Article Text

Abstract
Introduction Fetal alcohol spectrum disorder (FASD) is a significant public health concern. To prevent FASD, factors that place women at risk for giving birth to children with FASD must be investigated; however, there are little data in this area. This paper describes the development of the Manitoba mothers and FASD study, a retrospective cohort of mothers whose children were diagnosed with FASD, generated to investigate: (1) risk factors associated with giving birth to children with FASD; (2) maternal physical and health outcomes, as well as the usage of health and social services.
Methods The study population will be identified by linking children diagnosed with FASD from a provincially centralised FASD assessment clinic (from 31 March 1999 to 31 March 2012) to their birth mothers using de-identified administrative health data housed at the Manitoba Centre for Health Policy. Preliminary analysis has identified over 700 mothers, which is the largest sample size in this field to date. A comparison cohort of women with children who did not have an FASD diagnosis matched on the region of residence, date of birth of child with FASD and socioeconomic status will be generated to compare exposures and outcomes. Potential demographic, socioeconomic, family history, and physical and mental health risk factors will be investigated by linking a range of health and social databases, furthering insight into the root causes of drinking during pregnancy. The longitudinal data will allow us to document the usage patterns of healthcare and social services throughout significant periods in these women's lives to identify opportunities for prevention.
Ethics and dissemination Ethical approval has been obtained by the University of Manitoba's Health Research Ethics Board and the Manitoba Health Information Privacy Committee. Dissemination of study results will include engagement of stakeholders and policymakers through presentations and reports for policymakers, in parallel with scientific papers.
- Fetal alcohol spectrum disorder
- prenatal alcohol use
- Maternal risk factors
- administrative health data
- study protocol
- drinking during pregnancy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Fetal alcohol spectrum disorder
- prenatal alcohol use
- Maternal risk factors
- administrative health data
- study protocol
- drinking during pregnancy
Strengths and limitations of this study
Through the use of linked clinical and administrative data, the Manitoba Centre for Healthy Policy Data Repository allows the generation of the largest population-based sample of all women whose children were diagnosed with fetal alcohol spectrum disorder (FASD).
The Manitoba FASD Centre offers a valid and reliable clinical diagnosis of FASD, and by linking these records to the birth mothers, we can be certain that women in this sample have given birth to children with FASD.
Administrative data eliminate re-call bias and offer accurate information that can be isolated in critical periods of time throughout a study participant's lifespan.
The study is subject to the limitations of administrative data and is reliant on the accuracy of data submitted by the organisations that deliver services.
While we have taken great care in excluding all mothers with possible prenatal alcohol exposure and children with a diagnosis of FASD, we cannot be certain that there are no women in our comparison group who do not have un-reported prenatal alcohol use or children with undiagnosed FASD.
Background
The prevention of fetal alcohol spectrum disorder (FASD) is a significant public health concern. In North America, over 10% of women report alcohol consumption during pregnancy.1 Prenatal alcohol use places infants at risk for FASD, an umbrella term comprising a range of effects associated with prenatal alcohol exposure.2 FASD has been recognised as the leading preventable cause of mental retardation in North America, highlighting FASD and prenatal alcohol consumption as substantial public health issues.2 Individuals with FASD experience myriad symptoms, including facial dysmorphology, growth restriction, central nervous system and neurodevelopmental abnormalities, as well as behavioural, emotional and social difficulties.2 ,3 Over the past decade, international FASD prevalence estimates have ranged from 2% to 5%4 in the general population and up to 23.3% in high-risk populations.5–14
FASD has been referred to as the world's only entirely preventable birth defect. Since the identification of fetal alcohol syndrome (FAS) in the 1970s, women who drink during pregnancy have been stigmatised and held responsible for causing this ‘preventable’ condition.15 The notion that this disorder can be prevented is rooted in the theory that the exposure can be easily eliminated.15 However, this response does not account for the many complex factors that influence women to engage in prenatal alcohol consumption, such as poverty, poor housing, trauma, physical and sexual abuse, mental disorders, lack of education and substance dependence.16 ,17 The use of alcohol during pregnancy cannot be separated from these issues in the lives of women, and from other potentially harmful behaviours such as poor health practices, poor nutrition and the use of other harmful substances.16 ,17 Only through identifying the demographic, social and economic factors that place women at risk for alcohol consumption during pregnancy can we obtain insight into the root causes of this behaviour and identify target points for prevention and support.
What is known about women whose children are diagnosed with FASD?
The WHO's global strategy to reduce the harmful use of alcohol highlights the importance of identification and prevention of the use of alcohol among pregnant women.18 Although a growing body of literature investigating prenatal alcohol use exists, there are limited data focusing on the birth mothers of children who are diagnosed with FASD.
