Article Text

Abstract
Background: Acute myocardial infarction (AMI) is the leading cause of death attributed to cardiovascular diseases. An association between traffic related air pollution and AMI has been suggested, but the evidence is still limited.
Objectives: To evaluate in a multicentre study association between hospitalisation for first AMI and daily levels of traffic related air pollution.
Methods: The authors collected data on first AMI hospitalisations in five European cities. AMI registers were available in Augsburg and Barcelona; hospital discharge registers (HDRs) were used in Helsinki, Rome and Stockholm. NO2, CO, PM10 (particles <10 μm), and O3 were measured at central monitoring sites. Particle number concentration (PNC), a proxy for ultrafine particles (<0.1 μm), was measured for a year in each centre, and then modelled retrospectively for the whole study period. Generalised additive models were used for statistical analyses. Age and 28 day fatality and season were considered as potential effect modifiers in the three HDR centres.
Results: Nearly 27 000 cases of first AMI were recorded. There was a suggestion of an association of the same day CO and PNC levels with AMI: RR = 1.005 (95% CI 1.000 to 1.010) per 0.2 mg/m3 and RR = 1.005 (95% CI 0.996 to 1.015) per 10000 particles/cm3, respectively. However, associations were only observed in the three cities with HDR, where power for city-specific analyses was higher. The authors observed in these cities the most consistent associations among fatal cases aged <75 years: RR at 1 day lag for CO = 1.021 (95% CI 1.000 to 1.048) per 0.2 mg/m3, for PNC = 1.058 (95% CI 1.012 to 1.107) per 10000 particles/cm3, and for NO2 = 1.032 (95% CI 0.998 to 1.066) per 8 μg/m3. Effects of air pollution were more pronounced during the warm than the cold season.
Conclusions: The authors found support for the hypothesis that exposure to traffic related air pollution increases the risk of AMI. Most consistent associations were observed among fatal cases aged <75 years and in the warm season.
- AMI, acute myocardial infarction
- HDR, hospital discharge register
- HEAPSS, Health Effects of Air Pollution among Susceptible Sub-populations
- PNC, particle number concentration
- UBRE, un-biased risk estimator
- air pollution
- particulate matter
- myocardial infarction
- ultrafine particles
Statistics from Altmetric.com
- AMI, acute myocardial infarction
- HDR, hospital discharge register
- HEAPSS, Health Effects of Air Pollution among Susceptible Sub-populations
- PNC, particle number concentration
- UBRE, un-biased risk estimator
Many epidemiological studies have linked the changes in daily air pollution levels to increased daily cardiovascular mortality and morbidity.1,2 However, the group of harmful cardiovascular conditions is diverse. By using more specific endpoints in studies it is possible to provide not only more accurate estimates for risk analyses, but potentially also information on disease mechanisms. Acute myocardial infarction (AMI) is the leading cause of death attributed to cardiovascular diseases. Several epidemiological studies have linked increased air pollution levels with increased risk of AMI.3–5
The important harmful characteristics of air pollution are still unclear. The main candidates include chemical composition, especially carbon compounds and heavy metals,6,7 or high number of ultrafine particles (<0.1 μm).8 Epidemiological studies have suggested that crustal material may have less of an effect on health than combustion particles.9,10 Traffic related combustion particles have been associated with increased mortality in cohort studies.11 Recently, short term exposure to traffic has been associated with the triggering of onset of myocardial infarction.12
The present study was conducted as part of the HEAPSS (Health Effects of Air Pollution among Susceptible Sub-populations) project, aimed at evaluating the effects of air pollution on cardiovascular diseases in five European cities. We have previously shown combustion originating air pollutants to be associated with fatal, non-hospitalised coronary events in Rome, Italy.13 In the HEAPSS cohort of AMI survivors, we have found an association between ambient air pollution and increased risk of cardiac hospital readmissions.14 The aim of the present study was to analyse the associations between traffic related air pollution and hospitalisation for first AMI, the event responsible for the individual’s inclusion into the HEAPSS cohort. CO and NO2 were included in the study as indicators of traffic related air pollution, while particle number concentration (PNC) was included both as an indicator of traffic related air pollution and by merit of possible direct causal association with AMI, since it is a good proxy for ultrafine particle concentration.15 There is a general lack of long measurement series of PNC. In the current study, we modelled PNC retrospectively.16,17
METHODS
Subjects
We collected data on hospitalisations for first acute myocardial infarction (AMI) in five European cities (table 1). Depending on the availability of data sources, either AMI registers (Augsburg and Barcelona) or hospital discharge registers (HDRs) (Helsinki, Rome, and Stockholm) were used. Patients were included in the study if they were aged 35 or above (under 75 in Augsburg, under 80 in Barcelona), and resident in the study area.
