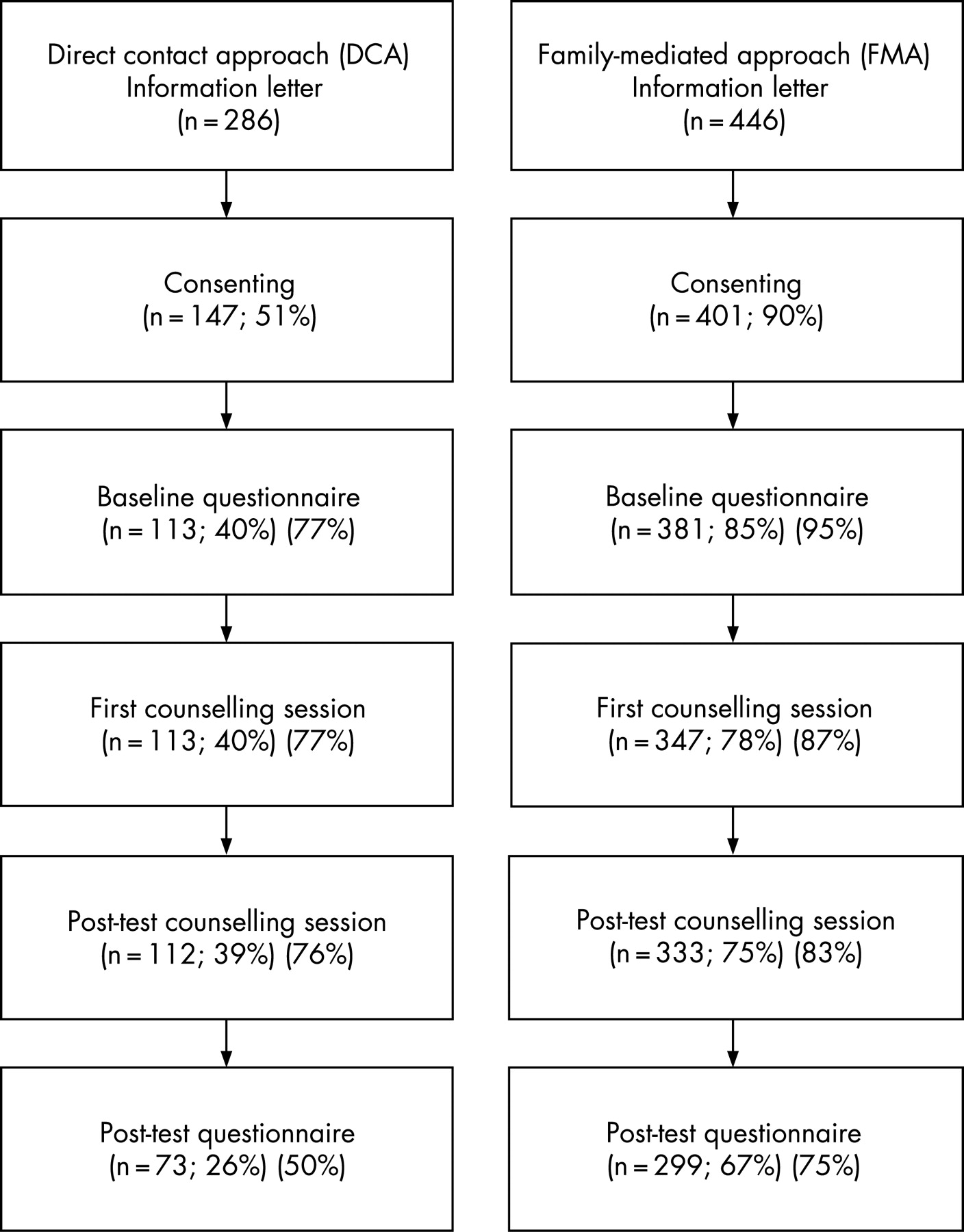
Methods: In families with hereditary non-polyposis colorectal cancer (Lynch syndrome), 286 healthy adult relatives with a 50% risk of a predisposing mutation were contacted by letter. Of these, 112 participated in counselling and predictive testing. Baseline information and information obtained 1 month after the test for 73 respondents were compared with 299 corresponding subjects, approached via the proband (family-mediated approach in our previous study) in these families.
