Article Text

Abstract
Background Life course exposure to violence may lead to disability in old age. We examine associations and pathways between life course violence and mobility disability in older participants of the International Mobility in Aging Study (IMIAS).
Methods A cross-sectional study using IMIAS 2012 baseline. Men and women aged 65–74 years were recruited at 5 cities (n=1995): Kingston and Saint-Hyacinthe (Canada), Tirana (Albania), Manizales (Colombia) and Natal (Brazil). Mobility was assessed by the Short Physical Performance Battery (SPPB) and by 2 questions on difficulty in walking and climbing stairs. Childhood physical abuse history and the HITS instrument were used to gather information on childhood exposure to violence and violence by intimate partners or family members. Multivariate logistic regression and mediation analysis models were constructed to explore the significance of direct and indirect effects of violence on mobility. Interaction effects of gender on violence and on each of the mediators were tested.
Results Experiences of physical violence at any point of life were associated with mobility disability (defined as SPPB<8 or limitation in walking/climbing stairs) while psychological violence was not. Chronic conditions, C reactive protein, physical activity and depression mediated the effect of childhood exposure to violence on both mobility outcomes. Chronic conditions and depression were pathways between family and partner violence and both mobility outcomes. Physical activity was a significant pathway linking family violence to mobility. Gender interactions were not significant.
Conclusions Our results provide evidence for the detrimental effects of life course exposure to violence on mobility in later life.
- EPIDEMIOLOGY
- PUBLIC HEALTH
- SOCIAL MEDICINE
- GERIATRIC MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Novel research question on the associations between domestic violence experienced throughout the life course and mobility disability in old age.
Common and validated methodology applied to five samples of community-dwelling older adults from diverse populations which provide a wide range of exposures to domestic violence and physical function.
Assessment tools for domestic violence from childhood to old age were standardised and validated by results from previous research on these five populations.
Information about severity and duration of violence events was lacking, and consequently we were unable to examine dose-dependent relationships.
Mediation analyses were based on cross-sectional data and the lack of temporal sequence for some potential mediators, such as depression, could lead to underestimation of the direct effect of violence on mobility if mobility disability leads to depression.
Introduction
Exposure to domestic violence (DV) at any point in the life course is associated with poor health.1 DV experienced in childhood or during adulthood is associated with low self-rated health,2 depression,3 ,4 alcohol addiction and obesity,5 increased risks for cancer,6 osteoarthritis,7 chronic conditions,8 and acute myocardial infarction.9 The association between DV and poor general health, musculoskeletal pain, headache, stomach problems, allergy, anxiety, sleeping problems, stress and suicidal thoughts has also been well documented.10–13
Mobility, defined as the ability to move oneself independently or by using assistive devices or transportation within environments,14 is a major predictor of morbidity and mortality in older adults.15 ,16 The prevalence rates of mobility disability show huge variations from 13.3% in men aged 65–69 years to 83.3% in women aged 90–95 years.17
The embodiment theory proposes that our bodies are biological organisms and social beings concurrently and that, through various mechanisms, social adversities can integrate to the body causing direct biological damages.18 The life course approach examines long-term effects of physical and social exposures and their interactions on health conditions.19 A variety of models have been suggested based on the life course approach and the impact of violence on health can be best explained by the chains of risk model. According to this, a series of exposures to adverse conditions are connected to each other, increasing the risk of illness because exposure to a given risk factor leads to another more proximal risk factor.20 So life course experiences of violence may lead to poor health behaviours, chronic physical conditions and depression, which are risk factors for mobility disability21 ,22 and could be pathways whereby violence is embodied into biology.
Few studies have analysed long-term effects of life course exposure to violence on the functional health of older adults.4 ,23 ,24 Sousa et al24 found that older adults who reported social adversities in childhood (including being physically abused before 15 years of age) were three times more likely to have low physical performance in the Short Physical Performance Battery (SPPB). Another study reported that elderly women who experienced intimate partner violence were more likely to report a disability due to chronic pain and mental illness.25 Despite the known excess prevalence of mobility disability and experience of violence among women, to the best of our knowledge, no study has directly addressed the gender differences in mobility using violence as the main exposure. Furthermore, the pathways through which exposure to early childhood adversities may affect mobility later in life and whether these pathways are different in women and men have rarely been explored.23 ,26 We hypothesised that experience of DV during the life course is a risk factor for mobility disability in older ages, and that this association might be partly explained by biological (chronic conditions, metabolic syndrome, inflammation), behavioural (obesity, alcohol and physical activity) and psychological (depression and cognition) pathways.