A systematic literature review conducted in 2013 summarised studies that identified maternal factors associated with the development of FASD.19 The review identified 15 studies that were conducted throughout the world, including the USA, South Africa and New Zealand.9 ,20–29 The included studies summarised demographic factors, family and social factors, psychiatric and neuropsychological factors, and patterns of alcohol consumption, and identified the following maternal factors associated with the development of FASD: older age, lower educational level, lower socioeconomic status (SES), unemployment during pregnancy, rural residence, higher parity and gravidity, family relatives with alcohol abuse issues, mental disorders, psychological distress, physical and sexual abuse, use of tobacco and illicit drugs during pregnancy, and a more severe pattern of alcohol consumption in general and in pregnancy, including more binge drinking.19
What are the evidence gaps in the current literature?
While these studies have laid the groundwork for investigating factors associated with giving birth to children with FASD, they have several important limitations that may preclude them from informing FASD prevention strategies in North America:
Limited generalisability: first, there are no Canadian studies and few studies from the USA that were conducted at a population level. The majority of studies are from South Africa and Italy, and many focus on women who are from high-risk populations, such as indigenous populations.7 ,23 ,24 ,30 Owing to differences in population demographics and cultural norms, caution should be taken when extrapolating these results to the general North American population.
Small sample sizes: previous studies have utilised small samples that range from 8 to 250 birth mothers.20 ,22–25 ,30 These small sample sizes may be a function of the complexity of diagnosing children with FASD, particularly because alcohol consumption during pregnancy is underreported.4 ,10 However, these sample sizes limit the generalisability of results, have limited power to detect significant differences among comparison groups and limit the ability to conduct powerful multivariate analyses.
Recall bias: the majority of studies in this area are also limited by recall bias from self-report survey and interview data.11 ,20 ,31–33 There are many factors that affect the validity of self-report data in alcohol use during pregnancy, including severity of alcohol use disorder, issues of confidentiality, stigmatisation, fear of disclosure, fear of involvement of child welfare services, mental disorders and denial of alcohol use as a problem.25 ,32 Moreover, the accuracy of the information provided by self-reports is questionable, especially during periods of high alcohol consumption, which affects memory and judgement.34
Limited data on diagnosed physical and mental health disorders: no previous studies have documented clinically diagnosed physical and mental health disorders in women who give birth to children with FASD using reliable and validated clinical data, highlighting an important gap in the literature. There is a strong association with mental health disorders and alcohol consumption35–40 and investigating this relationship in women who give birth to children with FASD is extremely important for the advocacy of effective support and prevention strategies.
Limited data on service utilisation: a few studies have investigated prenatal care in this population through self-report data and have found that these women receive fewer prenatal visits compared to women in the general population, and generally begin prenatal care later in their pregnancies.23 ,24 ,30 ,41 However, these results are limited by recall bias and do not report any other health or social services use.
How can administrative health and social data help address evidence gaps?
The Manitoba mothers and FASD study (MBMomsFASD) is a data linkage project that will generate a retrospective cohort of all mothers who gave birth to children diagnosed with FASD in Manitoba, Canada. In partnership with the Manitoba FASD Centre (a provincially centralised FASD assessment and diagnostic clinic) and the Manitoba Centre for Healthy Policy (MCHP) (a population health research unit within the University of Manitoba, Canada), we will analyse explanatory variables associated with giving birth to children with FASD by analysing potential risk factors that are present before giving birth to a child with FASD (eg, SES, marital status, prenatal psychological distress, inadequate prenatal care), as well as maternal outcomes after the child with FASD is born (eg, postpartum psychological distress, suicide attempts and completion).
This study will make important contributions to the literature by filling existing gaps and addressing key methodological limitations identified in previous studies by using linked administrative health, social and education data housed at the MCHP. The MCHP Data Repository (herein referred to as the ‘Repository’) is one of the world's most comprehensive collections of population-based administrative databases. These data are a powerful tool to investigate factors that promote the health of populations, as well as to understand the usage of healthcare services and social programmes of populations and specific groups.42 The Repository consists of population-wide administrative data from health and social service agencies, education institutions and Canadian Census,42–44 which allow the investigation of outcomes from multiple domains in a cohort of individuals.42–44 This approach allows for an enhanced assessment of overall well-being and the impact of the multiple social determinants of health. This type of holistic investigation is particularly relevant to women who give birth to children with FASD. Women who drink during pregnancy often have histories that are rooted in abuse, poverty, other substance abuse and mental and/or physical illness.17 ,45 ,46 Owing to the wealth of social and health data within the Repository, these data are an ideal source to investigate potential factors associated with prenatal alcohol consumption that results in the birth of a child with FASD. Administrative data are also ideal to investigate the usage of health and social systems among a population for any length of time or specified years.42–44 ,47 ,48 We will document the usage of health and social systems among women whose children have been diagnosed with FASD to provide insight into how they navigate the health, social and education systems.