Results: After the contact letter, 51% consented to the study. Of these, 92% approved of the direct contact and 33% had tried to seek information. In 34% of the mutation carriers, neoplasia was identified in the first post-test colonoscopy. Although post-test fear of cancer increased among the mutation carriers and decreased among noncarriers, almost all participants were satisfied with their decision to participate, independently of their test results, parallel to the family-mediated approach.
Conclusion: In this large-scale study, relatives in cancer families were actively contacted to inform them of the condition and genetic counselling. Their attitudes were encouraging, and the psychosocial consequences were similar to the family-mediated approach. Our results suggest the appropriateness of direct contact as an alternative method of contact in cases of life-threatening treatable disease.
- HNPCC
- hereditary non-polyposis colorectal cancer
- Lynch Syndrome
- direct contact approach
Statistics from Altmetric.com
In families with inherited diseases, the current practice is to encourage the patients to inform other family members and encourage them to contact clinical geneticists. This family-mediated approach is an efficient way to disseminate information to at-risk relatives in many circumstances. Studies investigating communication in cancer families, however, have revealed that informing relatives is mentally challenging for the patient, especially when distant relatives are concerned.1 Discussing this type of information is discomforting,2 there is concern about upsetting relatives,3 4 and probands tend to inform the nuclear family rather than more distant relatives.5 Therefore, some relatives may remain unaware of a serious genetic condition segregating in the family.
Hereditary non-polyposis colorectal cancer (HNPCC, also called Lynch syndrome) is an autosomal dominant syndrome caused by mutations in DNA mismatch-repair genes, mostly MLH1 or MSH2.6 It predisposes to cancer with early onset, the peak incidence occurring between 30 and 50 years of age.7 8 Predictive genetic testing allows identification of mutation carriers. Regular surveillance aiming at early detection of tumours substantially reduces morbidity and mortality from colorectal cancer and increases life expectancy.9 10 Informing all at-risk relatives can therefore be extremely valuable.
The balance between confidentiality and duty to warn relatives is an ongoing debate.11–19 Because of our clinical experiences with families with HNPCC, we felt obliged to contact high-risk individuals directly because some of the non-tested members (who had not applied for genetic counselling as part of our earlier predictive genetic-testing programme)20 developed colon cancers. Without exception, these cancer patients expressed disappointment that their relatives had not warned them of their at-risk status. In addition, our previous findings about the large-scale genetic-testing programme had been encouraging, confirming high levels of satisfaction and no serious psychological side-effects related to testing.20–22 These results have since been confirmed by other studies showing similar trends.23–25 Several groups have proposed that the duty to warn patients may outweigh the requirement for confidentiality in cases of life-threatening disease where prevention exists.15–19 Of 56 mainly international guidelines on genetic counselling related to genetic testing, 43 discussed confidentiality, and 12 of these acknowledged that confidentiality can be breached in order to prevent harm in cases of serious, imminent or treatable conditions.26 Thus, the resolution of the conflict between confidentiality and the duty to warn is not unambiguous.
With cancer prevention as our ultimate goal, we contacted all those family members at 50% risk of HPNCC who had not yet been involved in genetic counselling, in order to offer information on inherited cancer risk. Concurrently, we aimed to examine attitudes and reactions towards this direct-contact approach (DCA), and to compare the data with the results that already existed from our earlier study on family members who had been informed by their relatives (family-mediated approach, FMA). To our knowledge, this is the first large-scale hereditary cancer study to report attitudes to DCA recruitment and psychosocial responses to genetic-risk communication comparing two different approaches.
PARTICIPANTS AND METHODS
Study population
In 2003, the Finnish HNPCC registry included 110 families with a known pathogenic mismatch-repair mutation.27 Genetic counselling and predictive testing had been offered to all high-risk family members who could be reached via other family members, including those in our previous research programme.20 In total, 1420 individuals had received a test result; 644 mutation-positive and 776 mutation-negative.27 The registry works as a research database of patients and high-risk members.19 27 During previous molecular genetics studies, complete pedigrees had been constructed using the population and cancer registries, and therefore we were aware of 286 unaffected relatives (no personal history of cancer), aged 27–90 years, who had a 50% risk of having the pathogenic mutation and who were assumed to be unaware of their increased cancer risk.