Our objectives were: (1) to examine associations between the experiences of childhood abuse and DV throughout the life course and mobility disability in old age; (2) to explore the significance of possible pathways for these associations; and (3) to examine differences between men and women in these associations.
Methods
Settings and study population
Data were obtained from the 2012 baseline survey of the International Mobility in Aging Study (IMIAS),27 a population-based longitudinal study conducted in five cities: Tirana (Albania), Natal (Brazil), Manizales (Colombia), Kingston and Saint-Hyacinthe (Canada). These cities represent different settings in terms of socioeconomic and environmental characteristics.28 Furthermore, levels of human development index, gender equality29 and social and DV vary considerably across these sites.30 ,31
The study population is composed of community-dwelling older adults between 65 and 74 years of age. The sample was stratified by sex to recruit ∼200 men and 200 women at each site, with a total sample size of 1995 at the five sites. The sample size at each site allows for a comparison of baseline mobility disability prevalence of men and women assuming a prevalence ratio of 1.8, a type I error of 0.05 and a power of 0.80.
Sampling strategy
Participants were recruited through neighbourhood primary care centre registers at Tirana, Manizales and Natal. At these sites, random samples of elderly people registered at the health centres were drawn and participants were directly invited to participate in the study through home visits. Since Albania and Brazil have universal healthcare systems, more than 90% of the population in the 65–74 age range are registered at a neighbourhood health centre. In Manizales, about 70% of the people of interest are registered in the Public Health Insurance programme. In Tirana, Manizales and Natal, response rates were higher than 90%. Owing to ethical requirements, the sampling strategy in Canadian sites was different; participants received a letter from their primary care doctors inviting them to book an appointment for a home visit. Only 30% of these people contacted us; however, out of these, about 95% agreed to participate, resulting in overall response rates of 28%. We excluded those with four or more errors in the orientation scale of the Leganes Cognitive Test (LCT),32 indicating severe cognitive impairment. Few people were excluded from the study, ranging from zero in Kingston to five in Natal.
Data collection
Interviewers at each site were trained in administrating computer-assisted questionnaires and in performing video-based and direct measurements using standard and validated protocols.33 Manuals of procedures were available in the study languages: Albanian, Spanish, Portuguese, English and French; they are available on request.
Variables
Lower extremity functioning
It was assessed by the SPPB,15 which includes three timed tests of lower body function: a hierarchical test of standing balance, a 4 m walk and five repeated chair stands. A summary performance score was obtained by adding the scores of each individual SPPB component test (range 0–12), with higher scores indicating better lower body function. An SPPB score lower than 8 was indicative of poor physical performance.24 Self-reported mobility disability was defined by two questions: ‘Do you have difficulties climbing 10 stairs without resting?’ and ‘Do you have difficulties walking 400 m?’ People who reported difficulty in walking 400 m and/or climbing 10 stairs were defined as having mobility disability.21
Childhood abuse and DV
Participants were asked: ‘During the first 15 years of your life, were you ever physically abused by someone close to you?’ A positive response was defined as the experience of childhood physical abuse (CPA). To assess DV, we used the HITS instrument.34 We asked if an intimate partner/family member had ‘Hurt; Insulted; Threatened or Screamed at you’. The Hurt item of HITS aims at identifying physical violence and the remaining items assess psychological violence. Separate questions were asked for ‘partner’ and ‘family members’ and repeated for ‘any’ point in the life and for ‘the preceding 6 months’. Response options were: never, rarely, sometimes, fairly often, and frequently and then further categorised into never and ever (rarely to frequently). Using these three questions, we created five variables, one for the unique experience of CPA, and four reflecting exposure to ‘physical’ or ‘psychological’ violence by ‘partner’ or by ‘other family members’. Participants were then classified into four groups: (1) never experienced violence; (2) experienced violence in their life but not in the past 6 months; (3) experienced violence in their life and in the past 6 months; and (4) experienced violence only in the past 6 months but never previously. Figure 1 illustrates how violence variables were created.
