Article Text

Abstract
Palliative care is recommended for patients with end-stage heart failure with several recent, randomised trials showing improvements in symptoms and quality of life and more studies underway. Future care planning provides a framework for discussing a range of palliative care problems with patients and their families. This approach can be introduced at any time during the patient's journey of care and ideally well in advance of end-of-life care. Future care planning is applicable to a wide range of patients with advanced heart disease and could be delivered systematically by cardiology teams at the time of an unplanned hospital admission, akin to cardiac rehabilitation for myocardial infarction. Integrating cardiology care and palliative care can benefit many patients with advanced heart disease at increased risk of death or hospitalisation. Larger, randomised trials are needed to assess the impact on patient outcomes and experiences.
Statistics from Altmetric.com
Life is pleasant. Death is peaceful. It's the transition that's troublesome. Isaac Asimov
Introduction
WHO defines palliative care as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual”.1 In 2014, WHO resolved that palliative care should be integrated in all settings and by all hospital specialties in its member countries. A holistic palliative care approach, for patients with congestive heart failure (CHF) is of fundamental importance although reports from around the world suggest that implementation falls short of expectation.2–5 Despite limited trial evidence, there is clear justification for improving holistic care for people whose health is deteriorating with end-stage heart failure given its very poor prognosis and severe symptoms.6 Recently published heart failure guidelines recommend that palliative care be an integral part of treatment and care in advanced disease, with evidence grade ranging from level B,7 to good practice points8 although one CHF guideline concludes that there is a lack of evidence for palliative care outcomes.9 This disparity reflects an eagerness to include palliative care recommendations in guidelines while also acknowledging that this complex intervention lags behind other evidence-based treatments. There is evidence that palliative care models improve outcomes for patients with cancer with one randomised controlled trial showing mortality benefit10 and numerous studies showing improvements in symptoms and quality of life.10–14 A recent systematic review showed there are no benefits in healthcare resource utilisation.15 In heart failure specifically, a number of small studies have demonstrated some improvements in symptoms of breathlessness using opioids16 and oxygen.17 However, long-term inotrope therapy in advanced heart failure increased mortality.18 Trials assessing holistic palliative care models for heart failure have shown mixed results. A randomised trial in 107 hospitalised patients (51% with CHF) showed no improvements in symptoms or quality of life,19 while a more recent trial of 36 elderly patients with chronic heart failure did report improvements in quality of life and symptoms.20 Generalist palliative care initiated during hospitalisation for patients with heart failure (n=232) improved quality of life, symptoms and depression over the subsequent 3-month follow-up period in the 116 patients randomised to receive the intervention.21 These findings certainly support the need for further trials of interventions addressing specific symptoms and also of the broader palliative care approach. Randomised trials addressing palliative care issues in people with heart failure are underway in several countries and will generate much needed findings.22 ,23 However, the ongoing focus on heart failure may lead to a missed opportunity to extend the provision of good holistic care to all patients with any type of advanced or end-stage heart disease associated with a limited prognosis.
Defining advanced or end-stage heart disease
A number of studies have evaluated ways of identifying patients with cardiac diseases who may be suitable for palliative care24 ,25 with an ongoing debate as to whether the needs of the patient or prognosis should trigger identification. Patients with a limited prognosis who are socially and medically well supported may need limited input from a specialist palliative care team and an approach focusing on proactive planning for the future may be ideally suited to this type of patient. Patients who have complex medical, social, family and spiritual needs are more likely to need specialist palliative care involvement to support ongoing care by the patient's cardiologist and general practitioner (GP). In both instances, prognosis is important but recognising the uncertainty of a patient's prognosis may be just as important and in itself should trigger discussions about planning for the future. Prognosis can be estimated or assessed using heart disease specific26–29 or generic30 ,31 clinical prognostic tools while other tools are sometimes used to assess the need for specialist palliative care.24 ,25 ,32 Natriuretic peptides may have a role in the identification of patients in need of a palliative approach to care. Prognostic scoring tools are reasonably accurate in large populations but given that the illness trajectory of the last year of life for an individual patient with advanced heart disease is so difficult to predict, they should be used to support clinical decision-making and should not replace the clinical judgment of senior clinicians and the wider multidisciplinary team (figure 1).