Study procedures
The study plan was accepted by the ethics committee of Jyväskylä Central Hospital in 2003. We contacted all high-risk subjects (n = 286) by letter, with an enclosed reply letter containing an informed consent form. In the letter, the subjects were asked about their interest in participating in a study focused on hereditary cancer. The letter did not state that a hereditary cancer had occurred in their family. The subjects were asked to consent to receiving a phone call from our research nurse. Those consenting were telephoned and informed about the possibility of hereditary cancer in their family, and offered participation in genetic counselling and a possible gene test. A pre-test questionnaire was sent to those who agreed to participate in the study. After returning the questionnaire, they were directed to genetic-counselling units in their hospital districts. In the first counselling session, the pedigree was drawn according to the counselled subject’s knowledge. If the subject had no knowledge of cancer in the family it was stated, vaguely, that the counselling staff had received information of occurrence of an HNPCC-related cancer in their family, and that for confidentiality reasons the identity of the affected relatives could not be given. The benefits and disadvantages of a predictive gene test were discussed, including psychological reactions and possible difficulties in employment or insurance coverage in the future. Usually, the counselled subjects made their decision at the end of the session but some wanted more time for reflection. Those who chose to take the test signed a consent form and donated a blood sample for the predictive genetic test. Post-test counselling was arranged and mutation-positive subjects were referred for regular colonoscopies, and women were also referred for gynaecological examinations. A post-test questionnaire was sent to those tested 1 month after the test disclosure session. No rounds of reminders were sent to avoid any feelings of pressure.
The data of the subjects in the DCA study were compared with data (n = 446) from a FMA study on predictive genetic testing for HNPCC conducted between 1995 and 1998, including corresponding questionnaire assessments and testing procedure.20–22 The only differences in the two approaches were the contents of the contact letters, which were designed according to the assumed previous knowledge of cancer, and the number of questionnaire reminders. In the DCA study, the contact letter was sent only once in order not to create anxiety among those who did not want to respond. In the FMA study, two rounds of reminders were sent.
Measures
Most of the questions (sociodemographic variables, previous history of colonoscopy, pre-test risk perception, satisfaction with life, state of anxiety, fear of cancer and death) had been used in previous studies,20–22 whereas some were designed specifically for this study (opinions of direct contact via professionals and occurrence of cancer in the family).
We assessed attitudes to direct contact and experience of familiar cancer from answers to questions with the following options.
Do you approve of active contact taken by healthcare professionals when it concerns the cancer cases in the family? (1, no; 2, have no opinion; 3, yes)
Do you know one or more cancer patients in your family? (1, yes; who?; 2, no)
Do you think there might be more cancer than on average in your family? (1, no; 2, yes)
If you do think so, have you tried to seek information related to this (1, no; 2, yes) and were you worried about it? (1, no; 2, yes)
Have you attended a colonoscopy? (1, no; 2, yes)
Pre-test risk perception (risk of having familial cancer) was measured by the following options (1, low; 2, medium (higher than average); 3, high).
General anxiety was measured by the state measure of the State-Trait Anxiety Inventory (STAI), which is a 20-item scale.28 The answers to questions are scored on a 4-point scale. Response categories range from 1 (not at all) to 4 (very much so). Scores range from 20–80, higher scores indicating greater state anxiety. Cronbach α was 0.9 in every measurement, indicating high internal consistency.
Fear of cancer and death were measured with items derived from the Illness Attitude Scale, originally developed by Kellner and translated and culturally adopted for Finland by Aro.20
Are you afraid of that you may have cancer?
Does the thought of death scare you?
Are you afraid of dying soon? (0, no; 1, rarely; 2, sometimes; 3, often; 4, most of the time).
Attitudes to the future and satisfaction with life were assessed from the following questions:
What does your future look like? (0, extremely negative; 1, rather negative; 2, have no opinion; 3, fairly promising; 4, extremely promising)
Are you satisfied with your life in general at the moment? (0, extremely dissatisfied; 1, rather dissatisfied; 2, neither satisfied nor dissatisfied; 3, fairly satisfied; 4, extremely satisfied).