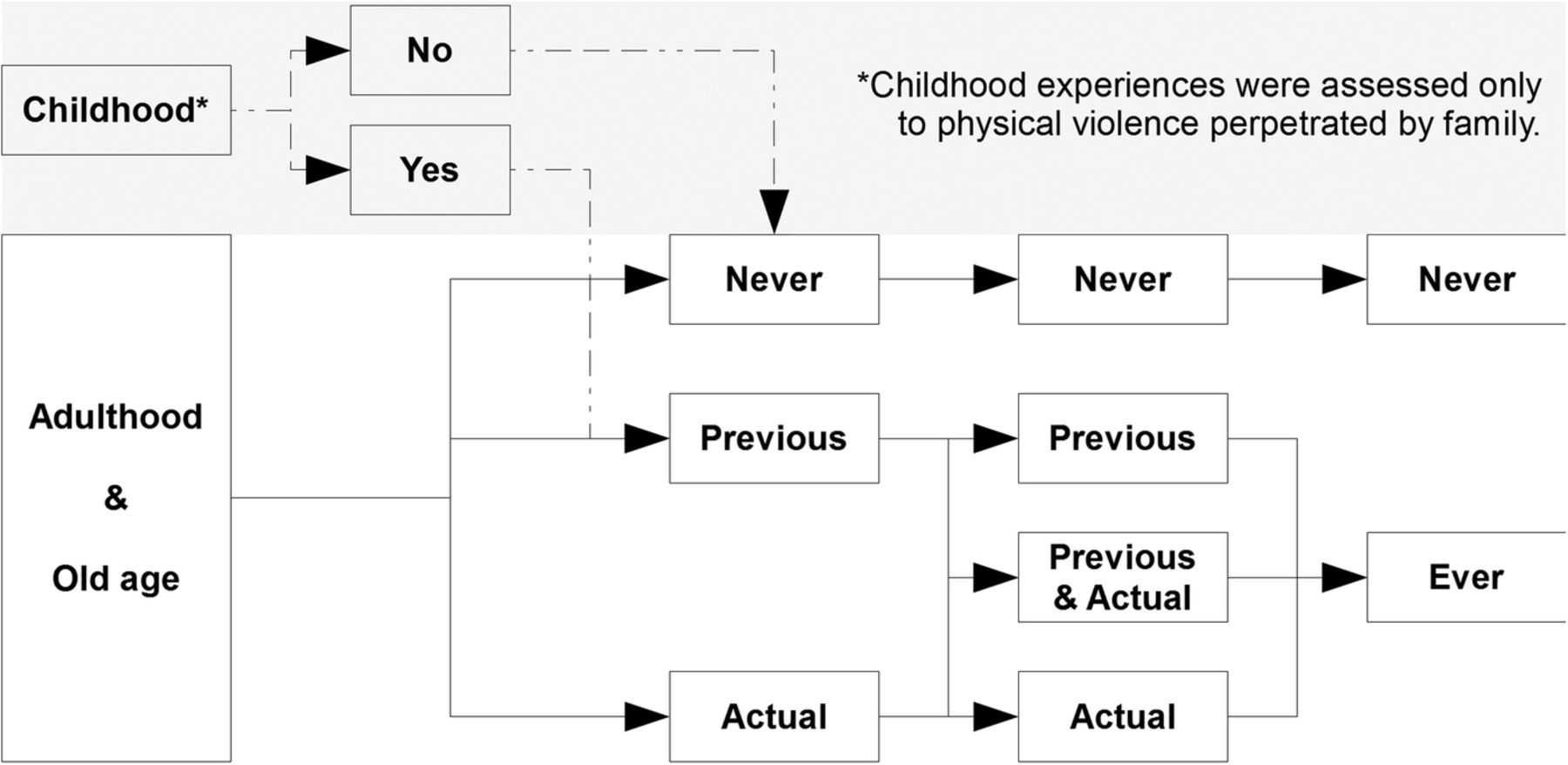
Strategy to create domestic violence variables (both physical and psychological) perpetrated by partner or other family members in a life course perspective.
Potential pathways
Chronic conditions: participants stated if a physician or nurse had ever told them that they have high blood pressure, diabetes, cancer, lung disease, heart disease, neurological problems or rheumatic diseases.
Metabolic syndrome was assessed using the National Cholesterol Education Program's Adult Treatment Panel III.35
Inflammation was assessed by ultrasensitive C reactive protein (CRP) enzyme-linked immunoabsorbent assays. Serum from Saint-Hyacinthe and Kingston was analysed at Kingston General Hospital (Queen's University), serum from Manizales at the Caldas University Hospital and from Natal at a certified local laboratory. CRP assessment was not available at Tirana.
