Article Text

Abstract
Objective To examine the impact of access to primary care physicians (PCPs), geographic availability of orthopaedic surgeons, socioeconomic status (SES), proportion of older population (≥65 years) and proportion of rural population on orthopaedic surgeon office visits and orthopaedic surgery.
Design Population multilevel study.
Setting Ontario, Canada.
Participants Ontario residents 18 years or older who had visits to orthopaedic surgeons or an orthopaedic surgery for musculoskeletal disorders in 2007/2008.
Primary and secondary outcomes Office visits to orthopaedic surgeons and orthopaedic surgery.
Results Access to PCPs and the index of geographic availability of orthopaedic surgeons, but not SES, were significantly associated with orthopaedic surgeon office visits. There was a significant interaction between access to PCPs and orthopaedic surgeon geographic availability for the rate of office visits, with access to PCPs being more important in areas of low geographic availability of orthopaedic surgeons. After controlling for office visits with orthopaedic surgeons, the index of geographic availability of orthopaedic surgeons was no longer significantly associated with orthopaedic surgery.
Conclusions The findings suggest that, particularly, in areas with low access to PCPs or with fewer available orthopaedic surgeons, residents are less likely to have orthopaedic surgeon office visits and in turn are less likely to receive surgery. Efforts to address adequate access to orthopaedic surgery should also include improving and facilitating access to PCPs for referral, particularly in geographic areas with low orthopaedic surgeon availability.
- Primary Care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The comprehensive coverage of the Ontario public funded healthcare system enables us to examine data on office visits to orthopaedic surgeons and surgery for musculoskeletal disorders in Ontario, Canada. We were able to examine the source of variability in orthopaedic surgeon office visits and orthopaedic surgical rates by looking at access to primary care physicians and availability of orthopaedic surgeons.
-
The databases used do not have information about individual's socioeconomic status, thus we had to use an area-level indicator.
-
We relied on utilisation rates as a proxy measure of access to primary care physicians since the amount of service provided by primary care physicians by health regions was not available.
-
The data used do not enable us to examine the circumstances of the orthopaedic practice, such as surgeon preferences.
Introduction
Access to orthopaedic surgery is an ongoing concern with long waiting times, particularly for total joint replacement surgery (TJR), being a recurrent theme in the media and politics of healthcare delivery. This concern is further fuelled by the prospect of increased demand because of the aging of the baby boomer generation.1–5 Furthermore, potential shortages in healthcare resources, not least orthopaedic surgeons and hospital-based resources for surgery, are also a concern.1 ,5–10 Studies of access to orthopaedic surgery have mainly focused on TJR and individual-level factors such as socioeconomic status (SES), ethnicity and patients’ and surgeons’ preferences.10–19 Although the literature provides some insights regarding factors associated with access to TJR, considerably less information exists about access to orthopaedic surgery in general, including office visits to orthopaedic surgeons for a surgical opinion.20 While it is well recognised that there are geographic variations in rates of surgery,21–23 few studies have looked at the contribution of organisational factors such as the geographic distribution of surgeons or distance to services.10 ,24 ,25 A surprising omission in these studies is the limited attention that has been paid to access to primary care physicians (PCPs), a crucial first step where access to surgery is via referral to a specialist.
Our previous studies suggest that surgery is only one component of the work of orthopaedic surgeons in the management of musculoskeletal disorders (MSD). We also found that a substantial proportion of referrals were for the medical management and treatment of these conditions.26 ,27Another study of ours suggested that geographic variation of surgeon supply partially explained observed geographic variation in the rate of office visits to orthopaedic surgeons.10 However, in this study we examined geographic variation in utilisation of orthopaedic surgeons across large health areas. We also used a provider-to-population ratio to estimate orthopaedic surgeons’ availability for each area. These ratios are commonly used for comparisons across health regions; however they do not take into account the possibility of patients crossing health region borders for care.28 Therefore, the purpose of this study is to examine the impact of access to PCPs, geographic availability of orthopaedic surgeons, and indicators of potential need for care on utilisation of orthopaedic surgeon office services and surgery. We used an index of geographic availability of orthopaedic surgeons that incorporates travel distances and will examine geographic variation in utilisation rates across 105 smaller health planning areas.
