Advances in optimizing the prescription of antibiotics in outpatient settings
BMJ 2018; 363 doi: https://doi.org/10.1136/bmj.k3047 (Published 12 November 2018) Cite this as: BMJ 2018;363:k3047
- Laura M King, health research analyst1,
- Katherine E Fleming-Dutra, deputy director1,
- Lauri A Hicks, director1
- 1Division of Healthcare Quality Promotion, National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention, Mailstop H16-3, Atlanta, GA, 30329, US
- Correspondence to: K E Fleming-Dutra ftu2{at}cdc.gov
Abstract
The inappropriate use of antibiotics can increase the likelihood of antibiotic resistance and adverse events. In the United States, nearly a third of antibiotic prescriptions in outpatient settings are unnecessary, and the selection of antibiotics and duration of treatment are also often inappropriate. Evidence shows that antibiotic prescribing is influenced by psychosocial factors, including lack of accountability, perceived patient expectations, clinician workload, and habit. A varied and growing body of evidence, including meta-analyses and randomized controlled trials, has evaluated interventions to optimize the use of antibiotics. Interventions informed by behavioral science—such as communication skills training, audit and feedback with peer comparison, public commitment posters, and accountable justification—have been associated with improved antibiotic prescribing. In addition, delayed prescribing, active monitoring, and the use of diagnostics are guideline recommended practices that improve antibiotic use for some conditions. In 2016, the Centers for Disease Control and Prevention released the Core Elements of Outpatient Antibiotic Stewardship, which provides a framework for implementing these interventions in outpatient settings. This review summarizes the varied evidence on drivers of inappropriate prescription of antibiotics in outpatient settings and potential interventions to improve their use in such settings.
Introduction
Antibiotics are life saving drugs that have enabled many advances in modern medicine. However, the more that antibiotics are used, the less effective they become. Antibiotic resistance is an important global threat to public health.1 In addition, antibiotics are associated with adverse events ranging from mild gastrointestinal distress to life threatening Clostridium difficile infections. Antibiotic stewardship is the measurement and optimization of antibiotic use. It includes ensuring that antibiotics are given only when necessary and beneficial, and that the right agent, dose, and duration of treatment are used. Antibiotic stewardship also emphasizes that, when antibiotics are needed, such as when sepsis is suspected, they should be started promptly. The goal of antibiotic stewardship is to optimize patient safety and outcomes.
Globally, 85-95% of all antibiotics for humans are prescribed in outpatient settings, including physicians’ offices, urgent care facilities, retail health clinics, and emergency departments.23 In 2015, in the United States, enough antibiotic prescriptions were dispensed in the outpatient setting for five out of every six people to receive a course of antibiotics.4 Until recently, much of the focus on antibiotic stewardship has been in hospitals. However, there has been a recent surge of research in outpatient settings and, in 2016, the US Centers for Disease Control and Prevention (CDC) published the Core Elements of Outpatient Antibiotic Stewardship5 (fig 1) to provide a framework for US outpatient clinicians and facilities to improve antibiotic use.

Essentials of the Core Elements of Outpatient Antibiotic Stewardship.5 Figure courtesy of the US Centers for Disease Control and Prevention
{kind=link}
The aim of this review is to synthesize the growing literature examining the causes of inappropriate antibiotic prescribing and potential antibiotic stewardship interventions in outpatient settings. To contextualize this literature, our review also provides a brief overview of the consequences and epidemiology of outpatient antibiotic prescribing.
Sources and selection criteria
The references for this review were identified through PubMed searches, the authors’ libraries, and reference lists from CDC publications. Our PubMed search was limited to English language publications published in peer reviewed journals from January 2012 to November 2017. Search terms included “antimicrobial stewardship” AND “outpatient”, “antimicrobial stewardship” AND “primary care”, and “antimicrobial stewardship review”. We reviewed relevant titles and abstracts from this search and included meta-analyses, systematic reviews, randomized controlled trials (RCTs), and large descriptive and observational studies. When those types of studies were limited or when other study types yielded richer data—for example, when examining the drivers of inappropriate prescribing—we included qualitative and small observational studies. We included older (pre-2012) references from authors’ libraries and CDC reference lists if they were highly cited, complemented or contextualized recent studies, or if recent literature on the topic was limited. We also included relevant government documents and resources from authors’ libraries. We included studies from both US and non-US settings. When discussing drivers of inappropriate prescribing and potential interventions, we noted studies from outside the US. During the peer review process, two studies with new information on topics described here were published. Because of the novelty of the information in these studies and their relevance to this topic, we included them in this review.