Characteristics of acute myocardial infarction (AMI) patient data sources in the five cities, and number of hospital admissions for first AMI during the study period
The definition of AMI in Augsburg and Barcelona followed the MONICA recommendations.18 In Augsburg, patient data on AMI cases dying within 24 hours from hospitalisation were not available. In Helsinki, Rome, and Stockholm, hospitalisations for AMI (ICD-9 = 410; ICD-10 = I21, I22) recorded in acute care hospitals were selected. AMI diagnoses in HDRs and in AMI registers following MONICA recommendations have been found to be highly comparable.19–21 In order to increase the specificity of the AMI diagnoses in the HDRs, hospitalisations shorter than three days were excluded, as they are most likely to represent ruled out AMI. In Helsinki and Stockholm, the specificity was further improved by excluding hospitalisations recorded as elective (non-acute). In Augsburg and Barcelona AMI was defined as first based on the recorded patient history. In the other three cities AMI was defined as first if record linkage found no AMI hospitalisations during the previous three years, and if no ICD code indicating a previous infarction (ICD-9: 412, ICD-10: I25.2) was found as a secondary diagnosis in the record of index event.
Environmental data
An average of the city monitors representing inner city background levels of air pollution was used in the analyses. However, in Augsburg scaling down total suspended particulate matter concentrations with a factor of 0.83 formed an estimate of PM10 concentrations. The scaling factor was chosen based on earlier empirical data and information from the Bavarian Environmental Protection Agency. In Barcelona, daily estimates of PM10 for the two missing years were constructed using a linear prediction model that included concentrations of total suspended particles and black smoke.
Analyses on ozone were restricted to warm season (April–September), because levels and correlations with other pollutants depend on season, and health effects of ozone have generally been associated with summer levels.
PNC was measured in all cities with identical condensation particle counters (TSI model 3022) over a three year period.16 We constructed models to estimate PNC using available data on other air pollutants and meteorological variables.17 The models were then applied to predict retrospectively daily PNC levels.
Data analysis
We analysed data using Poisson regression. For estimation of possible non-linear effects of confounders we used penalised splines in generalised additive models.22 We selected potential confounders based on the literature on triggering of AMI. For barometric pressure, the current-day value was used. Instead of measured temperature we used apparent temperature, which is an index of perceived temperature combining temperature and humidity, the former dominating the value.23 In particular, the health effects of hot weather conditions may not be well represented by using air temperature. Separate terms were used for immediate effects and more lagged effects:24 current-day average apparent temperature for the immediate effect, and the difference between current-day average apparent temperature and the three previous days’ average apparent temperature for slower effects. The shapes of the smooth terms for trend, temperature, and barometric pressure were judged one by one. The smoothing parameters were chosen to minimise the un-biased risk estimator (UBRE) score for the model using the magic fit method (the R package mgcv 0.9–5).
We built the basic model without air pollution in strict stepwise order starting with a model including time trend, current-day mean apparent temperature, weekday, holiday (national), and population reduction (due to summer holidays). Next we added terms for the lagged effect of temperature and barometric pressure one at a time. We based inclusion of these confounders on estimated degree of freedom, confidence bands, and UBRE score.22 Finally, factors for holidays and population reduction were removed if not needed based on statistical significance and UBRE score.
The main analyses were limited to short lags (days 0–3); lags until day 5 were used for descriptive purposes. Lag 0 was defined as the average air pollution level on the event day, lag 1 represented the level on the day before, and so on.
