


- © 2007 Canadian Medical Association
Abstract
Background: Mortality associated with colorectal cancer can be reduced by early detection. However, the participation of eligible people in colorectal cancer screening is thought to be inadequate. We examined the frequency of colorectal cancer screening in 4 Canadian provinces and the influence of patient contact with a family physician on the uptake of cancer screening.
Methods: We performed analyses using data from the 2003 Canadian Community Health Survey. The study population included 12 776 people at average risk for colon cancer living in British Columbia, Saskatchewan, Ontario, and Newfoundland and Labrador who were aged 50 years or older and who were eligible for colorectal cancer screening. We assessed the proportion of respondents who reported having previous colorectal cancer screening tests and the degree of contact with a family physician.
Results: The provincial response rates for the survey were 78.5%–87.0%. The proportion of respondents who reported any history of colorectal cancer screening was 23.5%. This value dropped to 17.6% when only up-to-date screening was considered (screening within the time frame recommended in guidelines). The proportion of people with up-to-date colorectal cancer screening varied significantly among provinces, but it was low in all provinces sampled. Contact with a family physician was associated with increased colorectal cancer screening. Compared with no physician contact, the odds of screening associated with 1–2 physician contacts in the 12 months before the survey was 1.97 (95% confidence interval [CI] 1.56–2.48], and the odds of screening associated with more than 4 contacts was 2.75 (95% CI 2.14–3.53).
Interpretation: Self-reported colorectal cancer screening falls well below acceptable levels. People with increased contact with a family physician are more likely than those without contact to report a history of up-to-date colorectal cancer screening.
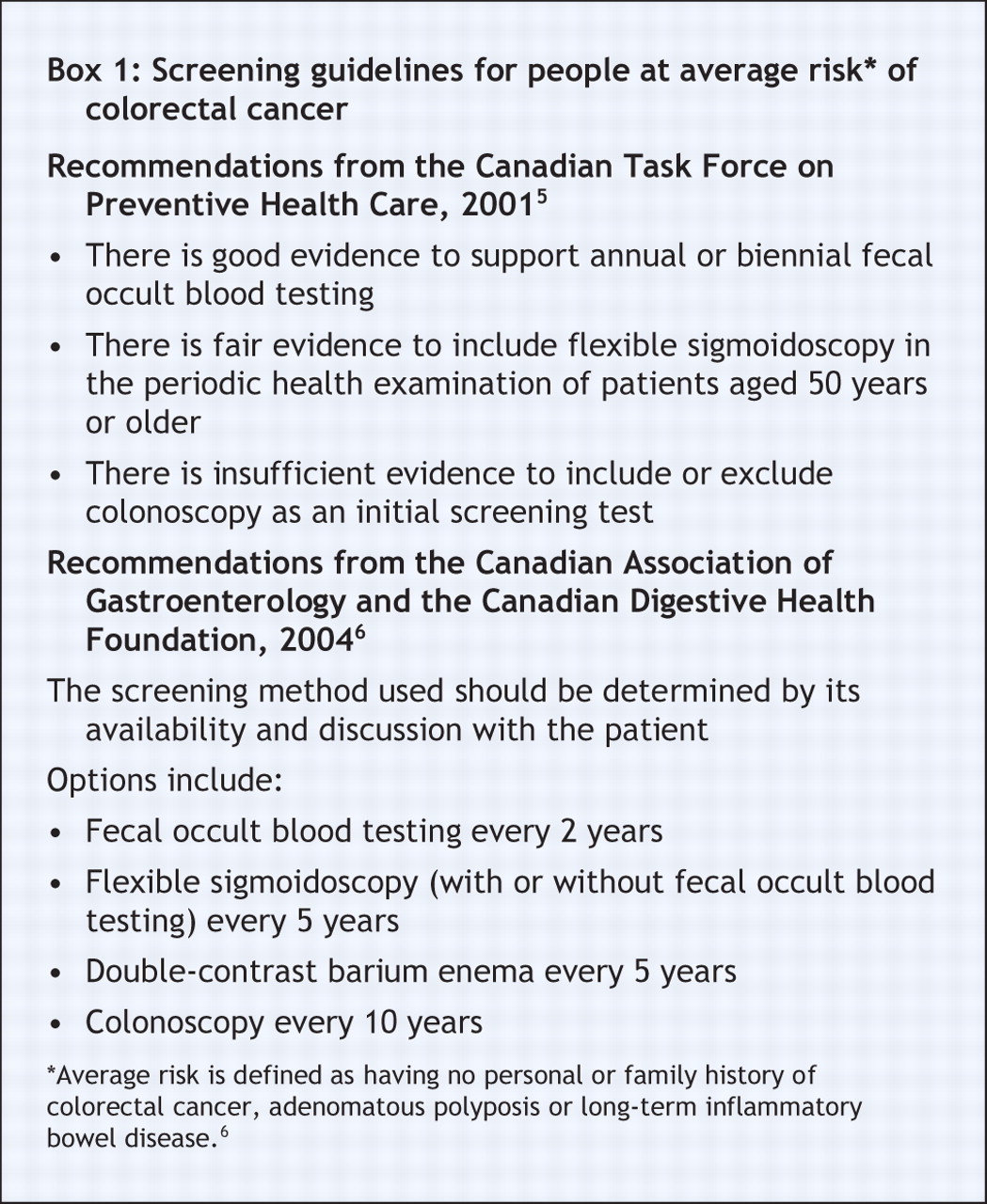
Colorectal cancer is the second leading cause of cancer-related deaths in Canada. In 2006 in Canada, there were an estimated 20 000 newly diagnosed cases of and 8500 deaths from colorectal cancer.1 Several randomized controlled trials and case–control studies have shown that colorectal cancer screening, either by fecal occult blood testing or by sigmoidoscopy, decreases mortality.2–4 Population screening for colorectal cancer has been recommended by the Canadian Task Force on Preventive Health Care since 2001.5 According to the Canadian recommendations, people at average risk who are 50 years of age or older should have an annual or biennial fecal occult blood test or should undergo periodic flexible sigmoidoscopy (Box 1).5 (Appendix 1 lists US recommendations, available at www.cmaj.ca/cgi/content/full/177/6/593/DC2).

Despite the high incidence and mortality associated with colorectal cancer and the known survival benefits associated with population screening, colorectal cancer screening remains inadequate. Before the 2001 Canadian task force recommendations, the proportion of eligible people who received colorectal cancer screening in Ontario was less than 25%.7,8 National estimates have not been published. In Canada, the primary access point to preventive services such as immunization and cancer screening is the family physician. One would expect that contact with a family physician would increase participation in colorectal cancer screening programs; however, this assumption has not been formally evaluated.