Research questions
What are the differences in: (a) demographic characteristics; (b) socioeconomic characteristics; (c) family characteristics; (d) psychiatric morbidity; (e) suicide behaviour; (f) physical morbidities, and (g) use of health and social services among women whose children have a clinical diagnosis of FASD compared to women whose children do not have a diagnosis of FASD?
What demographic, socioeconomic, family, mental and physical health characteristics are associated/predictive with giving birth to children with FASD compared to not giving birth to children with FASD?
Methods and analysis
Description of data sources
Records from the following data sources will be requested and linked together for analyses:
Manitoba FASD Centre: This data set includes information on all children assessed at the clinic from 31 March 1999 to 31 March 2012 and consists of children who have received a diagnosis of FASD, children who have been assessed but do not meet the criteria for FASD and those who have received a deferred status, meaning that they will be assessed at a later time (eg, when children are older, symptoms are more apparent). The clinic uses the Canadian diagnostic guidelines developed by Chudley et al,2 and the updated guidelines published by Cook et al.49 These guidelines include all alcohol-related disabilities that are included under the FASD definition: alcohol-related neurodevelopmental disorder (ARND), alcohol-related birth defects, FAS and partial FAS (pFAS). Diagnosis of FASD is conducted by a multidisciplinary team and FASD diagnosis typically includes screening and referral; physical examination and differential diagnosis; neurobehavioral assessment; and treatment and follow-up.2
MCHP Repository: The following databases will be utilised in this study:
The population registry: a registry maintained by the provincial department of health of all Manitobans eligible to receive health services since 1970 (updated semiannually) and includes demographic information and 6-digit residential postal code;
Canada census information: social data based on the Statistics Canada Population Census. These data were used to determine area-level income, with the Manitoba population divided into quintiles according to average area-level household income, composed of five income groupings with Q1 being the lowest and Q5 being the highest income quintile;
Employment and income assistance: data from the Social Assistance Management Information Network that provide information on Manitoba residents who receive provincial employment and income assistance, a programme that provides financial assistance for meeting the basic needs of living.
Education data: education data maintained by the provincial department of education that provides information on enrolment, marks, and high school completion, and special funding. Special education funding is provided to children with severe to profound disabilities.
Babies first/families first screening programme data: data collected as part of a universal screening programme conducted by Healthy Child Manitoba. The screen is filled out by Public Health Nurses on all families with newborns in Manitoba and captures data on biological, social and demographic risk factors, including alcohol use during pregnancy.
Healthy baby prenatal benefit: data from the Healthy Baby programme, which provides an income supplement to help women meet nutritional needs during pregnancy and connects women to programmes and resources in their area;
InSight program data: data from an outreach program where mentors provide intensive support to substance-using women who are pregnant or have recently had a baby. This data set includes information on women who have prenatal alcohol use;
Justice system data: an incident tracking system maintained by the provincial department of justice. These data include information on incidents, charges and involvements (eg, witness, accused, victim) in the justice system in Manitoba;
Hospital discharge abstracts: consisting of all hospitalisations in Manitoba, including up to 16 ICD-9-CM diagnostic codes for discharges before 1 April 2004 and up to 25 ICD-10-CM diagnostic codes for discharges on or after 1 April 2004.
Medical/physician reimbursement claims: consisting of all ambulatory physician visits in Manitoba and include a single ICD-9 diagnostic code associated with each visit, coded to the third digit;
Pharmaceutical drug claims: containing all prescription drug claims from the Drug Program Information Network (DPIN, an electronic, online, point-of-sale prescription drug database that connects Manitoba Health and all pharmacies in Manitoba). Contains information on all prescription drugs dispensed in Manitoba;
Manitoba vital certificates mortality data: a longitudinal population-based registry maintained by Manitoba's Vital Statistical Agency that includes all Manitobans who have died since January 1970 to present and the cause of death;
Child and family services data: a data management system that supports case tracking and reporting of services provided to children and families as they are served through the Manitoba Child and Family services (CFS) System. This database includes information on children in care as well as information of families receiving protection and support services.
See table 1 for descriptions and years of data sets used for analysis.