Our analytic strategy is presented in figure 1A. In summary, we expect that, in a referral system, access to PCPs as well as the geographic availability of orthopaedic surgeons will be associated with the rates of office visits to orthopaedic surgeons. Furthermore, studies suggest that proximity to specialists influence PCPs referral decisions.29 ,30 We therefore, expect that the relationship between access to PCPs and the rate of orthopaedic surgeons office visits will be modified by the geographic availability of orthopaedic surgeons. Finally, we anticipate that access to PCPs, the geographic availability of orthopaedic surgeons, and office visits to orthopaedic surgeons will be positively associated with orthopaedic surgery rates.

Conceptual model (A) and summary of findings (B), combining the results of main effect and adjusted models. RR, rate ratio; RR are for highest quintile versus lowest quintile of the distribution; NS, not significant. All estimates are adjusted for age, sex age and sex interaction, area-level socioeconomic status, proportion population 65 years and over and proportion of rural population.
Methods
Setting and study design
This is a population-based multilevel study of individuals with MSD aged 18 years and over living in 105 health planning areas in Ontario, Canada, who used orthopaedic surgeon services in the fiscal year 2007–2008 (1 April 2007 to 31 March 2008). All medically necessary hospital and physician services are covered by the Ontario Health Insurance Plan (OHIP). Access to orthopaedic surgeons is by referral from other physicians, typically PCPs. However, there are no restrictions on the location of orthopaedic surgeons to whom referral can be made.
The health planning areas are administrative areas known as subLocal Health Integration Networks (subLHIN). Local Health Integration Networks (LHINs) were created by the Ontario government in 2006. These are 14 not-for-profit organisations working with local health providers and community members to determine the health service priorities of each region. The boundaries of the 14 LHINs reflect patients’ patterns of healthcare services utilisation in their communities. In addition, each LHIN has identified subLHIN areas for planning within their LHIN. Owing to the fact that LHINs vary substantially in size and population, the number of subLHINs differs. As such, a subLHIN may represent specific communities or aggregations of communities.31 The population of subLHIN's ranges from 3820 to 433 805, with the least populous subLHINs being in rural areas.
Data sources
Data on the number of patients with at least one office visit to an orthopaedic surgeon or PCP for MSD or who had an orthopaedic surgery were obtained for each health planning area. The OHIP physician billings database linked to the Registered Persons Database provided data on patients with office visits to PCPs and orthopaedic surgeons with diagnostic codes relevant to MSD. These were arthritis and related conditions (osteoarthritis, rheumatoid arthritis, traumatic arthritis, synovitis, ankylosing spondylitis), injury and related conditions (fractures and dislocations, sprains and strains, joint derangement and other trauma), and bone and joint conditions (other spine, bone and unspecified joint disorders; see online supplementary table A1).27 ,32 Physician specialty was defined using the Institute of Clinical Evaluative Sciences Physician Database (IPDB). The IPDB was linked to the OHIP database to identify visits to orthopaedic surgeons and PCPs. All claims made by the same physician on the same date for the same patient were considered one visit.
The Canadian Institute for Health Information (CIHI), Discharge Abstract Database (DAD) and the National Ambulatory Care Registry System (NACRS) were used to obtained data on orthopaedic surgeries carried-out as inpatient and outpatient procedures, respectively.33 Individuals with orthopaedic surgery were identified if they had at least one inpatient hospitalisation or outpatient surgery where an orthopaedic surgeon was the main healthcare provider. Inpatient hospitalisations and day surgeries with a diagnostic code of MSD were kept for analysis (see online supplementary table A2).27
Variables
Outcomes: Two main outcomes were used for analysis: having at least one office visit to an orthopaedic surgeon and having at least one orthopaedic surgery for MSD.