We sought to determine the extent of participation of eligible people in colorectal cancer screening programs in 4 Canadian provinces. We also examined the relation between contact with a family physician and the uptake of colorectal cancer screening.
Methods
Study population
The analyses for this study were based on data from the 2003 Canadian Community Health Survey, cycle 2.1,9 which was conducted by Statistics Canada. The target population of this cross-sectional survey was people aged 12 years or older who were living in private dwellings in Canada. People who lived on First Nations reserves, people who were full-time members of the Canadian Armed Forces, people in institutions, homeless people and people living in remote regions were excluded from the survey.
A multistage, stratified sampling design was used, with each dwelling as the final sampling unit. Demographic data were obtained for 144 836 households, and 1 or 2 people per household were asked to complete an in-depth interview. From this sample, 134 073 individual responses were obtained, giving a national response rate of 80.7%. The survey included questions related to health status, health care use and health determinants.
From the survey database, we identified people aged 50 years or older who had been administered an optional survey module addressing colon cancer screening. The provinces that participated in this module were British Columbia, Saskatchewan, Ontario, and Newfoundland and Labrador. In the colon cancer screening module, respondents were provided with a brief description of fecal occult blood testing and were asked if they had ever had such a test. Respondents were asked when the test had been performed and the reason for the test. These questions were also asked for sigmoidoscopy/colonoscopy.
Exposure and outcome variables
Contact with a family physician was categorized by the number of times a respondent reported talking with a general practitioner (in person or on the phone) in the 12 months before the survey. We defined people at “average risk” as those with no personal or family history of colorectal cancer, adenomatous polyposis or long-term inflammatory bowel disease.6
We identified respondents as being screened if they were at average risk and reported having a previous fecal occult blood test or colonoscopy/sigmoidoscopy performed as part of a regular check-up or routine screening or in response to a person's age. We excluded people who reported such testing for “other reasons” or who had a personal or family history of colorectal cancer or inflammatory bowel disease. Up-to-date colorectal cancer screening was defined according to the Canadian Association of Gastroenterology Guidelines6 as fecal occult blood testing within the past 2 years or colonoscopy within the past 10 years (Box 1). Sigmoidoscopy and colonoscopy were combined in the source database, and therefore a 10-year expiry cut-off was applied for sigmoidoscopic screening. Data concerning barium contrast testing were not available.