Defining the ‘end-of-life’ phase and ‘dying phase’ (adapted from Neuberger J, Guthrie C, Aaronvitch D. More care, less pathway: a review of the Liverpool care pathway. Department of Health, Crown Copyright. 2013).
Planning improves end-of-life care for all patients with advanced heart disease
Heart failure is not the only cardiac condition associated with poor prognosis. Many older patients with advanced heart disease are at increased risk of death either because of their cardiac disease or due to comorbidities such as chronic kidney disease, chronic lung disease, cerebrovascular disease or dementia. A common problem is that prognostic uncertainty, lack of knowledge and confidence leads to a failure to initiate and pursue discussions about end-of-life care between cardiologists, patients and their families.33 ,34 While this is improving, there continues to be uncertainty about when to approach patients, whether doing so will remove hope and if a patient's condition might improve following the introduction of additional evidence-based treatment. Cultural change is needed if we are to address these barriers. A positive but realistic approach combines best-evidence cardiology treatments with realistic conversations about deteriorating health and the possibility of a patient dying.
Future care planning
Planning ahead for deteriorating health in the future (future care planning, FCP) has two components that may be offered sequentially or together depending on the patient's circumstances. Advance care planning is a process by which a person chooses to make plans about their future health that will take effect if they deteriorate.
The main elements of Advance care planning include a discussion with the patient and their family about their views on the following aspects of planning ahead:
Nominating a power of attorney or a surrogate decision maker if the patient loses capacity
Any preferences for place of care should they become more unwell, seriously ill or be dying
Preferences for treatment options including withdrawal of life-prolonging treatments (eg, internal cardiac defibrillators (ICDs))
Cardiopulmonary resuscitation and its likely outcome in the person's current or a possible future health state.
An anticipatory care plan is a valuable aid to care coordination for people with long-term conditions who are at risk of deteriorating such as patients with advanced heart disease. It is an individualised, care-record describing the actions, interventions and responses that care providers should consider following an acute deterioration or a sudden change in the patient's condition or home circumstances. In Scotland, the discussion includes seeking patient consent for their anticipatory care plan to be recorded in an electronic key information summary that is shared with emergency care services, primary care and hospitals.35 If the patient is deteriorating and would benefit from more coordinated care from their primary care team, the benefits of being included in a practice palliative care register are often discussed.
Future care planning interviews offer an ideal opportunity to review clinical care and enable patients and families to ask questions about their health problems and its management. They are then invited to talk about their goals and priorities so that these inform planning ahead and talking about advance care planning and/or agreeing with an anticipatory care plan. Previous trials using this type of approach in patients with chronic medical conditions, including heart failure, have indicated that it reduces hospital admissions, healthcare resource utilisation and improves patient satisfaction and quality of life.36 ,37 FCP is appropriate at any stage of a patient's illness (figure 2). The process should establish good communication and shared decision-making with the patient and their family as a fundamental part of ongoing care. FCP can be delivered by a wide range of health professionals as a way of introducing the concept of holistic palliative care to the patient and their family. It seeks to gradually shift the focus from medically orientated treatment outcomes to the personal goals of the patient38 (table 1).