Statistical analysis
We used the χ2 test to examine differences for categorical variables and one way analysis of variance (ANOVA) for continuous dependent variables. When we examined the differences between the two studies in bivariate baseline associations, logistic regression was used for categorical and ANOVA for continuous outcome variables. In the case of skew-dependent variables, we used the non-parametric Mann–Whitney test for comparing two independent samples. Changes in outcome variables from the baseline to 1-month follow-up were analysed with repeated measures analysis of covariance, age being a covariate. If assumptions of sphericity were not met, the Greenhouse–Geisser correction was used for correct F ratios. Two-tailed p values l<0.05 were considered significant. All data analyses were performed with SPSS for Windows V.12 (SPSS Inc., Chicago, Illinois, USA).
RESULTS
Characteristics of study patients
In the DCA study, of the 286 contacted subjects, 51% consented, 39% did not respond and 10% actively refused to participate (table 1). In the FMA study, 90% consented, 8% were non-respondents and 2% refused. In the DCA group, the overall mean age was 10 years older than in the FMA group. In the DCA study, the subjects actively refusing were significantly older than those consenting or not responding. In both approaches, unmarried people were more likely to be non-respondents. None of the tested interaction terms were significant, indicating that the associations between consenting variable and demographic variables were similar in both studies.
Completion of predictive genetic testing and study questionnaires
The attrition rate was higher in the DCA than in the FMA study (fig 1). Of those consenting, 76% (112/247) in the DCA and 86% (333/401) in the FMA study took the test and received results (χ2(1) = 3.58, p = 0.06) of which 28% (n = 32) and 30% (n = 99) were mutation-positive.
{kind=link}
Attitudes towards direct contact and experience of familial cancer
Of the DCA baseline respondents, 92% approved of direct contact by healthcare professionals, 7% were unsure and one respondent disapproved (table 2). Of the respondents, 97% knew someone with cancer in their family and 74% considered there was a greater than average cancer rate in their family. Of the latter group, 51% had been worried about it and 33% had tried to seek more information. Only 21% reported previous colonoscopy examination, significantly fewer than the 63% in the FMA study (χ2(1) = 59.32, p<0.001).19 In total, 64% of those in the DCA study and 71% in the FMA study perceived their pre-test risk of getting cancer as being higher than average (χ2(2) = 2.09, p = 0.35).
Longitudinal analysis of psychosocial measures
Table 3 lists the mean scores on psychological variables at baseline and 1-month follow-up for the DCA and FMA studies. Baseline differences between the two studies, after adjusting for age, were tested with the analysis of covariance. The only variable with statistical significance was attitude towards the future: subjects in the DCA study had higher mean scores (F(1.49) = 5.0, p = 0.03), indicating a higher expectation of a positive future. Attitude towards the future was the only variable for which the change between baseline and follow-up was remained the same for the DCA study but increased for the FMA study subjects (table 3). This association remained significant after adjusting for age (F(1.37) = 16.4, p<0.001).
In total, 51 mutation-negative and 21 mutation-positive subjects returned the 1-month follow-up questionnaire in the DCA study. Fear of cancer increased among the mutation-positive and decreased among the mutation-negative subjects (F(1.68) = 4.5, p = 0.04). No other significant differences were found between mutation-positive and mutation-negative subjects in the DCA study for changes with time for the psychological variables listed in table 3.
Most respondents were very satisfied that they took the test (table 4). There was no difference in trust about the test result between the mutation carriers and non-carriers (table 4). The question about whether they would have taken the test in the light of their present knowledge showed no differences between the groups defined by mutation status. When we compared these variables between DCA and FMA study subjects,19 no significant differences were found according to the Mann–Whitney U test (data not shown).
Clinical findings among the mutation carriers in the DCA study
In the post-test colonoscopy, colorectal carcinoma was found in four people (mean age 58.5 years, range 48 to 74) and two of these were locally advanced, with lymph-node metastases. An adenomatous polyp was found in seven mutation carriers (mean age 56.9 years, range 45 to 59).