Health behaviours: first, we used animated videos to ask how many days the person walked during a typical week and the approximate duration of the walk. We then calculated the number of minutes walked in a usual day. Participants' alcohol consumption was estimated from the reported average number of drinks per day.
Body mass index (kg/m2): height was measured without shoes, using a stadiometer. Weight was measured with an electronic scale after removal of outer garments and footwear.
Cognitive function was measured by LCT,36 with scores between 0 and 32. Depressive symptoms were assessed by the Center for Epidemiologic Studies Depression scale (CES-D), with scores between 0 and 60.37
Potential confounders
Childhood economic status was inquired by a single question: ‘During the majority of the first 15 years of your life, what was the economic situation of your family?’ with three categories of response: good, average and poor.
Income sufficiency was assessed by the question: To what extent is your income sufficient to cover basic needs? Possible answers were: very sufficient, sufficient and insufficient. Level of education was assessed by years of schooling.
Statistical analyses
Bivariate associations between mobility outcomes and exposure to violence and potential confounders were first assessed by χ2 and analysis of variance tests. We estimated associations between life course violence exposure and mobility disability by fitting logistic models, adjusting for research site, age, sex, childhood economic status and education. Since the city a person lives in might affect both mobility and exposure to violence, we considered ‘city’ as a control variable. Interactions between violence variables and gender on mobility outcomes were also tested.
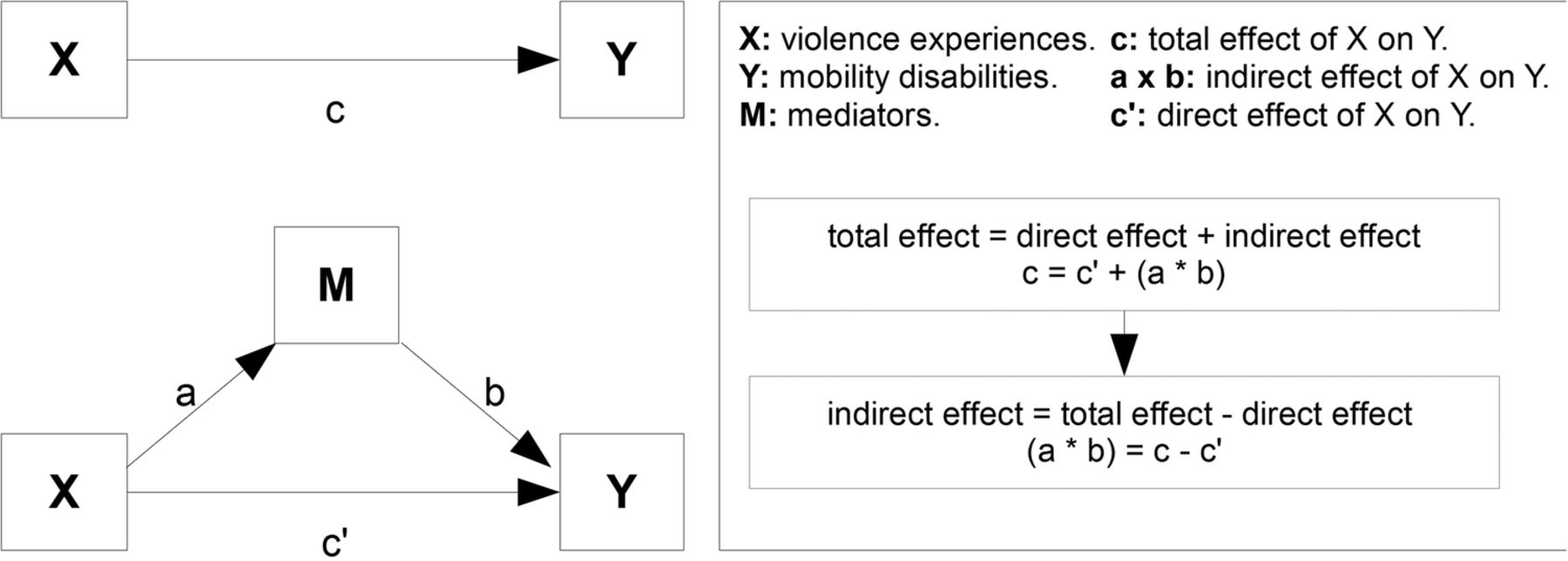
For mediation analyses, the strategy proposed by Preacher and Hayes38 (figure 2) was adopted to evaluate the possible pathways (indirect effects). According to this approach, testing mediation is based on the following: (1) there exists an effect to be mediated (c≠0); and (2) the indirect effect (a×b) be statistically significant in the direction predicted by the mediation hypothesis, where a is a risk factor of X (violence) on M (possible mediators), b is a risk factor of M on Y (mobility disability) and c is the direct effect (X as a risk factor to Y). All potential pathways were used as continuous variables in mediation analyses. To avoid collinearity problems associated with simultaneous assessment of parallel pathways that can attenuate indirect effects, we analysed each pathway separately, adjusting for the same covariates we used in logistic models. To evaluate the significance of indirect effects, we used a non-parametric test to estimate 95% CIs (10000 bootstrapping samples). Multiplicative interactions between gender and each mediator were tested. Mediation analysis was performed using the Process Macros (http://www.afhayes.com/) for SPSS (IBM Corp, Armonk, New York, USA).