Need indicators: Given that the prevalence of MSD is higher in older people, those with low SES, and those living in rural areas,34–36 it is natural to assume that potential need for orthopaedic care at the population level is likely related to the distribution of these factors in the population. Therefore, three indicators of potential need for each health planning area were calculated using data from Statistics Canada 2006 Census. These indicators were the proportion of the population aged ≥65 years, proportion of rural population and SES. SES was calculated by combining the median household income with the proportion of the population with less than high school using a similar approach to Diez-Roux et al.37 Both components were standardised into a z-score and combined into the overall SES score.
Access to PCPs: Data on the amount of care provided by PCPs in each location in Ontario were not available. However, data from Ontario show that MSD is one of the most frequent reasons for seeing PCPs.38 Therefore, the rate of individuals visiting PCP for MSD was used as a proxy measure of access to PCPs.
Geographic availability of orthopaedic surgeons. A 2006 survey of Ontario orthopaedic surgeons provided data on postal codes of all orthopaedic surgeon practice locations in Ontario. It also provided the number of hours per week working in the office and performing surgeries at each location.10 ,39 Practice locations were geo-coded using Geographic Information System (GIS) software40 and assigned to a dissemination area (DA). DAs are the smallest geographic units for which census data are available (19 777 in Ontario). A geographic availability index was derived for each health planning area using a gravity model.28 In the first step, working from each DA population centroid, distance from each orthopaedic surgeon location to each DA population centroid was calculated using the Minkowski metric,41 which has been found to be a good approximation to the road distance. In a second step, for each DA all orthopaedic surgeon locations within a reasonable distance (we used 50 km) were identified. Then, the hours of office and surgical care available from these orthopaedic surgeons were weighted by the inverse of the squared distance from the population to the orthopaedic surgeon location. Thus, the farther away the orthopaedic surgeon location the lower contribution this location made to the overall availability for the population. In a next step, the sum of the weighted hours was calculated for each DA. In a final step the index at the DA level was aggregated to the health planning area. All spatial calculations were performed using ArgGIS 9.1 and SAS V.6.2.
Statistical analysis
Multilevel Poison regression modelling was used to examine factors associated with the rates of office visits to orthopaedic surgeons and orthopaedic surgery. The outcomes were modelled as age and sex strata nested within each health planning area. As the increase with age in the rate of office visits and surgery differed by sex, an age-sex interaction term was added to all models.27 Random intercept models were used to allow the outcomes to vary across health planning areas. The Poisson distribution was used and in the presence of overdispersion, a generalised Poisson model was fitted.42 Population counts for each stratum were added as an offset in all models. The estimates obtained from the regression models compare the log of the rate of the outcome (eg, orthopaedic surgery) by individual and area-level indicators. Rate ratios were calculated by exponentiating the regression coefficients.
We used a sequential approach to perform the analyses. All models included individuals’ age, sex and an age–sex interaction term. We modelled office visit rates and surgical rates separately, testing for main effects as well as adjusted models, with a final adjusted model for surgical rates which also included orthopaedic surgeon office visit rates. Finally, we examined whether the relationship between access to PCPs and orthopaedic surgeon office rates was affected by the geographic availability of orthopaedic surgeons in adjusted models by including an interaction term between access to PCPs and the orthopaedic availability index.
For analytic purposes, all area level indicators were categorised in quintiles to facilitate interpretation with the exception of the proportion of rural population, which was categorised as follows: <15%, 15–50% and ≥50%. Analyses were conducted in SAS (proc GLIMMIX) and rate ratios for the fixed effects (ie, individual and area-level predictors) and 95% CIs from multilevel regression models are presented.