Future care planning : examples of medical versus personal goals
{kind=link}
{kind=link}
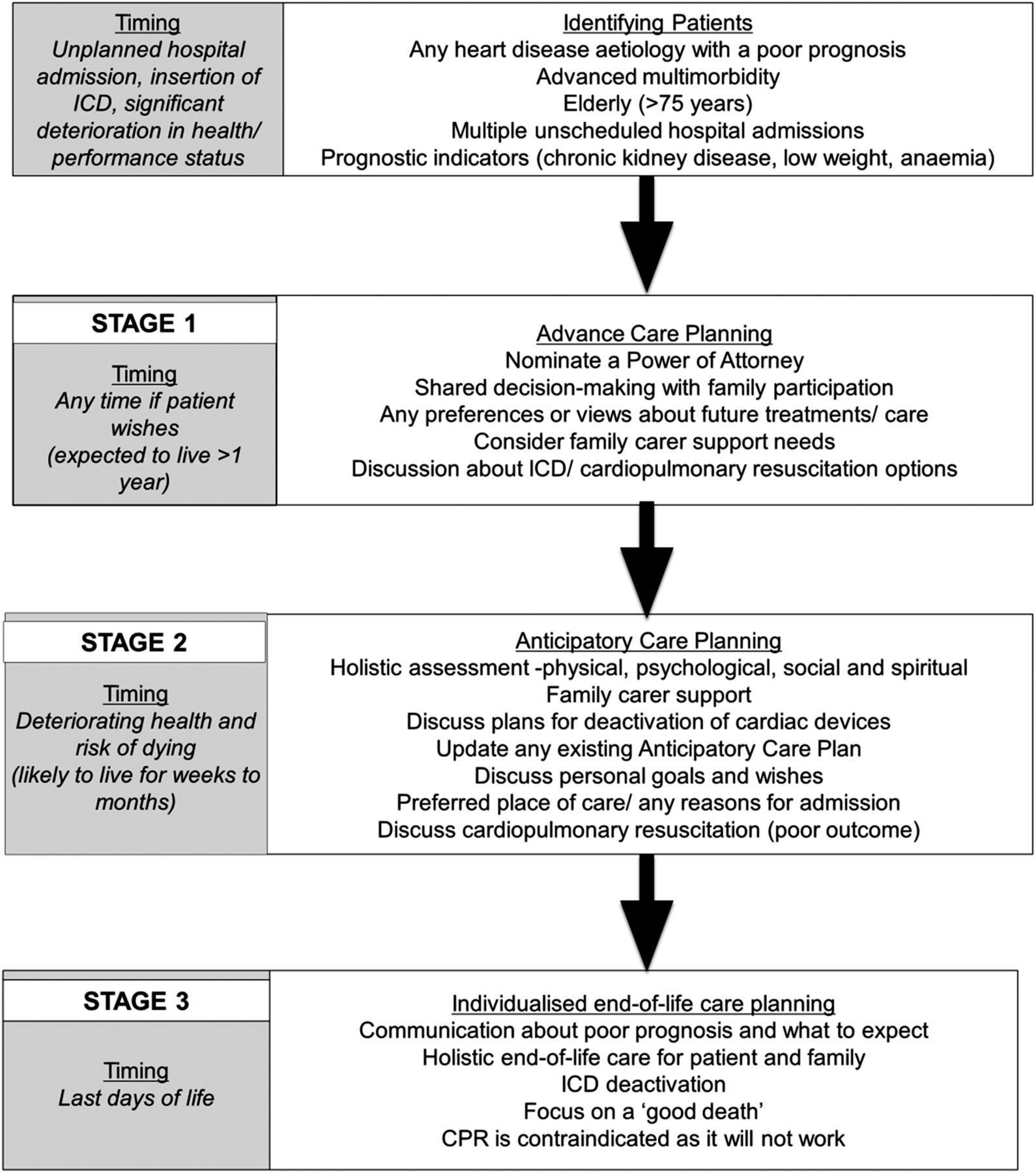
Staged implementation of advance care planning, anticipatory care planning and integrated end-of-life care planning.
When and where should FCP take place?