{kind=link}
{kind=link}
Strategy to analyse mediating factors between violence experiences and mobility disabilities, using the model proposed by Preacher and Hayes.38
Results
Our sample was composed by 1995 older adults, 1040 women and 955 men. One hundred and twenty-two participants never had a partner in their life, and therefore the sample size for the exposure of partner violence was 1873. Owing to missing data on blood, analyses of metabolic syndrome and CRP were restricted to 1728 and 1060 participants, respectively.
Research sites were different in terms of education and income levels, and women were over-represented among socially disadvantaged groups. In the pooled data and all sites except Kingston, women had more self-reported mobility problems. There was no statistical difference in SPPB scores between Canadian men and women. Canadian participants presented better mobility outcomes (table 1).
Distribution of sociodemographic factors and mobility measures by sites
Psychological violence either perpetrated by partner or family was more frequent than physical violence (table 2). Compared with men, women were more often victims of all types of violence.
Experiences of violence in life course by site and gender
According to our adjusted regression models, experiences of CPA and adult physical violence either by family or partner were related to mobility disability, whereas after adjustment for age, sex, childhood socioeconomic status, education and research site, psychological violence did not increase the relative odds of mobility decline (table 3). Those exposed to physical violence by an intimate partner showed 40% greater odds of mobility limitations and had 63% higher odds of scoring under 8 on the SPPB, while physical violence by partner was associated only with an SPPB score <8. CPA was associated with both mobility outcomes. Gender was not an effect modifier for the relationships between any form of violence and mobility.
Associations between violence and mobility measures
Since there was no significant relationship between psychological violence and mobility measures, mediation analyses were only performed for examining pathways between physical violence and mobility measures. Significant indirect effects of chronic conditions, CRP, physical activity and depression suggest that some impacts of childhood abuse experiences on violence might have been mediated through these pathways (table 4). Interpretation of significant continuous mediators for a discrete outcome is not straightforward but can be explained as follows. Consider two older adults who are identical in all factors but one was exposed to CPA while the other was not. The model estimates a total effect of 0.38 and a significant chronic condition indirect effect of 0.125. These results indicate that the two exposed and unexposed participants differ by 0.38 SDs in the log odds of mobility disability on average (total effect), from which 0.125 SDs on average would be attributable to the effect of CPA on chronic conditions, which in turn affect mobility. The remaining effect of CPA on mobility would be independent of the impact of chronic conditions. Chronic conditions and depression were significant pathways between physical violence and both mobility measures. We identified physical activity as an additional pathway between family physical violence and mobility with an indirect effect of 0.149 on mobility limitations and of 0.183 on SPPB (table 4). None of the gender×mediator interaction effects were significant.
Total, direct and indirect effects of physical violence in the life course on mobility measures using the Preacher and Hayes approach
Discussion
We examined the associations between experiences of violence in the life course and mobility disabilities in older adults, and explored possible pathways and differences between men and women in those associations in five international settings. We found that physical violence (at childhood, by family or partner) was consistently associated with mobility disability. Furthermore, we found that physical violence operates through physical health (number of chronic conditions), health behaviours (physical activity) and mental health (depression) pathways. Finally, we observed that women experienced more mobility problems and more exposure to violence, but the association between physical violence and mobility disability was not different between women and men.