Description of data sets used for analysis and types of information retrieved
Data linkage
De-identified health records are transferred to MCHP from Manitoba Health, Seniors and Active Living (MHSAL, government department that administers the universal health insurance programme for the province) and contain scrambled identifiers that allow for linkages across multiple databases and years of data. MHSAL acts as a third party for other non-health data providers to develop cross-walk files allowing individual-level linkages across different data sectors. Linkages are performed using de-identified personal health identification numbers, which are unique nine-digit numeric identifiers assigned by Manitoba Health to every person registered for health insurance in Manitoba.
The main sources of data for this work will be the MB FASD database and the databases identified above from the Repository. This linkage produces a powerful tool for studying children and families with FASD that combines the comprehensive health, social and education administrative data with detailed clinical information. For this study the first linkage will identify the study population through linking children identified as having a clinical diagnosis of FASD to their birth mothers. Children diagnosed with FASD through the MB FASD Centre will be linked to their mothers using the ‘Hospital Newborn to Mother Linkage’ which is a Registry file in the Repository. This file contains basic demographic and hospital data on newborns born in a hospital in Manitoba from 1984/1985 onward and their mothers. This file includes all live and stillbirths to Manitoba residents, and babies born in out of province hospitals to Manitoba residents, if reported to MHSAL. Babies not included are those: born out of hospital, born in Manitoba hospitals to out-of-province residents, those born out of province to Manitoba residents who are not reported to MHSAL. A baby's birth record is matched to the mother's obstetrical delivery record using PHINs. The next linkage involves linking the study population to several other Repository data sets (hospital, physician, drug and the social and educational databases specified above) through one-to-one links between PHINs and data records. For example a woman in the Repository identified as having given birth to a child diagnosed with FASD from the MB FASD data set will be linked to her individual hospital abstract records, physician claims records and prescription data records. No identifying information is used to merge these files as linkage is conducted through using encrypted PHINs in order to ensure the utmost privacy and confidentiality of the data of Manitobans.
Study Population: Two groups of women will be generated to address research questions.
Group 1 (Cases/Exposed): Mothers whose children have received a clinical diagnosis of FASD: Clinical data from the MB FASD Centre will be used to ascertain all children and youth (birth to 21 years of age) in Manitoba who have been diagnosed with FASD between 1999 and 2012. This database will be linked to administrative data from the MCHP Repository to identify these children's birth mothers. Only mothers who can be linked to their children (who had a baby–mother linkage), who have postal code information and who were Manitoba residents registered to receive healthcare in the province and covered from their birth until March 2012 will be included. If a mother has multiple children diagnosed with FASD, we will use the first child diagnosed with FASD as the index child.
Group 2 (Comparison group/unexposed): mothers whose children have not received a clinical diagnosis of FASD: Women whose children have never received an FASD diagnosis from the MB FASD Centre, with no known record of prenatal alcohol use in the databases available, and whose children have no evidence of FASD from the Repository will be matched to the exposed group of women on the date of month of birth of the index child, SES and region of residence. Matching will be performed without replacement, at a ratio of three controls for each case. To decrease the likelihood that the comparison women have children with undiagnosed FASD, the following exclusion criteria will be used: (1) women with any children assessed at the Manitoba FASD Centre; (2) women with children who had a diagnosis of FASD as recorded in hospital or physician claims data using the following ICD codes: a hospital visit with ICD 9CM code 760.71, ICD 10CCA code of 86.0 or a physician visit with any ICD 9 code 760; (3) women who had children who had prescriptions for psychostimulants or risperidone; (4) women with children diagnosed with ADHD (due to high comorbidity with a diagnosis of FASD and ADHD;50 ,51 (5) women involved in the InSight Mentoring programme (a programme that provides support for women with alcohol and substance abuse issues); (6) women with a history of substance abuse disorder (including alcohol) during pregnancy as indicated by the physician and hospital claims; (7) women whose newborn risk screen indicates they had used alcohol during pregnancy; and (8) women whose children received special education funding indicating they had severe to profound disabilities.
Study design
Two study designs will be used based on the two different research questions being addressed.
Research question 1
A retrospective matched cohort study design will be used to investigate differences in rates of psychiatric morbidity, suicide attempts and completion, physical health disorders and usage of health and social services (outcome variables) (see figure 1) between our exposed group (group 1) and our unexposed group (group 2) before and after the birth of the index child.

A retrospective matched cohort study design to investigate differences in rates of psychiatric morbidity, suicide attempts and completion, physical health disorders and health and social services utilisation between the exposed unexposed group before and after the birth of the index child.