Statistical analysis
We used univariable and multivariable logistic regression to examine the relation between contact with a family physician and colorectal cancer screening. An odds ratio greater than 1 signifies increased colorectal cancer screening compared with the referent group. In the models, records that contained missing data for any of the explanatory covariates listed in Appendix 2 (available at www.cmaj.ca/cgi/content/full/177/6/593/DC2) were deleted if they compromised greater than 5% of the available data. Records were also deleted if data appeared to be missing at random. Missing data for income adequacy (total houshold income given the number of occupants) were coded as a separate category. We estimated the model parameters using the method of maximum likelihood, and we compared nested models using the –2 log-likelihood test. We explored effect modification by testing 2-way interaction terms of physician contacts with other factors.
The Canadian Community Health Survey is a complex survey; thus, we weighted all point estimates to the populations in the 4 participating provinces based on the individual sampling weights.10 The sampling weight can be interpreted as the number of people that a respondent represents in the population. The mean age-specific design effect for the survey was considered in the variance estimations for both simple and regression analyses.10
Results
The study population included 12 766 survey respondents from British Columbia, Saskatchewan, Ontario, and Newfoundland and Labrador. This sample represented 1 910 116 people aged 50 years or older who were at average risk for colorectal cancer. Of the respondents, 50.3% were men. The population of the provinces sampled represents 56.7% of the target (Canadian) population. The response rates to the provincial survey varied from 78.5% to 87.0%.
The majority (94.1%) of people reported having a regular medical doctor, and physician contact increased proportionally with age (Appendix 2, available at www.cmaj.ca/cgi/content/full/177/6/593/DC2). Of the respondents, 85.0% had spoken, in person or on the phone, with a family physician in the 12 months before the survey, and the median number of contacts was 3 (quartiles 1, 5).
The proportion of respondents who reported any history of colorectal cancer screening was 23.5% (2987/8980). This value decreased to 17.6% (2209/9749) when only up-to-date screening was considered (Table 1). Contact with a family physician increased colorectal cancer screening: 17.7% of respondents who reported having 1–2 contacts with a family physician in the 12 months before the survey reported having colorectal cancer screening, as compared with 8.8% of those who reported no contacts. Of the respondents who reported having more than 4 contacts, 20.9% reported having colorectal cancer screening.
Table 1.
The proportion of people who reported up-to-date colorectal cancer screening was highest in Ontario (20.0%) and lowest in Newfoundland and Labrador (12.6%) (Figure 1). The proportions in British Columbia and Saskatchewan were 16.5% and 17.0% respectively.
Regression modeling demonstrated a dose-dependent increase in colorectal cancer screening with self-reported contact with a family physician. Compared with no contact, the OR associated with colorectal cancer screening among respondents with 1–2 contacts in the 12 months before the survey was 1.97 (95% confidence interval [CI] 1.56–2.48) (Figure 2). Among people who reported more than 4 contacts, the OR associated with colorectal cancer screening was 2.75 (95% CI 2.14–3.53). In a separate model that adjusted for the same covariates, having a regular medical doctor was strongly associated with colorectal cancer screening (OR 3.57, 95% CI 2.33–5.47).