Sensitivity analysis: Analyses are presented for the index of geographic availability of orthopaedic surgeons calculated using a distance of 50 km. Analyses with the index calculated using 25, 75 and 100 km thresholds yielded similar results. Analyses using an orthopaedic availability index with office hours for office visits, and surgeon surgical hours for surgeries showed no discernible variations.
Results
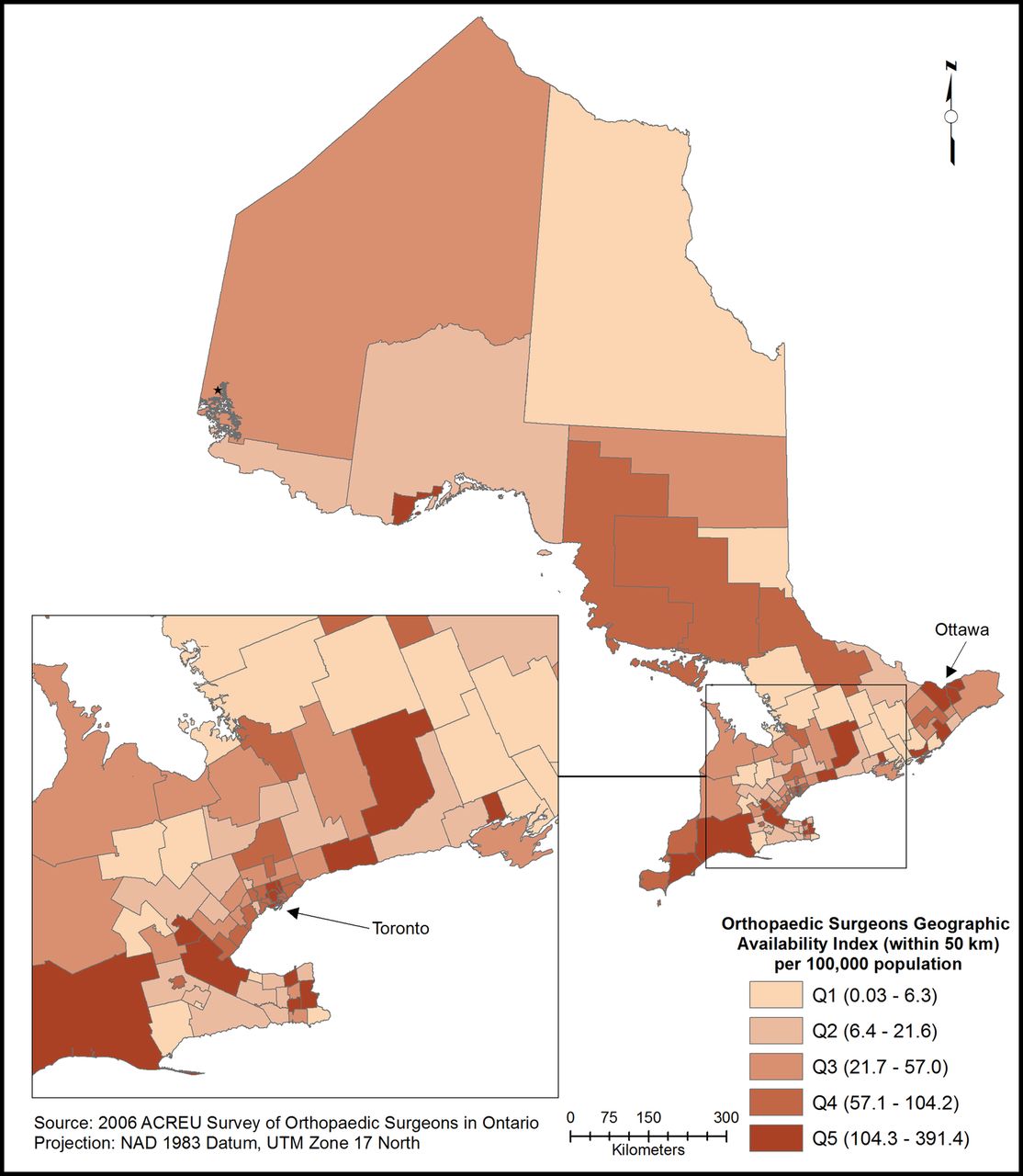
In the 2007/2008 fiscal year there were 477 000 individuals with office visits to orthopaedic surgeons, 132 600 individuals with orthopaedic surgery for MSD, and almost 2.4 million individuals made at least one visit to PCPs for MSD in Ontario. Table 1 presents summary data for use of orthopaedic surgeon services, access to PCPs and the geographic availability of orthopaedic surgeons’ index. Almost 5% of the population made at least one office visit to orthopaedic surgeons, and 1.5% had an orthopaedic surgery. One-quarter of the population 18 years and older made at least one visit to PCPs for MSD in Ontario with a fourfold variation in the rate across health planning areas. The median distance to the nearest orthopaedic surgeon was 11.5 km and ranged up to 342 km. Nevertheless 97.5% of the population lived within 50 km of an orthopaedic surgeon. The median geographic availability of orthopaedic surgeons’ index (using a 50 km radius) was 57 h/week/100 000 population with a sevenfold variation across the health planning areas (figure 2).
Use of orthopaedic surgeons services, access to primary care physicians (PCP) by those 18 years and older and availability of orthopaedic surgeons across health planning areas (n=105), Ontario: 2007–2008
{kind=link}
{kind=link}
Index of geographic availability of orthopaedic surgeons (within 50 km) per 100 000 population by health planning areas in Ontario: 2006.
Rates of individuals with office visits to orthopaedic surgeons and with orthopaedic surgery for MSD increased with increasing age (see online supplementary tables A3 and A4, respectively). The rate of surgery was higher in women aged 55 years and over than in men in the same age groups and the reverse was seen in those aged 44 years and younger (p<0.0001). A similar pattern was seen for the rate of office visits. Descriptive analyses showed no regular patterns in rates of office visits to orthopaedic surgeons or orthopaedic surgery across quintiles for access to PCPs or the geographic availability of orthopaedic surgeons. The rate of office visits to orthopaedic surgeons and orthopaedic surgery was higher in the highest quintiles of SES. The rate was also higher in the highest quintiles of the population aged ≥65 years (table 2).