Research question 2
A retrospective matched case–control design will be used to investigate potential risk factors (exposure variables) associated with giving birth to a child with FASD (outcome) (see figure 2). Our case group (group 3) will be compared to our comparison group (group 4) to investigate whether they had the following risk factors before the birth of the child and whether these factors were associated with giving birth to children with FASD: demographic and socioeconomic factors, family history, mental disorder diagnoses, physical health diagnosis, use of healthcare and social services.

{kind=link}
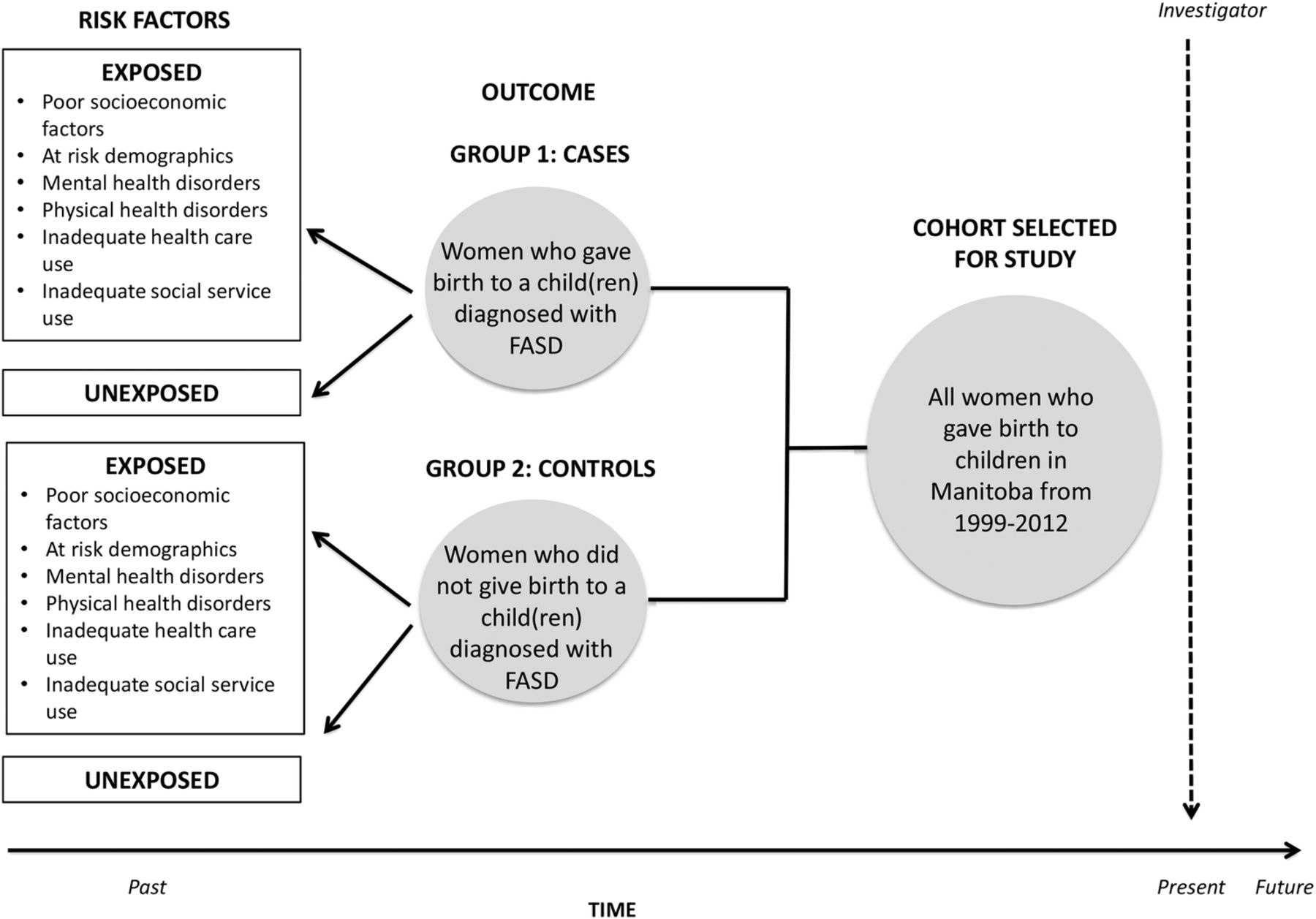{kind=link}
A retrospective matched case–control design to investigate potential risk factors associated with giving birth to a child with fetal alcohol spectrum disorder.