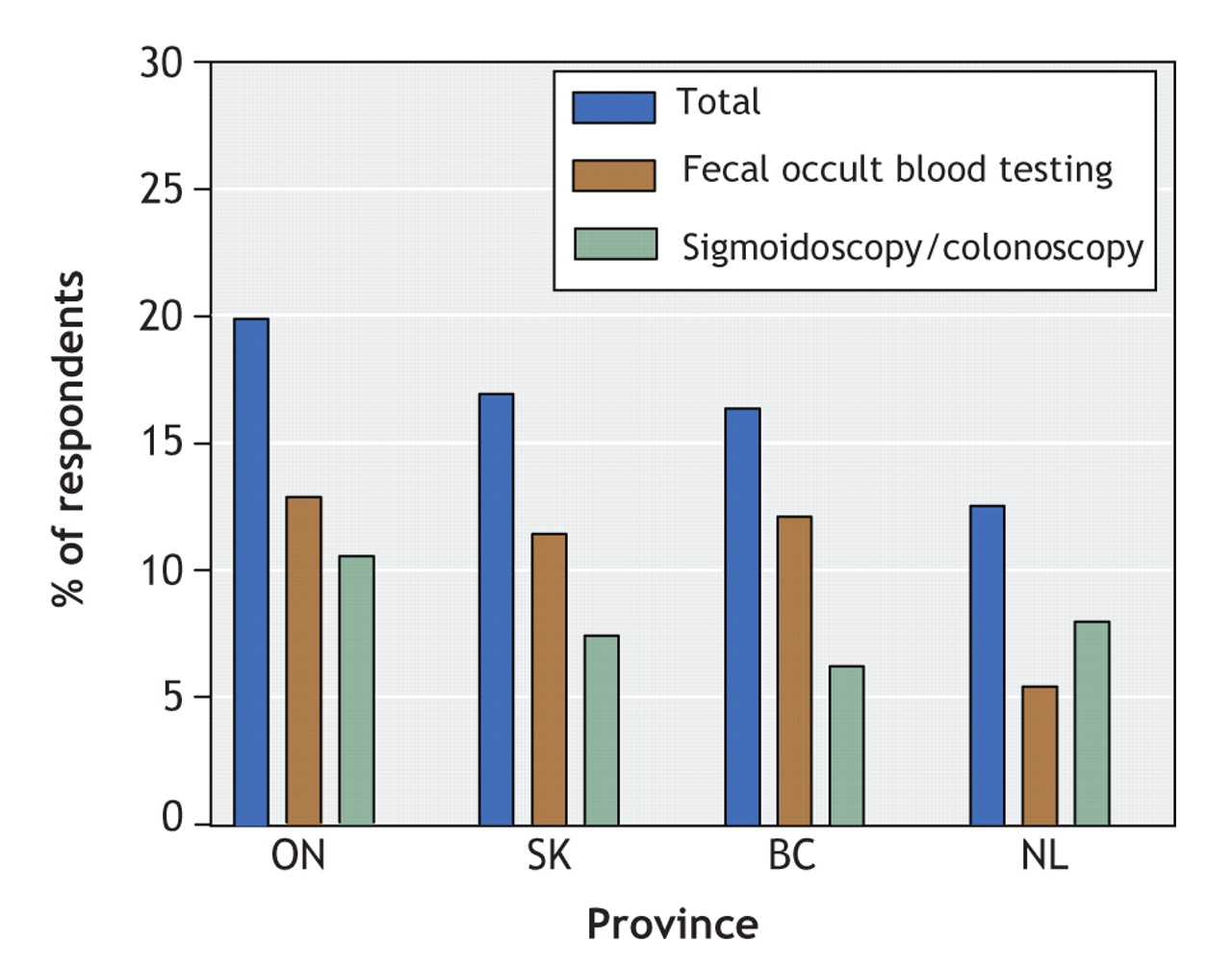
Figure 1: Proportion of survey respondents who reported up-to-date colorectal cancer screening by Canadian province.
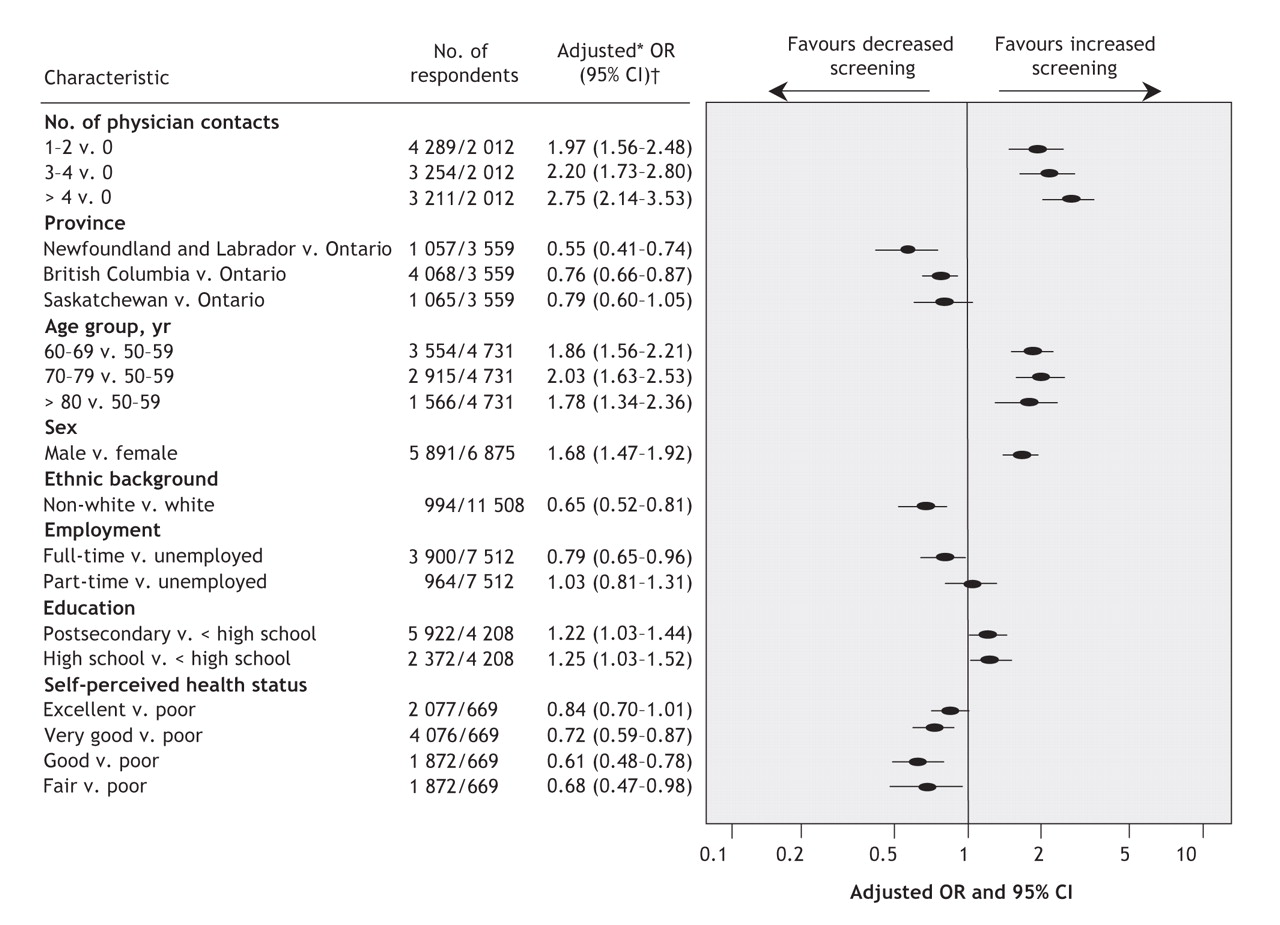
Figure 2: Analysis of factors associated with up-to-date colorectal cancer screening. *Adjusted for number of contacts, age, sex, employment, education, income, self-perceived health status, ethnic background and province. †Weighted to the Canadian population. Note: OR = odds ratio, CI = confidence interval.
The relation between other predictor variables and up-to-date colorectal cancer screening is shown in Figure 2. Older age, compared to respondents aged 50–59, was associated with increased colorectal cancer screening. The OR associated with colorectal cancer screening among men was 1.68 (95% CI 1.47–1.92), despite the fact that a greater proportion of women had increased contact with a family physician. Full-time employment was associated with a 20% decrease in the odds of colorectal cancer screening. Higher education (postsecondary education v. not completed high school, completed high school v. not completed high school) was associated with increased odds of screening. In the final model, individual categorical strata of income adequacy were not significant. Compared with white respondents, more non-white respondents reported increased contact with a family physician. However, being non-white was associated with decreased odds of up-to-date colorectal cancer screening (OR 0.65, 95% CI 0.52–0.81).
Significant variation in the number of people who reported receiving colorectal cancer screening persisted between provinces after adjustment for multiple potential confounders (Figure 2). The odds associated with up-to-date colorectal cancer screening in British Columbia and in Newfoundland and Labrador were statistically lower than in Ontario.
Interpretation
We found that an exceptionally low proportion (17.6%) of eligible Canadians reported having received colorectal cancer screening within the recommended time frame. The proportion varied significantly among provinces, but it was low in all of the provinces sampled. Increased self-reported contact with a family physician was associated with an increased likelihood of colorectal cancer screening. However, even among patients who reported more than 4 physician contacts in the 12 months before the survey, up-to-date colorectal cancer screening was reported by only one-fifth of the respondents. Fewer women than men, and fewer non-white than white respondents, reported receiving colorectal cancer screening. However, women and non-white respondents reported having more contact with physicians.