If the city-specific estimates were not significantly heterogeneous (p<0.1),25 we calculated a pooled effect estimate as the weighted average of city-specific regression coefficients using the inverse of the squared standard errors of the regression coefficients as weights. When the estimates were heterogeneous, we used a random effects approach. We calculated pooled results for PM10 for an increase of 10 μg/m3 in order to be comparable to previous studies. Results for other pollutants have been calculated for an increase of study mean IQR multiplied by the ratio between 10 μg/m3 and the PM10 IQR in the study. Two-pollutant models were used to evaluate the effects of PNC while considering O3 and PM10.
We considered age, fatality, and season as possible effect modifiers. We stratified data at the same time for age and fatality as they are potentially related. Stratified analyses were restricted to the three centres with HDRs, where data contained information also on persons aged >75 years. We collected data on deaths in Helsinki and Stockholm from national registers, and in Rome from municipal registers. AMI hospitalisation was categorised as fatal when death occurred within 28 days from hospitalisation. We also conducted stratified analyses by warm and cold season.
As an alternative smoothing approach, we used natural b-splines in generalised linear models.26 We tested the sensitivity of results to modelling of temperature by using the average of 1–3 day lagged temperature as a term for delayed temperature effect. We evaluated the impact of selection of confounders by excluding/including confounders that were of borderline significance (p<0.2) in the original basic model. Finally, we checked the effect of high pollution days by restricting the analyses to the days below the 98th percentile of the concentration distribution.
RESULTS
Altogether, 26 854 individuals were hospitalised during the study period (table 1). The number of admissions was clearly higher in the three centres where large HDRs were used than in the two centres with AMI registers. In the latter, there were high proportions of men, due mainly to the upper age limits set by the registers.
Modelled particle number concentrations were clearly highest in Barcelona, followed by Rome (table 2). CO and NO2 levels and warm season O3 levels were highest in Rome. CO levels, as well as PM10 levels, were lowest in the far northern cities Helsinki and Stockholm.
Daily air pollution levels and apparent (perceived) temperature*
Modelled PNC correlated most strongly with NO2 and CO in Augsburg, CO in Barcelona and Rome, and NO2 in Helsinki and Stockholm (table 3).
Spearman’s correlation coefficients between air pollutants and measured temperature
When we pooled the results from all the five cities together, we found at 0 day lag a suggestive association of CO and PNC with first AMI hospitalisations (table 4). When we restricted analyses to the three cities where large HDRs were used, we found marginally stronger associations of CO and PNC with AMI. The effects were homogeneous between cities at lag 0. Pooled estimates at 1 and 3 day lags for CO and PNC were heterogeneous. Results for maximum 8 h CO and 1 h NO2 did not differ from the results obtained using the daily averages (data not shown). Ozone was not associated with AMI, and including ozone in the same model with PNC did not affect the results for either. Thus, stratified analyses have been conducted without ozone. In a two-pollutant model including PNC and PM10, pooled rate ratios (95% CI) for PNC remained essentially the same in the five cities, but decreased for PM10 to 0.999 (0.990–1.009) at lag 0, and increased to 1.006 (0.996–1.015) at lag 3.
Pooled rate ratios (RRs) and 95 % confidence intervals (95% CIs) for the associations of daily air pollution levels with hospitalisation for first acute myocardial infarction
The heterogeneity in the pooled estimates was mainly caused by differences between cities in lag times. The lag structure for PNC in the five cities has been plotted in figure 1. PNC seemed to have an immediate effect in Rome, data of which drove the pooled results at 0 day lag. In Helsinki, the effects were most pronounced at lag 1 and in Stockholm at lag 3. PNC had no clear association with AMI in the two cities with AMI registers, where the smaller data set resulted in larger confidence intervals.