Rate of persons with at least one office visit to orthopaedic surgeons and with at least one orthopaedic surgery for musculoskeletal disorders, Ontario: 2007–2008*
Office visits to orthopaedic surgeons
Table 3 displays the findings for main effect and adjusted models for office visits to orthopaedic surgeons, with the overall findings summarised in figure 1B. Age, sex and the age–sex interaction were significantly associated with office visits in all models (data not shown). Findings from the main effect models (table 3, 2nd column) indicate that neither access to PCPs nor the geographic availability of orthopaedic surgeons’ index were significantly associated with office visits to orthopaedic surgeons. However, in the adjusted model (table 3, 3rd column) both were positively associated with office visits to orthopaedic surgeons suggesting an interaction between the two. At first examination, we estimated the models with the availability of orthopaedic surgeons and access to PCPs as continuous variables and found that the interaction term was statistically significant (p<0.001). This result suggested a linear trend of increased utilisation of orthopaedic surgeon office services with increasing access to PCPs for a given level of availability of orthopaedic surgeons. For ease of interpretation we then carried out a stratified analysis by the orthopaedic availability index. For this stratified analysis we grouped the orthopaedic availability index into tertiles in order to have adequate sample size to perform the estimations. The results of the stratified analysis are presented in table 4. Access to PCPs was significantly and positively associated with office visits to orthopaedic surgeons in areas in the lowest and middle tertiles of orthopaedic surgeon availability. For example, in areas of lowest availability of orthopaedic surgeons, residents of health regions in the top quintile of access to PCPs were 50% more likely to have visits to orthopaedic surgeons than those in the bottom quintile of access to PCPs.