Analysis plan: research question 1
Outcomes
To investigate health outcomes and use of services among our exposed and unexposed groups, the following outcomes will be investigated:
Psychiatric morbidity: diagnosis of substance abuse disorder, personality disorder, mood and anxiety disorder, and schizophrenia 3 years prior to the birth of the index child. Prenatal psychological distress (8 months prior to the birth of the index child) and postnatal psychological distress (from birth to 12 months prior to the birth of the index child) (see table 2 for definitions)
Suicidal behaviour: suicide attempts (3 years before the birth of the index child, during pregnancy, during the postpartum period, until the end of the study period) and completion (from birth to the end of the study period) (table 3).
Physical health disorders: diabetes, hypertension, ischaemic heart disease, total respiratory morbidity (3 years prior to the birth of the index child) (see table 4 for definitions).
Use of healthcare service: average number of physician/ambulatory visits 1 year before the pregnancy with the index child, average number of physician/ambulatory visits during the pregnancy with the index child, average number of all hospitalisations 3 years before the birth of the child, average number of antenatal hospitalisations 3 years before the birth of the index child, late initiation of prenatal care, no prenatal care, low number of prenatal visits, inadequate prenatal care (see table 5)
Use of social services: receipt of healthy baby prenatal benefit (1 year prior to the birth of the child), participation in healthy baby support program (1 year prior to the birth of the child), participation in InSight Mentoring programme (1 year prior to the birth of the child), record of a Family First/Baby First Screen (after the birth of the index child) (see table 6).
Definitions of mental disorders exposure/outcome variables
Definitions of suicide behaviour exposure/outcome variables
Definitions of physical health disorders exposure/outcome variables
Definitions of health services exposure/outcome variables
Definitions of social services exposure/outcome variables
Statistical analysis: Univariate statistics, including proportions and means, will be calculated for all outcome variables (ie, events). Adjusted relative rates for all outcomes will be calculated using generalised estimating equations with a Poisson distribution. A negative binomial distribution will be used if data are overdispersed. Both models are suitable for non-normally distributed data such as counts. All analyses will test for differences between study groups and will adjust for the following covariates: receipt of income assistance, SES (low, middle, high), age of mother at birth of child (18 or under, 19 to 24, 25 to 34, 35 and over).
To model the rates of events for our two groups, we will create a summary data set for the total number of events (eg, total number of mothers with mood and anxiety disorder) for unique strata and the total number of per-person years at risk for the strata. We will include the log of the total number of person-years as an offset in the model to produce an analysis of rates of events, rather than simple counts, and to generate estimates of adjusted RRs of events. This procedure will ensure that any variation in follow-up times for women in the study groups will be accounted for.
Analysis plan: research question 2
To investigate potential risk factors associated with giving birth to a child with FASD, the following exposure variables will be investigated 5 years prior to the birth of the index child for our case and comparison group:
Demographic and socioeconomic factors: maternal age at birth of index child, maternal age at first birth, history of teen pregnancy, region of residence, mean household income, SES, receipt of income assistance, high school completion, involvement with the justice system (see table 7 for definitions);
Family history: marital status, gravidity, parity, birth order of the index child (first, middle, last), involvement with CFS, type of FASD diagnosis of child (see table 8 for definitions);
Diagnosis of a mental disorder: substance abuse disorder, personality disorder, mood and anxiety disorder, schizophrenia, prenatal psychological distress, suicide attempts (table 2);
Diagnosis of a physical health disorder: diabetes, hypertension, ischaemic heart disease, total respiratory morbidity (table 4);
Quality of prenatal care: late initiation of prenatal care, no prenatal care, low number of prenatal visits, inadequate prenatal care (table 5).
Definitions of demographic and socioeconomic exposure/outcome variables
Definitions of family history exposure/outcome variables
Statistical analysis: research question 2: univariate statistics will be used to describe all potential risk factors for cases and comparison women. Bivariate associations between each independent variable and outcome (having a child with FASD) will be conducted as a preliminary investigation of the relationship between the outcome and risk factor. Associations between groups will be tested using t-tests for continuous variables and Pearson's χ2 tests for categorical variables. Variables with a p value of ≤0.2 in the bivariate analysis will be included in a multivariate regression analysis using conditional logistic regression, which is appropriate for studies using a matched case–control design, and accounts for observations that are correlated. Goodness-of-fit tests will be run to test the fit of the model and diagnostics will be run to assess collinearity between independent variables.