From 1995 to 2000, administrative and billing data indicate that less than 20.5% of Ontario residents aged 50–59 years were screened for colorectal cancer.7 In an Ontario survey8 performed during 1998–2000, 23% of respondents aged 50 years or older reported ever receiving colorectal cancer screening.Despite the current evidence and the publication of the recommendations of the Canadian Task Force on Preventive Health Care in 2001, our study suggests that participation in colorectal cancer screening programs is essentially unchanged.
Participation in colorectal cancer screening and the development of organized screening programs varies widely between regions and countries. In Canada, several provinces have announced colorectal screening programs, but no national strategy exists. In the United States, screening programs exist, but they vary considerably in terms of coverage and completeness.11 About 15% of Americans aged 50 years or older have undergone fecal occult blood testing for screening purposes and almost 21% have undergone endoscopy.12 In the United Kingdom, a nationally administered colorectal screening program and a recall system have recently been instituted. Pilot data from this program indicate uptake of almost 60%.13 Similar to the pilot program underway in Manitoba, in the United Kingdom people receive kits for fecal occult blood testing directly by mail instead of having to obtain them from a family physician.
The majority of physicians recommend screening for adults at average risk of colorectal cancer, and physicians themselves actively participate in screening.14,15 A recent Canadian survey found that 53% of physicians had undergone colorectal cancer screening and that 56% of all physicians and 91% of gastroenterologists chose to be screened by colonoscopy.15 In a separate Canadian study, 70% of physicians reported that colonoscopy was the only screening test that they themselves would undergo or recommend to their patients.16 Screening guidelines and approaches must evolve if specialists are choosing one modality when the official guidelines recommend another. This dichotomy may be confusing to family physicians, and it is likely to compromise the clarity and completeness with which they pursue colorectal cancer screening for their patients.
Our study has several limitations. It is based on self-reported data; thus, it is vulnerable to factors such as recall and misclassification bias. We feel that it is unlikely that respondents would systematically forget receiving fecal occult blood testing or sigmoidoscopy/colonoscopy, given the level of participation that these tests require. Self-reporting of colorectal cancer screening has been shown to provide accurate and reliable estimates of previously performed interventions.17 Our results for Ontario are also remarkably consistent with previously published analyses.7,8 Physician contact in this study included both visits and telephone calls. Although these methods of contact are unlikely to represent equivalent screening opportunities, this limitation is unlikely to cause bias in the overall findings of this study. Participation in colorectal cancer screening remained low over a range of physician contacts.
In conclusion, the proportion of people at average risk who reported having colorectal cancer screening in Canada is exceptionally low. This is true despite published guidelines and a widespread belief among physicians that screening for colorectal cancer is worthwhile. Contact with a family physician increases the odds of screening.
@ See related article page 545
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/177/6/593/DC1
This article has been peer reviewed.
Contributors: All of the authors contributed to the study conception and design and the interpretation of the results. Ryan Zarychanski and Yue Chen performed the data analyses. Ryan Zarychanski wrote the manuscript, and all of the authors revised it for important intellectual content. All of the authors approved the final version submitted for publication.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Assessing the impact of colonoscopy complications on use of colonoscopy among primary care physicians and other connected physicians: an observational study of older Americans
- Screening rates for colorectal cancer in Canada: a cross-sectional study
- Non-Visit-Based Cancer Screening Using a Novel Population Management System
- Colorectal cancer screening practices in Saskatchewan: Survey of family physicians
- Feasibility of a call-in centre to deliver colorectal cancer screening in primary care
- Cancer screening practices of cancer survivors: Population-based, longitudinal study
- Use of an elastic stain to show venous invasion in colorectal carcinoma: a simple technique for detection of an important prognostic factor
- Provincial primary care and cancer engagement strategy
- Outcomes of 1949 endoscopic procedures: Performed by a Canadian rural family physician
- Asia Pacific consensus recommendations for colorectal cancer screening
- Rates of colorectal cancer screening
- Perception versus reality: Overcoming barriers to colorectal cancer screening
- Colorectal cancer screening
- Colorectal cancer screening
- Colorectal cancer screening
- Survivre au cancer colorectal
- Outliving colorectal cancer
More in this TOC Section
Similar Articles
Collections