Multilevel Poisson regression models for office visits to orthopaedic surgeons for MSD: results for the main and adjusted effects of access to PCP, geographic availability of orthopaedic surgeons and need indicators, Ontario: 2007–2008
Multilevel Poisson regression model*: rates ratios (95% CIs) for the effects of access to PCP on the rate of office visits stratified by tertiles of geographic availability of orthopaedic surgeons, Ontario: 2007–2008
The proportion of the population aged ≥65 years was significantly associated with office visits to orthopaedic surgeons in the main and adjusted models; while the proportion of rural population was only significant in the adjusted model.
Orthopaedic surgery
Table 5 displays the findings for main effect and adjusted models for orthopaedic surgery. In the main effect models (table 5, 2nd column) access to PCP was not significantly associated with the rate of orthopaedic surgery, while there was a negative association with the index of geographic availability of orthopaedic surgeons. However, the associations of the orthopaedic accessibility index, SES and age of the population, and urban/rural status with orthopaedic surgical rates in the main effect models were no longer apparent after adjustment for the rate of orthopaedic surgeon office visits (table 5, 3rd column).
Multilevel Poisson regression models for orthopaedic surgery for MSD: results for the main and adjusted effects of access to PCP, geographic availability of orthopaedic surgeons and need indicators, Ontario: 2007–2008
Analysis restricted to visits to orthopaedic surgeons and to surgery for arthritis and related conditions and injury and related conditions showed similar results (see online supplementary tables A5 and A6).
Discussion
Using geographic variation as a probe and controlling for indicators of potential need, this study examined the impact of the geographic availability of orthopaedic surgeons and access to PCPs on variations in rates of utilisation of orthopaedic services for MSD across health regions in Ontario, Canada. Our findings point to the importance of both geographic availability of orthopaedic surgeons and access to PCPs in explaining variations in rates of office visits to orthopaedic surgeons. This is one of the first studies to focus on the factors associated with office visits to orthopaedic surgeons. The findings show that access to PCPs is particularly important in areas with lower orthopaedic surgeon availability. This is in line with studies suggesting that the awareness of specialist availability by PCPs affects their referral decisions.29 ,30 The lack of association between orthopaedic surgeon availability and surgical rates after accounting for the rate of orthopaedic office visits suggests that it is access to office-based services that is crucial for getting access to surgery. Therefore, provision of greater resources for surgery alone would not increase surgical rates unless attention is also paid to factors affecting access to orthopaedic office visits.
The primary focus of this study was all MSD as we were interested in examining the total caseload of orthopaedic surgeons. Taken together arthritis and related conditions and injury represent approximately 80% of all orthopaedic surgeon visits for MSD.27 Restricting analyses to these subgroups gave similar results. This is perhaps not surprising as all surgery for arthritis and related conditions and most surgery for injury have a prior orthopaedic surgeon office visit: about 5% of all surgeon contacts are for immediate surgery.26
Few studies have examined variations in access to orthopaedic surgery by focusing on the availability of orthopaedic surgeons and these have used a crude measure of availability, namely surgeon-to-population ratio.10 ,24 ,43 As we had access to detailed data on the location and hours of office-based and surgical care provided by Ontario surgeons, we were able to calculate a geographic availability index by combining the amount of services available with the distance between orthopaedic surgeons and population locations, under the assumption that the closer the medical services, the easier it is to access them. This index is an improvement over traditional physician-to-population ratios since it incorporates an indicator of travel distances. A key characteristic of the index is the ability to provide a more realistic measure of the availability of orthopaedic surgeon services, particularly for health planning areas with few orthopaedic surgeons that are adjacent to areas of more ample availability.