Discussion
The MBMomsFASD is the largest, most comprehensive, in-depth investigation into the characteristics, health and mental health, and use of services among women whose children have been diagnosed with FASD. This study offers numerous methodological advantages over studies using primary data collection. First, the use of linked clinical and administrative data is the study's greatest strength. It is difficult to ascertain and follow large groups of women whose children have a clinical diagnosis of FASD using primary data collection, due to challenges of attrition and length of follow-up time needed to obtain longer term outcomes of mothers (eg, suicide). In our study we identify mothers through children who are diagnosed at the Manitoba FASD Centre, which is one of the first and only provincially centralised FASD diagnostic clinics in Canada and as a result, one of the largest. Through the use of linked clinical and administrative data, the MCHP Repository allows the generation of a large population-based group of all women whose children were diagnosed with FASD in Manitoba since 1999 (preliminary n over 700 cases), which is the largest sample size in this field to date, enhancing the generalisability of our study results.
Second, the Manitoba FASD Centre offers a valid and reliable clinical diagnosis of FASD, and as a result we can be certain that women in this sample have given birth to children with FASD. Previous studies investigating characteristics of women who have consumed alcohol during pregnancy cannot confirm a clinically corroborated diagnosis of FASD in children. Therefore, these women may have different characteristics, use of healthcare and social services from those women whose children developed FASD.
Third, through the Repository, we have access to information on the whole population of Manitoba. These data facilitate the creation of clinically relevant comparison groups and accurate comparative analysis. Using the multiple available databases, comparison groups can be created using a host of matched characteristics, including age, sex, SES, geographic location and disease specific cohorts.42 These comparative analyses are difficult to perform using primary data recruitment methods as controls and cases can be difficult to identify, can take years to recruit and are subject to attrition.48 Moreover, through the use of hospital, physician, educational and social administrative data to develop exclusion criteria, the likelihood that women in the comparison group had children with undiagnosed FASD can be decreased. This is potentially a major limitation in previous studies as FASD is an extremely underdiagnosed condition.
Fourth, through leveraging the comprehensive, longitudinal databases available at MCHP, we can investigate novel health outcomes not yet studied. Specifically we can document the mental health diagnoses of women who give birth to children with FASD and determine rates of prenatal and postnatal anxiety and depression, as well as suicide attempts and completions. Women with alcohol substance use issues are at higher risk for prenatal and postpartum depression,52–54 investigating these outcomes specifically in mothers who give birth to children with FASD can provide evidence to policymakers responsible for optimising FASD prevention and support resources. Furthermore, maternal suicide is an increasing public health issue55 and investigating whether women who give birth to children with FASD are at increased risk for suicide is also important to optimise support resources and that these women do not slip through the cracks. Furthermore, due to the longitudinal nature of the data, an analysis of system usage of women before, during and after pregnancy can be conducted and compared to women in the general population whose children have not been diagnosed with FASD. This analysis is important to identify points for prevention, early intervention and treatment and effective resource allocation, as well as supporting the health and well-being of women who give birth to children with FASD. The Repository is ideal for these analyses, as the data accurately calculate the usage of healthcare services and have been validated for research purposes.42–44 ,47 ,48 ,56 ,57 MCHP data have been used to calculate the usage of the healthcare services among related populations in the past; for example, Brownell et al58 used MCHP data to document the usage of health and social systems among children with FASD.
Finally, administrative data eliminate re-call bias and offer accurate information that can be isolated in critical periods of time throughout a study participant's lifespan. It is difficult to conduct studies on mothers with children with FASD due to stigmatisation and attrition of study participants. Furthermore, studies using primary data collection may be conducted after a significant time period has passed because of these women's pregnancies. This makes the recall of specific diagnoses, events and use of health services during the pregnancy difficult and increases the likelihood of inaccuracy. The use of our data is an important opportunity to ascertain accurate, unbiased information on these mothers and their use of health and social services and comorbid diagnoses before and during pregnancy and the postpartum period.