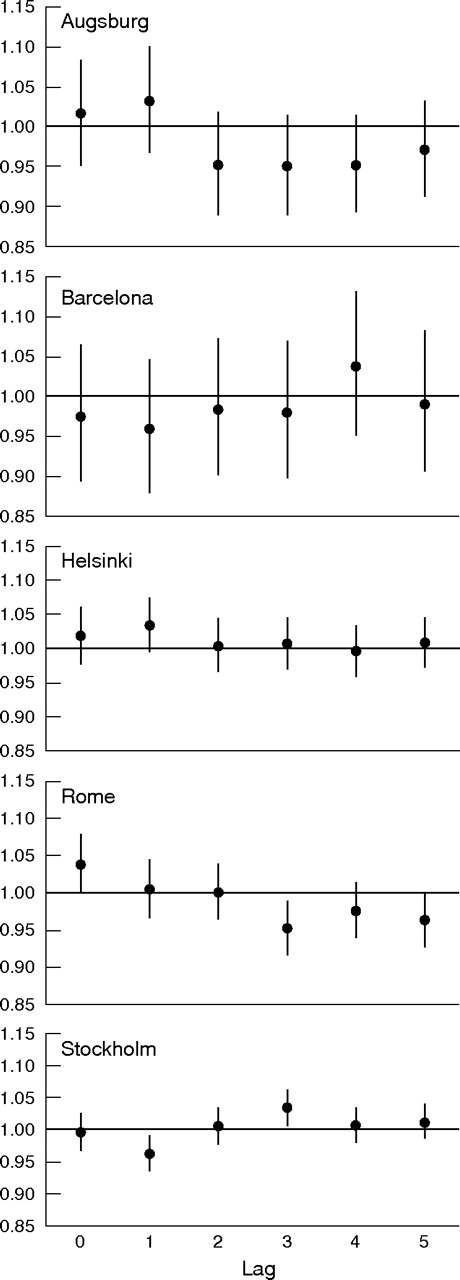
Rate ratios (RR; dots) and 95% confidence intervals (95% CI; vertical lines) based on single-day lag models with increasing lags for the association of particle number concentration (PNC) with hospitalisations for first acute myocardial infarction. RRs calculated for city-specific interquartile increases in PNC.
In the sensitivity analyses, only the exclusion of extreme concentrations had any effect on the associations of PNC and CO with first AMI. The pooled rate ratio (five cities) for PNC at 0 day lag decreased to 1.002 (95% CI 0.991 to 1.014), and confidence intervals for the association of CO with AMI got wider: 95% CI 0.984 to 1.030 (RR = 1.007). When we pooled results of only the three cities with HDRs, the association between PNC and AMI at 0 day lag became weaker, 1.005 (95% CI 0.990 to 1.021), whereas the association for CO got clearly stronger, 1.042 (95% CI 1.009 to 1.077), after exclusion of extreme values.
In Helsinki, Rome, and Stockholm, there were altogether 5158 fatal AMI hospitalisations. Among persons below 75 years of age, 12.8% of the hospitalisations were fatal, whereas 33.1% of them were fatal among persons aged 75 or above. AMI was consistently associated with PNC and CO among fatal AMI cases below 75 years of age (table 5). In the stratum, there was evidence also on the associations of PM10 and NO2 with AMI, and any pooled results were no longer significantly heterogeneous. Figure 2 illustrates how the stratification affected the lag structure for PNC and consequently decreased heterogeneity between cities. Among non-fatal cases aged 75 or above, we observed associations of the same day PNC and CO levels with AMI (table 5).
Pooled rate ratios (RRs) and 95 % confidence intervals (95% CIs) for the associations of daily air pollution levels with hospitalisation for first acute myocardial infarction by age and fatality in the three cities with hospital discharge registers

{kind=link}
{kind=link}
Rate ratios (RR; dots) and 95% confidence intervals (95% CI; vertical lines) based on single-day lag models with increasing lags for the association of particle number concentration (PNC) with fatal hospitalisations for first acute myocardial infarction among persons <75 years of age in the three cities with hospital discharge registers. RRs calculated for a change of 10 000/cm3 in PNC.
In Helsinki, Rome, and Stockholm, there were altogether 11 015 AMI hospitalisations during the warm season and 12 712 during the cold season. Rate ratios for the associations of CO, NO2, PNC, and PM10 with AMI were higher during warm season than cold season (table 6). There was no significant heterogeneity in effect estimates between cities when data were restricted to warm season. Strongest associations were observed at lag 0 during the cold season, but at higher lags during the warm season.
Pooled rate ratios (RRs) and 95 % confidence intervals (95% CIs) for the associations of daily air pollution levels with hospitalisation for first acute myocardial infarction by season in the three cities with hospital discharge registers
DISCUSSION
The pooled results of the five European cities suggest a weak association of CO and PNC with AMI hospitalisations. Stronger associations were observed in the three cities that used large HDRs. Among these cities there was considerable variation in the lag times of air pollution effects. Less heterogeneous results and higher effect estimates were obtained in stratified analyses, where the associations of CO and PNC with AMI were most consistent among fatal cases (28 day fatality) <75 years of age, and during warm season.