Discussions about FCP take time and require appropriate training of healthcare staff in order to ensure that interviews are done in a sensitive and effective way. Ideally, the initial interview should be in a quiet non-clinical environment, at a time when the patient is stable and well enough to participate. If it follows an acute event or unplanned hospital admission, the patient and their family can reflect on what could have happened at a time when they are feeling positive that the patient has recovered well. FCP discussions are an essential part of preparing people for ICD implantation to address and plan for the potentially difficult situations that can arise towards the end of life in a patient with an ICD. In addition, the risk of death, even with ICD, remains relatively high at around 7–10% annual mortality in recent trials with optimal medical and device care.39
Which patients with heart disease benefit from FCP?
Until recently much of the emphasis on timely introduction of palliative care has focused on heart failure. There are strong arguments for including people with all forms of advanced heart disease. Older patients with aortic stenosis or myocardial infarction present to acute cardiology services offering an opportunity for assessment of palliative care needs. Patients with advanced congenital heart disease present a specific challenge.
Chronic heart failure
Given that all patients with CHF are at increased mortality risk then some of the elements of FCP are relevant at all disease stages. Even younger patients with dilated cardiomyopathy and mild symptoms who are likely to respond extremely well to drug treatment should be informed about the risks of sudden death. This may change with time if they respond well to treatment and show improvement in left ventricular function. Patients who certainly do need FCP discussions are those with advanced age, multiple comorbidities and limiting symptoms despite optimal tolerated therapy. Patients with low blood pressure, chronic kidney disease and who have had repeated unplanned hospital admissions should certainly have a FCP discussion and should also be carefully assessed for specific palliative care needs. Patients with limiting symptoms who are intolerant of ACE inhibitors and/or β-blockers are by definition at increased risk and should have FCP discussions initiated. Making a link to recent changes in the patient's health, treatment or care needs can help clinicians introduce the topic of planning ahead for deteriorating health.
Valvular heart disease: aortic stenosis
Management of valve disease has changed dramatically in a short time period. Elderly patients with severe aortic stenosis are presenting in increasing numbers and require complex decision-making in relation to surgical and percutaneous cardiac interventions. The Partner B trial clearly showed that, while there are substantial mortality benefits for some patients, the overall outcome is poor with 3-year mortality of 81% in the untreated group and 54% in transcutaneous aortic valve implantation-treated patients.40 A more recently published registry also showed that patients with aortic stenosis who are considered but not accepted for transcutaneous aortic valve implantation also have a very poor prognosis.41 Elderly people with multiple comorbidities including advanced valvular heart disease could benefit greatly from a palliative care approach introduced through timely FCP discussions.42
Coronary heart disease
Elderly patients presenting with acute coronary syndromes are at high risk even after successful coronary intervention.43 For patients over 75 years, the presence of comorbidities such as chronic kidney disease, significant LV dysfunction, CHF, chronic lung disease, anaemia and peripheral vascular disease increase the 1 year mortality risk substantially. In a recent interview study with patients and carers, participants thought that an estimated 1-year mortality risk of 20% or higher should prompt a doctor to discuss what could happen in the future and initiate end-of-life care planning.44 Online prognostic tools such as the GRACE (Global Registry of Acute Coronary Events) score26 or the EPICOR ACS (long-tErm follow-up of antithrombotic management Patterns In acute CORonary syndrome patients) risk calculator27 can help identify these patients.
Congenital heart disease
Increasing numbers of patients surviving into early adulthood with Fontan circulation or Eissenmenger syndrome are reaching end-stage disease with very limited options for further intervention.45 Surveys have indicated very poor implementation of good end-of-life care in these patients46 and there is clearly a need to develop palliative care approaches tailored to the information and support needs of these patients and families.
Who should initiate FCP for people with heart disease?