While the use of routinely collected population data has numerous advantages, there are a few limitations that warrant discussion. First, the use of a clinically referred FASD sample may limit the generalisability of findings, as we may be missing women and children who are not referred to this clinic. Owing to the complex nature of FASD, the multiple comorbidities associated with the disorder, underreporting, coding patterns of physicians and the complex multidisciplinary teams required to diagnose FASD, there is no algorithm that has been developed to identify children with FASD in the MCHP Repository using other data sources. Therefore, record linkage with the Manitoba FASD Centre is necessary to confirm a clinical diagnosis of FASD in children in Manitoba. However, the referrals to the clinic come from a wide variety of sources and from all regions in the province, strengthening the representativeness across populations. Second, while we have taken great care in excluding all mothers with possible prenatal alcohol exposure and children with a diagnosis of FASD, we cannot be certain that there are no women in our comparison group who do not have un-reported prenatal alcohol use or children with undiagnosed FASD. However, this would serve to weaken rather than strengthen any of our findings. Furthermore, as in all studies using administrative databases, this study is reliant on the accuracy of data submitted by the organisations that deliver services, and may have variations in data collection methods and compliance rates in the recording of information that may result in data errors.42 However, as previously stated, MCHP data have been extensively validated for conducting this type of research. Furthermore, outcome data are dependent on the individual making contact with the healthcare system and are, therefore, a report of treatment prevalence; thus, this study would exclude women with undiagnosed physical health or mental health disorders. Furthermore, the Repository does not capture information on interpersonal relationships, violence and abuse, psychological trauma or patient insight, which is important for the understanding of underlying causes of the drinking during pregnancy and would provide context to results of larger quantitative studies. However, data collection methods are often resource and time intensive and studies with patient insight often have small sample sizes, limiting generalisability. Although these types of data are not readily available in the Repository, the results of this study have the potential to lay the groundwork for the development of future work in this area. Finally, due to the exploratory nature of this study, there are multiple comparisons being performed and we acknowledge the potential for an inflated type 1 error, which is a limitation of this work. Future research should be conducted that corroborates the results from this proposed study.
Dissemination
This study will be conducted at MCHP, which is a secure computing environment. Strict security measures are in place to protect the data files and to restrict access. The data in the Repository contain no identifiable personal information and are used only for research purposes. Data will be presented in a summary form, ensuring that identification of individuals is not possible.
To ensure the translation of the project's findings to policymakers, government stakeholders and community organisations, a study advisory group comprising physicians specialising in FASD, members of Healthy Child Manitoba (a provincial governmental organisation that works with the community to improve the well-being of Manitoba's children and youth) and FASD researchers has been established. During the final stages of the project, we will hold a forum to discuss policy implications arising from the project. Outputs from the project will include peer-reviewed papers, summary reports in formats intended for policy and community organisations and presentations at academic conferences and government meetings.
Conclusion and policy implications
The databases brought together for this study and the results produced will generate a significant amount of longitudinal outcome data and contribute to our understanding of the life circumstances of mothers who give birth to children with FASD. The study results will provide an informed picture of the determinants of health that place women at increased risk of alcohol consumption during pregnancy, and giving birth to children with FASD. Moreover, the study results will offer insight into how women whose children have been diagnosed with FASD navigate health and social service systems during the perinatal and postnatal periods. These results will add to the evidence base and facilitate FASD prevention efforts through identifying: (1) high-risk women who should be targeted for prevention and intervention, (2) areas in health and social services that can be targeted for FASD prevention and support programmes to enhance service delivery to this population. Research providing insight into the factors that place women at risk for having children with FASD is vital for effective targeting and developing of policy resources that can help women cope with the influences and stresses in their lives in order to decrease prenatal alcohol consumption and ultimately prevent FASD.
Acknowledgments
The authors acknowledge the Manitoba Centre for Health Policy for the use of data contained in the Population Health Research Data Repository under project file HIPC#2013/2014–2020 of the Government of Manitoba's Health Information Privacy Committee and under project HS16460(H2013:221) of the University of Manitoba Faculty of Health Sciences, College of Medicine Health Research Ethics Board, as well as the following data providers: the Manitoba FASD Centre and the Winnipeg Regional Health Authority, Healthy Child Manitoba Office, the Manitoba FASD Centre and the Winnipeg Regional Health Authority, Manitoba Families, and the Department of Education and Training. The results and conclusions are those of the authors, and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Healthy Living and Seniors or other data providers is intended or should be inferred.
References
Footnotes
Contributors This study was conceived by DS. All authors contributed to the design of the study. DS will perform data analysis, and with MB, LLR, SL, AH-D and DC, will interpret the data. All authors participated in the preparation of this manuscript, revised it critically for important intellectual content and approved the version submitted for publication.
Funding Funding from this project was received from two Graduate Studentship Awards from Research Manitoba, the PhD Dissertation Award from Research Manitoba, the Evelyn Shapiro Award for Health Services Research from the Manitoba and from the Canadian Foundation on Fetal Alcohol Research.
Competing interests None declared.
Ethics approval This study was approved by the University of Manitoba's Health Research Ethics Board (HS16460(H2013:221)) and the Manitoba Health Information Privacy Committee (HIPC#2013/2014–2020). Data access was approved by MCHP and the following data custodians: the Manitoba FASD Centre and the Winnipeg Regional Health Authority, Healthy Child Manitoba Office, the Manitoba FASD Centre and the Winnipeg Regional Health Authority, Manitoba Families, and the Department of Education and Training.
Provenance and peer review Not commissioned; externally peer reviewed.