By its nature, this narrative review may suffer from selection bias. We did not include gray literature or studies published in languages other than English, and we limited published studies to those available on PubMed or already in authors’ libraries. Thus, we may have omitted additional references that would have provided further insight.
Why the use of antibiotics in the outpatient setting needs to be improved
Resistance
The use of antibiotics selects for antibiotic resistant bacteria; antibiotic resistant organisms infect at least two million people, cause at least 23 000 deaths, and result in $20bn (£15.35bn; €17.25bn) in excess direct healthcare costs in the US each year.6 For some pathogens, such as carbapenem resistant Enterobacteriaceae, treatment options are becoming increasingly limited, increasing the risk of patient morbidity and mortality and treatment costs. The use of antibiotics is associated with resistance both at population and individual levels. Antibiotic resistance patterns for selected antibiotic-pathogen combinations have been seen to change in parallel with shifting antibiotic consumption patterns in a population.789 At the individual level, the odds of identifying antibiotic resistant bacteria (colonization or infection) are more than twice as high among people with recent antibiotic exposure compared with those who have not recently been exposed.10
Adverse drug events
Antibiotic associated adverse drug events are a threat to patient safety. Such events include gastrointestinal disturbances, nephrotoxicity, secondary infections (including yeast and C difficile infections), neurological or psychiatric effects, sensory or motor disturbances, and allergic reactions. The CDC estimates that one emergency department visit for an antibiotic associated adverse drug event occurs for every 1000 outpatient antibiotic prescriptions.11
C difficile infection is a life threatening antibiotic associated adverse drug event. C difficile caused an estimated 450 000 infections and 15 000 deaths in 2011 in the US.12 In 2015, estimated US annual acute care costs attributable to C difficile infection were $1.2bn-5.9bn.13 Antibiotic use is a well known risk factor for C difficile infection,14 and it is estimated that a 10% reduction in outpatient antibiotic prescription rates could result in a 17% decrease in C difficile infection rates.15 Reductions in specific antibiotics, such as fluoroquinolones and cephalosporins, are more likely to prevent C difficile infection.816
Certain antibiotics commonly used in outpatient settings are of special concern because they are associated with severe adverse drug events. Azithromycin is the most commonly prescribed antibiotic in outpatient settings,17 and it is often inappropriately prescribed for conditions for which it is not a recommended first line treatment or for which antibiotics are not indicated.18 In 2013, the US Food and Drug Administration (FDA) warned that azithromycin can lead to potentially fatal heart rhythm irregularities.19 Fluoroquinolones are also commonly used in outpatient settings, often inappropriately.20 In 2016, the FDA updated its warning on fluoroquinolones because they can have disabling and permanent side effects, including tendonitis, tendon rupture, worsening of myasthenia gravis, peripheral neuropathy, and central nervous system effects.21 The FDA recommended that fluoroquinolones should be avoided in acute sinusitis, acute bronchitis, and uncomplicated urinary tract infections.21
Effects on the microbiome
An emerging focus is the impact of antibiotics on the microbiome, the population of microorganisms in the body, and related effects on health. The use of antibiotics can result in loss of diversity and disturbances in the microbiome that can persist for years. Current evidence is limited, but it indicates that antibiotic use during early life may be associated with an increased risk of chronic diseases, such as juvenile idiopathic arthritis,22 celiac disease,23 inflammatory bowel disease,24 diabetes,25 and food allergies,26 probably as a result of disruption of the microbiome.27 Evidence suggests that increasing numbers of antibiotic courses in early life correspond with an increasing likelihood of developing these diseases.2223242526 In addition, the use of antibiotics in livestock growth promotion has prompted researchers to study the association between antibiotics and obesity in humans. Although nascent, many of the data on childhood antibiotic use and body mass, overweight, obesity, and weight gain show an association.282930313233 However, a recent observational study of more than 38 000 children followed to age 7 years found that the use of antibiotics within the first 6 months of life was not associated with later weight gain.34
Outpatient antibiotic prescribing in the US
National antibiotic prescribing
In 2015, 269 million antibiotic prescriptions, equivalent to 838 antibiotic prescriptions per 1000 population, were dispensed from US community pharmacies, making the outpatient setting an important target for improving the use of antibiotics.4 In fact, the US National Action Plan for Combating Antibiotic Resistant Bacteria, released in 2015, set a goal of reducing inappropriate antibiotic use in the outpatient setting by 50% by 2020.35 Inappropriate antibiotic use includes unnecessary use (using antibiotics for conditions for which they are not indicated) and suboptimal antibiotic selection, dosing, and course duration.