In our study we looked more comprehensively at the steps leading to potential surgery (figure 1A) by examining access to PCPs and access to orthopaedic surgeons in the office for consultation. Determining population need for healthcare interventions is challenging and has been given attention in the literature.3 ,44 As in our study, in the absence of reliable measures of need for healthcare, others have relied on population characteristics to assess need at the population level.43 ,44 As expected, we found that individual age was associated with both orthopaedic office visits and surgery. Furthermore, we found that areas with a higher proportion of older population also have higher rates of orthopaedic office visits. While this could be an indicator of need, it may also reflect a concentration of healthcare services for the older population, or the effect of social networks in the older population.
The lack of association between SES and the rates of office visits and/or surgery is in contrast with studies showing that rates of TJR are lower among those of low SES.2 ,15 ,24 While we did see a significant SES effect for orthopaedic surgery in our main effect model, this was no longer the case when we adjusted for the other variables. Further exploratory analyses (data not shown) indicated that SES might be serving as an indicator for access to PCPs and orthopaedic surgeon availability. Similarly, an initial finding of lower rates for surgery in urban areas, compatible with lower rates of TJR in urban areas,17 was no longer significant in adjusted analyses.
A major advantage of this study is the comprehensive coverage of the Ontario publicly funded healthcare system, which covers all medically necessary physician visits. This allowed us to examine data on office visits to orthopaedic surgeons and surgery for all MSD, not just the 25% of orthopaedic surgery represented by TJR.27 Moreover, we were able to examine the source of variations in surgical rates by looking at factors in the care pathway at the level of primary care and orthopaedic care.
Our study's limitations are those inherent to ecological studies and the use of health service data. A limitation of the databases used is the lack of individual data associated with need for healthcare such as SES, consequently we had to use area-level indicators. Unfortunately we did not have data on the circumstances of orthopaedic practice such as surgeon preferences13 ,22 ,45 or barriers to surgery (eg, availability of operating room resources).10 However, to the extent to which availability of surgical and office hours could be considered as a proxy for surgical resources, our findings suggest that the key aspect is access orthopaedic surgeons in the office for consultation. We did not have an accurate count of practicing PCPs within each health region and the amount of care provided. Therefore, we relied on a measure of utilisation as a proxy for access to PCP. Differences in PCP utilisation rates may reflect not only variation in the number of available physicians but differences in the preferences of physicians in managing common MSD.46 They may also reflect differences in need in the population for which we do not have a direct measure. Nevertheless, our results point to the importance of considering factors related to access to PCPs to ensure adequate access to orthopaedic services in the population. Finally, our study is based in Ontario, Canada, and it is unknown to what extent the findings can be generalised to other jurisdictions.
Conclusion
Our study found that, particularly, in areas with low access to PCPs or fewer orthopaedic surgeon resources, residents are less likely to use office-based orthopaedic surgeon services, and in turn are less likely to receive orthopaedic surgery. Clearly, lack of access to PCPs affects both access to orthopaedic surgery and, more generally, access to the expertise of orthopaedic surgeons in the diagnosis and management of MSD. These results suggest that increasing capacity for surgery alone may not be enough to improve access to orthopaedic surgery. Efforts to address access to orthopaedic surgery should also include improving and facilitating access to both PCPs for referral and orthopaedic office consultations. Further research is warranted to extend this work by examining individual and organisational factors along the orthopaedic care pathway that may affect how individuals access orthopaedic services.
Acknowledgments
The authors are grateful to Dr Nizar Mahomed, Director of the Arthritis Programme and Division of Orthopaedics, Toronto Western Hospital and the University of Toronto, for his input and advice. The authors are also grateful to the reviewers for their comments and suggestions which helped us to improve our paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors MC performed the statistical analysis and wrote the first draft of the article and EMB and AMD revised the manuscript and critically contributed to its content. All authors approved the final version.
-
Funding This study was supported by a CIHR Team Grant in Models of Care in Arthritis (ETG 92253). Additional support was given by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
-
Competing interests None.
-
Ethics approval The study was approved by the Institutional review board of Sunnybrook Health Sciences Centre.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.