The detrimental impact of violence during adulthood on a variety of health conditions,4 ,10 ,11 ,13 ,23 ,39 and the positive correlations between good mobility and health are established16 ,17 ,40 and consistent with findings of this study. However, to the best of our knowledge, only one study examined associations between childhood adversities (including physical abuse) and mobility disability24 and there exists no study exploring possible pathways linking life course violence and mobility disability. Our results were consistent with others that showed a strong link between life course adversities and adverse health outcomes other than mobility disability in older adults.4 ,10 ,39 The lack of a direct effect of psychological violence on mobility disability may be related to the fact that those experiences were minor in severity or that most of their effects are related to depression (data not shown), but this remains to be explored in other contexts and with violence measurement tools that include severity and timing.
Our findings supported that the explored behaviours and physical and mental health pathways may in fact link CPA to mobility disability, both using a self-reported measure and an objective measure of physical performance. Observed relationships between CPA and inflammation, depression and poor physical activity are consistent with previous reports.3 ,4 ,6 ,41 A recent study showed associations between childhood trauma (including being physically abused) and increased inflammatory genetic transcription later in life41 as embodying traumatic experiences. Our findings also concur with Min et al8 that partner and family violence are related to greater likelihood of chronic conditions later in life. It has been suggested that childhood violence may have long-standing effects on older adults' mental health,4 and we further showed that violence across the life course can influence mobility through mental health. Despite observed associations between violence measures and metabolic syndrome, obesity, alcohol consumption, and cognition and also associations between these factors and mobility, they did not link violence with mobility in our study. Future studies should verify these results as pathways may differ across populations.
Some methodological limitations need to be addressed. First, information about severity and duration of violence events was lacking, and consequently we were unable to examine dose-dependent relationships. Second, the sample size was relatively small for research on site-specific effects; however, we adjusted for site as a confounder in order to account for differences across sites. Third, the generalisability of this study is limited to the studied populations since the research cities are not representative of the countries where they are located. Finally, we cannot be certain of temporality of the associations for physical violence and psychological violence by partner and family as our analysis was based on cross-sectional data. However, the exposure to childhood violence happened in the past and the majority of cases of physical violence have not occurred in the past 6 months, which suggests that violence may precede many of the pathways. Finally, all violence data were collected retrospectively and could lead to misclassification if older adults had forgotten or would not wish to recognise abuse. Retrospective data on exposures have been shown to be reliable in some previous studies on childhood economic position42 but not on childhood or intimate partner violence (IPV) violence. As previously shown comparing historical data with retrospectively collected data, when misclassification exists, it is non-differential in relation to the health outcome and can produce underestimations of the measures of association.43 The main strength of this study is that it asks an innovative research question and is the first study of pathways between violence and mobility disability in five distinct social settings. In addition, the consistency of the associations is strengthened by the similarity of results obtained using both a self-reported outcome and an objective measure of physical performance.
Consequences of violence go beyond its immediate burden of injuries and lives lost. Our results provide evidence on the detrimental effects in the trajectory of life and impacts on physical function in later life.
Acknowledgments
This manuscript was prepared by the research group of International Mobility in Aging Study (IMIAS) studying the decline in mobility in older populations in four countries (Canada, Colombia, Albania and Brazil). IMIAS has financial support from The Canadian Institutes of Health Research (project number AAM108751) and participating universities: University of Montreal-Quebec, Canada; Universidade Federal do Rio Grande do Norte-Brazil, Queens University-Kingston, Canada; University of Caldas Manizales, Colombia and Instituti i Shendetit Publik—Tirana, Albania. The first author was also supported by the CNPq (National Council for Scientific and Technological Development—Brazil—Process project number 247290/2013-0). Finally, the authors thank Dr Kevin M Sherin (ksherin@yahoo.com) for permission to use the HITS tool.
References
Footnotes
Contributors DTG and ROG conceptualised the research questions, contributed to the study design and data analyses and drafted the manuscript. AV and BEA participated in the analyses of the data and interpretation of the study results and revised the manuscript. CLC participated in the design of the study and revised the manuscript. MVZ and JMG participated in the design of the study and hypothesis formulation and revised the manuscript. All authors read and approved the final manuscript.
Funding Canadian Institutes of Health Research, Project number AAM108751 and Conselho Nacional de Desenvolvimento Científico e Tecnológico/Brazil, Project Number 247290/2013-0.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Queens University and Universidade Federal do Rio Grande do Norte.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are not accessible online due to requirements of the Ethical Review Board of Queens University. However, all data are available on request from MVZ, principal investigator of the IMIAS by email: maria.victoria.zunzunegui@umontreal.ca.