Using national outpatient prescribing data, we previously estimated that at least 30% of antibiotics prescribed in physicians’ offices and emergency departments in the US were unnecessary (table 1).37 Total inappropriate antibiotic use, including selection, dosing, and duration, is probably much higher. In outpatient settings, acute respiratory infections (ARIs) are major drivers of inappropriate antibiotic use. ARIs accounted for 44% of antibiotics prescribed in US physicians’ offices and emergency departments in 2010-11 and half of these prescriptions were unnecessary.37
Proportion of antibiotic prescriptions that were unnecessary, United States, 2010-11*
Antibiotic agent selection
The selection of antibiotics in accordance with guidelines is an important stewardship target because it can improve “drug-bug” matching and reduce side effects. A descriptive study using national prescribing data found that among the three most common conditions that antibiotics are prescribed for in the US—acute otitis media, sinusitis, and pharyngitis—guideline recommended first line antibiotics were prescribed in only 52% (95% confidence interval 49% to 55%) of visits.38 When drug allergies and treatment failures were accounted for, the authors estimated that at least 80% of visits should be treated with first line agents.38
Duration of antibiotic therapy
Shortening treatment to the minimum effective duration reduces antibiotic exposure and minimizes the risk of resistance and adverse events. Recent editorials have advocated for shorter courses of antibiotic treatment.394041 In the past, seven day, 10 day, or 14 day courses were the norm for many conditions. However, shorter durations have been shown to be equally effective in several conditions, including community acquired pneumonia,42434445 pyelonephritis,46 exacerbations of acute chronic obstructive pulmonary disease,47 and sinusitis.48 However, long courses are still more effective for acute otitis media in young children.49 High quality studies defining the minimum effective duration of antibiotic treatment for specific diagnoses and populations are needed. Little evidence exists on duration in actual outpatient prescribing. An exception to this is our descriptive study of more than 3.5 million estimated adult visits for sinusitis with an antibiotic prescription. We found that 66.9% (61.0% to 72.8%) of prescriptions were for 10 days, longer than the five day to seven day course recommended in guidelines for uncomplicated cases.50
Geographic and setting differences
Antibiotic prescribing rates in the US are highest in the south compared with other regions.17515253545556 There is also a trend toward higher antibiotic prescription rates in rural, compared with urban, areas.5357 The reasons for these geographic differences are not known. Prescribing also varies by outpatient setting. A descriptive study of a large convenience sample of employer group health insurance claims (N=156 015 899) found that antibiotic prescribing rates for respiratory conditions for which antibiotics were inappropriate were highest among urgent care clinics (45.7% of visits) compared with emergency departments (24.6%), physicians’ offices (17.0%), and retail clinics (14.4%).58
Reduced antibiotic prescribing in children
Progress has been made in the US. National antibiotic prescription data show that outpatient antibiotic prescription rates decreased by 4% between 2011 and 2015—from 877 prescriptions per 1000 population in 2011 to 838 prescriptions per 1000 population in 2015.59 This decline has been driven by reductions in prescribing to children. US antibiotic prescribing rates for children decreased by 13% from 2011 to 2015, while rates among adults remained stable (fig 2).59 The improvement in pediatric antibiotic prescribing is likely to be the result of several factors, including the introduction of the 13 valent pneumococcal conjugate vaccine,60 public health efforts to educate parents and health professionals, and clinicians’ efforts to change behavior.

Outpatient antibiotic prescription rates 2011-15. Data from the US Centers for Disease Control and Prevention’s Patient Safety Atlas (https://gis.cdc.gov/grasp/PSA/AUNational.html)59
{kind=link}
Drivers of inappropriate antibiotic prescribing
There are many causes of inappropriate antibiotic prescribing. Growing evidence shows that reasons for inappropriate prescribing are at least partly psychologically and socially rooted, meaning that antibiotic prescribing is as much a behavior as a scientific decision. Much of this literature is qualitative and based on surveys or interviews with clinicians, with some evidence from observational studies.