The five cities in our study reflect different demographics, climates, and air pollution sources encountered within the European Union. In the current study, the focus was on air pollutants originating mainly from traffic in urban environments. The pooled results of the five cities suggest a weak association of CO and PNC with AMI. However, in Augsburg and Barcelona, CO and PNC were not associated with AMI. This is probably due to lower power for city-specific analyses in these cities. In the three cities with large HDRs, there was considerable heterogeneity in results. However, the heterogeneity was reduced in stratified analyses leading to higher pooled effect estimates and providing further support for the association between the pollutants and AMI.
Many recent studies support the importance of traffic and other combustion processes as the major source of harmful particulate matter.9,10 CO and PNC both originate from combustion processes, mainly traffic in most urban environments. It is known that exposure to CO may aggravate myocardial ischaemia by reducing the oxygen carrying capacity of blood by binding to haemoglobin, and occupational studies have suggested an association between ischaemic heart disease mortality and CO exposure.27 However, given the very low ambient levels of CO in especially Stockholm and Helsinki a causal role of CO is not likely in the current study, but CO has probably acted as a proxy for traffic related particulate pollution. It has been shown that outdoor CO levels may serve as surrogates for exposure to PM2.5, and may be poorly correlated with CO exposures.28 On the other hand, PNC might be also causally related to AMI.8
Our findings are in line with the few smaller scale studies that have evaluated associations between occurrence of AMI and traffic related air pollution. D’Ippoliti et al found CO and NO2 to be positively associated with AMI hospitalisations in Rome, but the strongest association was observed between total suspended particles and AMI.3 Peters et al found daily levels of both particles and gaseous pollutants to be associated with the onset of non-fatal AMI in Boston.4 In a recent similar study in Augsburg,29 the results for daily air pollution concentrations were essentially the same. PNC was included in the latter study, but no association with AMI was found.
In our study the effects of PM10 were less clear than those of CO and PNC. The percentage increase in AMI hospitalisations for a 10 μg/m3 increase in PM10 was also lower than in a recent large study on AMI in the US: 0.3% versus 0.65%.5 However, especially in stratified analyses PM10 seemed to have an effect in the current study, too. It should be noted that the use of a few central outdoor monitors makes the comparison of effect estimates of pollutants from different sources difficult. It is likely that also in our study, for example, the spatial variability in PM10 levels has been different from the variability of more obviously traffic related pollutants like PNC and CO. However, in time series analyses the spatial variability in pollutant levels is less of a problem than possible poor temporal correlation between sites. For PM2.5 it has been shown that the levels of traffic originating mass might be very different at different sites, but still longitudinally correlating.30 We have shown in the HEAPSS study fair correlation between two monitoring sites for PNC in Barcelona, Rome, and Stockholm.16 In Helsinki, rather high longitudinal correlations have been previously reported for several monitoring sites for PNC.31 Part of the exposure to traffic originating pollutants obviously occurs while outdoors and in traffic. As the study population consisted mainly of elderly persons, the time spent outdoors has probably been lower than for general population.
We found PNC and CO to be more strongly associated with AMI among fatal cases below 75 years of age than in the whole data. In this category, there was also some evidence of PM10 and NO2 effects. In the higher age group, we observed air pollution effects mainly among non-fatal cases. Persons ⩾75 years of age within the fatal category may be so frail that the effects of air pollution are masked by factors related, for example, to multiple comorbidities. It should also be noted that the fraction of fatal AMIs never reaching the hospital is dependent on age.32,33 Within the HEAPSS study, we have observed strong associations of out-of-hospital coronary deaths with PNC, PM10, and CO in Rome.13
We observed higher pooled effect estimates for air pollution during warm season than during cold season. This is consistent with a recent large American mortality study,34 and could be due to higher exposure or better exposure assessment during the warm season because of larger proportion of time spent outdoors and higher ventilation rates. On the other hand, seasonal differences in air pollution mixture may also affect the effect estimates, and could explain the seasonal differences in lag structure. Taken together, our two types of stratified analyses demonstrate how straightforward pooling of effect estimates in multicity studies may conceal inherent differences between cities in climate, air pollution mixture, and population. One potentially important effect modifier is medication—for example, the use of statins and beta-blockers,35,36 which might differ between cities. Unfortunately, HDRs do not include data on medication.