The general practitioner is ideally placed to start the process of FCP but concerns about judging prognosis in complex patients with advanced heart disease can mean they wait until the patient is very unwell or until the specialist recommends initiating palliative care.47 Many elderly patients are under the care of a number of hospital specialists with numerous clinic appointments. This creates a complex web of specialist-expertise around the patient which has the potential to mask their true functional and clinical status and hinder well-coordinated care delivered by primary care clinicians. When a patient presents to a cardiologist with an acute event such as myocardial infarction or acute heart failure, due to systolic dysfunction or aortic stenosis, this condition is likely to become the principle driver of the patient's prognosis. This is an appropriate time to start FCP discussions and the cardiologist is well placed to discuss the likely course of the illness, deactivation of ICD (if present) and cardiopulmonary resuscitation.
For patients with heart failure, specialist nurses have a key role in discussing FCP. These nurses manage patients with CHF in a holistic and multidisciplinary way, know the patient and their family well and have good relationships with general practitioners. Unfortunately their involvement is commonly targeted at people with systolic heart failure. If we are to improve the delivery of end-of-life care across a broad range of patients with heart disease then this needs to change.
FCP as an ongoing process
Future care plans, whether documented as a paper or electronic record, need to be widely shared and should be dynamic documents. They should reflect the goals and preferences of the patient and represent a process of shared decision making and planning with key professionals. A review interval, dependent on the needs of the patient, is important.
FCP discussions need to take account of how quickly the patient's health is deteriorating and their readiness to consider palliative and end-of-life care (figure 2). If the patient is fairly well and is coping well by living day to day as is often the case in people with a long-term condition such as heart disease, a sensitive discussion about what might be important if they were to deteriorate is often acceptable as in Stage 1. This may result in advance care planning. Should the patient deteriorate further (Stage 2) with a higher risk of deteriorating and dying, such that it would not be a surprise if the patient's life expectancy was less than 1 year, these early discussions can be extended.
If the possibility of dying is raised then the person's concerns and goals should be explored to inform more specific discussions about supportive and palliative care including developing an individual anticipatory care plan. In the last days of life (stage 3), the focus of discussions will be on what happens when someone is dying and planning for good care of the patient and family at this time.48
Future research
There is a need for research to assess the best ways to introduce FCP discussions with all patients who have advanced heart disease and optimal processes for information sharing and care coordination to deliver it effectively. Electronic records provide an ideal system for sharing key information about future care plans but need to be accessed and used by professionals in primary and secondary care and regularly updated. Testing electronic record solutions for information sharing and information reconciliation as the patient moves between care settings is essential. Trials in cancer care suggest that informed approaches to FCP discussions with patients and families are acceptable and effective but further studies are need to confirm the same outcomes in people with other conditions and illness trajectories such as heart disease.
A phase 2 randomised controlled trial of an FCP intervention around the time of discharge after an acute cardiac unit admission with patients who have advanced heart disease will be completed shortly.44 There are a number of challenges in the design and delivery of larger trials. Many acute hospital and primary care services in the UK are introducing some form of FCP on an empirical basis, although few have done so systematically. In Scotland, the electronic key information summary35 provides a unique opportunity to deliver FCP as a consistent process for all patients with advanced heart disease. Other print and electronic systems are in development in other parts of the UK and internationally that may have a similar potential. Barriers to engagement with FCP are well documented and need to be considered and addressed.
Conclusions
FCP, combining advance and anticipatory care planning in patients with heart disease who have a poor prognosis represents a first step towards a broader view of palliative care as integral to the care of all patients with deteriorating health who are at risk of dying. As a process it provides a unique opportunity to create cultural change within the wider cardiology community by overcoming some of the barriers associated with the term ‘palliative care’. Systematic approaches to FCP could result in a holistic, palliative care approach becoming the norm towards the end of life that is initiated and largely provided by their cardiologists and GP, with only a small proportion with complex needs requiring additional input from palliative care specialists. One of the challenges of making palliative care accessible to all patients with advanced heart disease is closing the gap in understanding between cardiologists, palliative care specialists and general practitioners. A series of randomised clinical trials of sufficient size and power are of key importance.
References
Footnotes
Contributors MAD drafted the document, SAM and KJB edited and added comments. All authors contributed to the concepts, ideas and knowledge within the article.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.