DISCUSSION
In hereditary diseases, it may be controversial to respect the patient’s right to keep his/her genetic information secret and, simultaneously, acknowledge the family members’ right to know. The issue is particularly problematic in serious conditions where early diagnosis or treatment would considerably improve the outcome. A legal dilemma may even exist if data obtained from the official cancer and health registries, or confidentially from patients is used in informing relatives against the wish of the patient.19 Alternatively, genetic information can be seen as the property of the near relatives as well,15 and it has been argued that the duty to warn may outweigh the duty to keep confidentiality.15–19
This study addressed the important topic of actively identifying individuals at risk for hereditary cancer susceptibility from families with a known HNPCC mutation, and informing them of their cancer risk. This active recruitment is a novel approach and it raises the ethical dilemma of respect for autonomy and privacy versus beneficence and the duty to warn. To our knowledge, this is the first prospective large-scale hereditary cancer study to report attitudes towards a direct-contact recruitment method and to compare psychosocial responses to am FMA study.
Consent for contact and participation in counselling and testing were lower in the DCA study (51% and 40%) than in the FMA study (90% and 78%). A lower participation rate was expected for several reasons. Firstly, subjects in FMA were better informed of the study (two-thirds of them had even been regularly followed by the HNPCC surgeons). In the FMA study, only 2% actively refused whereas in the DCA study the proportion was 10%. However, it remained unclear whether the 39% not responding really did not want to gain more information about HNPCC (independent of whether they were aware of the genetic susceptibility) or whether they just ignored the letter because it was too generally designed. In contrast to the DCA study, the contact letter in the FMA study directly informed the recipient of HNPCC running in their family, and perhaps correspondingly, only 8% did not respond at all.
The current study did not create visible adverse reactions, which raises the important question of whether a direct-contact letter should include more detailed information to increase the participation rate. In a recent study from South Australia, Suthers et al found a similar rate of participation (40%) using direct intervention to approach relatives whose contact information they had received from the proband.29 This was significantly higher than their historical data (23%) obtained from clinical practice based on family-mediated counselling. In their study, most of the contacted relatives were members of families with BRCA1 and 2, which may explain the low rate of participation in their counselling clinics, given the challenges in cancer prevention in BRCA1/2 gene carriers. The main outcome measure in their study was participation in genetic testing, and in contrast to the present study, attitudes to direct contact, psychological consequences or clinical findings in cancer surveillance were not reported.29
Our DCA managed to disseminate the message to nearly half of the remaining at-risk members in Finnish HPNCC families. In fact, one-third of them reported that they had already tried to seek information of cancer in their family; for instance, some respondents had consulted their general practioner, who had not recommended genetic or gastroenterological consultations. In our DCA study, the mean age of the family members contacted directly was clearly higher than the recommended age to start colonoscopy surveillance (25 years for mutation-positive people). Accordingly, among the 32 mutation-positive subjects, colorectal neoplasia was found in 11 (34%) in the first post-test colonoscopy, two of them locally advanced. This underlines the importance of having explicit information of hereditary cancer sufficiently early to receive clinical surveillance to prevent cancer.
We anticipated the possibility of negative reactions either from the probands or some of the relatives approached, but we faced neither legal action nor adverse reactions. During the genetic counselling, some subjects counselled were at first curious to know who were the cancer patients in their family, but easily understood why any personal data could not be revealed. There may have been important reasons why the proband had not contacted these relatives; for instance, the proband may have known that these relatives would be less willing to receive such information, as discussed in the introduction of this article. Unfortunately, we have no explicit data on this.
The people in the DCA group who consented to our study were very satisfied with their decision to participate in testing in all phases of the study, independently of their genetic test results. Several factors might explain the positive attitude towards the direct contact. The possibility of preventing a serious disease was experienced as positive, as expected. Furthermore, the mutation test results were interpreted by a professional in an individual face-to-face counselling session and cancer surveillance was organised. Apparently, potential future difficulties with health and life insurance policies did not worry the participants, probably due to the fact that such insurance has a minor role in the social security system in Finland.