Recently, an association between ozone and AMI was reported in Toulouse, but no association between AMI and NO2 or SO2.37 Thus, we decided to study the possible effects of ozone in addition to the effects of closely traffic related pollutants. However, we could not confirm the finding, as O3 was found not to be associated with AMI.
An obvious limitation in our study is the use of two different types of registers for the collection of AMI data. Nevertheless, the different practices of AMI diagnosis and registration are probably a minor limitation. Instead, the upper age limit of the AMI registers may be more problematic since it caused not only different age structure, but also different sex structure as compared to the cities with administrative hospital databases. In any case, the small number of cases alone might explain the lack of associations in Augsburg and Barcelona.
Particle number concentrations were not measured directly, but estimated using other pollutants and meteorology. We have demonstrated that the estimated concentrations correlate well with measured concentrations.17 However, due to uncertainties associated with retrospective modelling in general, the effect estimates of CO and PNC are not directly comparable. In the future, when more measurement data on the smallest fractions of particles accumulate in the five study centres and elsewhere, measured PNC can be used.
Main messages
-
Exposure to traffic related air pollution may increase the risk of first myocardial infarction.
-
In multicity air pollution studies on hospitalisations for myocardial infarction and other cardiovascular diseases, case fatality, age of patient, and season should be considered.
Policy implications
-
The results help the European Union and national institutions to design policies for air pollution abatement.
-
Efforts to reduce population exposure to traffic originating pollution to reduce the human and economical costs paid for air pollution should be continued both in Southern and Northern Europe.
In summary, we found support for the hypothesis that exposure to traffic related air pollution increases the risk of AMI. The associations of CO and modelled PNC with AMI were most consistent among fatal hospitalised AMI patients below 75 years of age and hospitalised AMI patients 75 years of age or older with non-fatal outcome. Associations were also stronger during the warm season than the cold season. The causal factor or factors remain to be identified
Acknowledgments
The study was funded by European Union (QLK4-2000-00708). In Finland, the study was also financially supported by the Centre of Excellence Programme 2002–2007 of the Academy of Finland (Contract 53307) and the National Technology Fund (TEKES, Contract 40715/01). The funding sources had no role in design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript. Fredrik Nyberg, employed by AstraZeneca, is also Lecturer in Epidemiology at Karolinska Institutet. AstraZeneca did not contribute any direct financing to this study. Dr Peters was partially supported by the US Environmental Protection Agency STAR center grant R-827354. Finnish patient data were provided by the National Research and Development Centre for Welfare and Health, and vital status was ascertained using the mortality register at Statistics Finland. German data were provided by the GSF-Research Center of Environmental and Health funded by the German Ministry of Research and Science and the State of Bavaria. Swedish patient data were provided by Statistics Sweden and the Swedish National Board of Health and Welfare.
REFERENCES
Footnotes
-
Published Online First 15 August 2006
-
Competing interests: none.
-
Full list of the HEAPSS study group. Italy: Forastiere F, D’Ippoliti D, Michelozzi P, Perucci CA, Picciotto S, Stafoggia M, Accetta G, Compagnucci P, Cattani G, Marconi A; Germany: Peters A, von Klot S, Löwel H, Hörmann A, Meisinger C, Cyrys J, Greschik C, Zetsche K, Harmath C, Kühner N, Kaup U, Schuler A, Lutkitsch D, Winter C, Orlik G, Zimmermann G, Pitschi P, Schnelle-Kreis J; Spain: Sunyer J, Marrugat J, Elosua R, Gil M, Sanz G, Molina L, Valle V, Julvez J, Rebato C, Cabañero M, Muñoz L; Finland: Pekkanen J, Lanki T, Tiittanen P, Salomaa V, Kokki E, Koskentalo T, Kulmala M, Aalto P, Paatero P, Hämeri K; Sweden: Nyberg F, Berglind N, Bellander T, Pershagen G, Bessö A, Sjövall B, Jonsson T, Johansson C, Köster M.