One of the major problems in most HNPCC centres around the world has been suboptimal coverage of family members, which has decreased the efficiency of cancer prevention.30 31 In the well-known family G, first described by Warthin in 1913 and further revised by Henry Lynch et al, only 40 members have had predictive genetic testing to date, resulting in 5 mutation carriers among 665 living family members.32 Thus, the carrier status for the majority of family members has remained unknown. The situation in Finland makes constructing pedigrees and contacting family members in a research setting relatively easy. Because of the existence of the population register centre, it is possible to obtain a comprehensive pedigree map and contact all living family members. Medical death certificates have been registered since 1936 and all cancer cases since 1953, enabling identification of obligate mutation carriers in earlier generations, even though they may have been deceased long before HNPCC was diagnosed in the family. This background data has facilitated the identification of at-risk people and organisation of surveillance regardless of the place of residence. Interestingly, in Denmark, a ministerial directive has recently raised the possibility of transmitting information directly from counselling clinics to relatives. However, in most cases, the first choice has been to transmit the information via counselled individuals.18
The direct approach has a high likelihood of working well in countries such as Finland and Denmark, in which registries are available that can facilitate active recruitment. The model might have to be modified in other countries, such as the US, where such comprehensive registries do not exist, and contact information for at-risk relatives would have to be gathered from the proband. Additional and complementary strategies might include public-health campaigns that increase awareness of the importance of family history in disease susceptibility, which would benefit health professionals and the public. Another strategy might be the development of family history tools that could help facilitate collection and organisation of family medical history by the public.
Limitations of the study
There are several limitations to this study. Firstly, we obtained very little information about those who did not complete the baseline questionnaire, and the opinions of those not responding or those actively refusing are not known. Secondly, the attrition in the DCA group was higher, with 50% completing the post-test questionnaire in contrast to 75% of the FMA group. One apparent explanation is the lack of questionnaire reminders in the DCA study compared with two reminders in the FMA study.
The FMA group was studied during 1995–1998, whereas the DCA group was sampled in 2003. This raises the possibility that some differences observed between the two groups could be due to temporal factors for which we could account. Despite these differences, comparing psychosocial outcome variables with our previous study was considered more informative than mean scores from the present study only.
It should also be noted that the psychosocial consequences were assessed at relatively general levels, which may mask more complicated reactions and the results are based on a relatively short-term follow-up. Further studies using more wide-scale validated instruments are needed to understand more thoroughly the impact of the testing in DCA setting.
CONCLUSION
We directly contacted 286 family members at risk for HNPCC, and 51% consented, resulting in attendance for genetic counselling and predictive genetic testing. The ultimate clinical aim of the direct contact was to detect cancer sufficiently early for treatment. Of 32 identified mutation carriers, the first post-test colonoscopy revealed neoplasia in 34%, most with a good prognosis. The attitudes to this novel direct-contact approach were encouraging and we observed neither adverse reactions nor legal action. The present results support the appropriateness of direct contact as a supplementary process in cases of a life-threatening treatable disease in countries with feasible legislation and social circumstances.
Key points
We directly contacted at-risk individuals in families with HNPCC who were assumed to be unaware of their increased cancer risk.
With cancer prevention as our ultimate goal, we investigated attitudes towards a direct-contact recruitment method and also compared psychosocial responses to a family-mediated approach study.
Of those directly contacted, 51% consented to the study. Of these, 92% approved of the direct contact and 33% had tried to seek information.
In 34% of the mutation carriers, neoplasia was identified in the first post-test colonoscopy.
Although post-test fear of cancer increased among the mutation carriers and decreased among noncarriers, almost all participants were satisfied with their decision to participate independently of their test results, which is comparable with the family-mediated approach.
We conclude that our results suggest the appropriateness of direct contact as an alternative method concerning a life-threatening treatable disease.
Acknowledgments
We thank the clinical geneticists Kristiina Aittomäki, Brita Liljeström, Satu-Leena Sallinen, and Outi Vierimaa for expert genetic counselling and Mrs Tuula Lehtinen for her assistance. This study was supported by Finnish Cancer Society, and Keski-Suomi Health Care District, and partly by EuroGentest, an EU-FP6 supported NoE contract number 512148.
REFERENCES
Footnotes
Competing interests: None declared.
- Abbreviations:
- DCA
- direct contact approach
- FMA
- family-mediated approach
- HNPCC
- hereditary non-polyposis colorectal cancer
- STAI
- State-Trait Anxiety Inventory