Clinicians’ perceptions
Clinicians may not realize that they prescribe inappropriately. A qualitative study of semi-structured interviews with 13 clinicians about the management of acute bronchitis found that clinicians agreed with guideline recommendations not to use antibiotics and thought that clinicians other than themselves were inappropriately using antibiotics to treat bronchitis.61 Without information on and oversight of their antibiotic prescribing patterns, clinicians may not understand their role in inappropriate antibiotic prescribing. In this same study, clinicians cited lack of feedback on their prescribing behavior and lack of accountability as barriers to appropriate antibiotic prescribing.61
Lack of knowledge
Knowledge of guideline recommendations on indications for the prescription of antibiotics is the foundation of appropriate prescribing. Lack of knowledge could lead some clinicians to prescribe antibiotics inappropriately. However, a qualitative study of 36 interviews with clinicians found that they were generally familiar with guideline recommendations for common conditions in outpatients.62 The lack of guideline recommendations for some conditions may contribute to variations in antibiotic treatment—for example, few guidelines are available on the management of dental infection.
Fear of complications
In addition, both of the above interview studies found that clinicians often cite fear of complications from infections as a reason for prescribing antibiotics when they are not indicated and for prescribing broader spectrum agents than necessary.6162 However, for ARIs that commonly lead to unnecessary antibiotic prescribing, infectious complications are rare compared with antibiotic associated adverse drug events. A cohort study of 3.36 million ARI episodes seen in primary care practices in the United Kingdom found that, overall, the number needed to treat to prevent one case of a serious ARI complication was more than 4000.63 However, as previously noted, it is estimated that for every 1000 outpatient antibiotic prescriptions, there is one emergency department visit for an antibiotic associated adverse drug event.11
Patients’ expectations
The interview studies described above also found that clinicians’ perceptions that patients want antibiotics drives them to prescribe antibiotics inappropriately.6162 Another qualitative study of pediatricians reported that antibiotics were sometimes prescribed for social reasons, such as wanting to please parents.64 Direct requests for antibiotics—that is, when patients explicitly ask for antibiotics for their illness—are rare. A qualitative study of 42 German visits to primary care clinics by adult patients with acute cough found that only two patients explicitly requested antibiotics, whereas implicit expectations were noted in seven visits.65 A 2001 mixed methods study of 295 parents at two pediatric practices found that overt requests for antibiotics occurred in only 1% of visits, yet clinicians perceived expectations for antibiotics in 34% of visits.66 Implied requests for antibiotics are more common, and certain communication behaviors by patients and families can lead clinicians to perceive that antibiotics are desired. Another mixed methods study of 522 pediatric encounters for cold symptoms found that clinicians were 20.2% (6.3% to 34.0%; P=0.004) more likely to perceive expectations for antibiotics when parents questioned the treatment plan and 9.3% (1.8% to 16.9%; P=0.02) more likely to perceive expectations for antibiotics when parents offered a candidate bacterial diagnosis.67 An example of a parent questioning the treatment plan would be when the parent responds to the clinician’s suggestions of symptomatic therapy with, “We have already tried that, and it is not helping.” An example of a parent offering a candidate bacterial diagnosis is when the parent says, “I am worried that she might have strep throat.” This study also found that clinicians were 31% (16.0% to 47.3%; P<0.001) more likely to prescribe an antibiotic for a viral diagnosis when they perceived parental expectations for antibiotics.67
Workload and time constraints
Workload and time constraints are also associated with antibiotic prescribing. In the previously discussed interview studies, clinicians reported prescribing antibiotics because they felt they did not have time to explain why antibiotics were unnecessary64 or because they perceived that writing a prescription was faster than communicating non-antibiotic treatment plans.61 Clinicians with high caseloads may be more likely to prescribe antibiotics than those with fewer patients. In an observational study of 440 general practitioners in Norway (N=142 900 ARI visits), the odds of prescribing an antibiotic for an ARI were 1.64 (1.33 to 2.03) times higher among clinicians with the highest number of ARI visits (top fifth) than among those with the lowest number of visits (bottom fifth).68 In addition, clinicians may face decision fatigue that makes prescribing antibiotics the default approach, even when inappropriate. An observational study of 21 867 primary care visits by adults found that the prescription of antibiotics for ARIs increased throughout each shift.69 The odds of receiving antibiotics for an ARI in the fourth hour of a clinic session was 26% higher than in the first hour (adjusted odds ratio 1.26; 1.13 to 1.41).69
Habit and prescription variation
Habit also drives patterns of antibiotic prescribing. The qualitative study of 36 clinician interviews described above found that clinicians report that they often rely on previous experience and familiarity with antibiotic agents.62 In addition, clinician level variation in antibiotic prescribing for ARIs is seen in studies that control for patient case mix and comorbidities. An observational study of 1 044 523 ARI visits at US Department of Veterans Affairs outpatient clinics found that 59% of the observed variation in antibiotic prescribing was attributable to provider level variation.54 Similarly, an observational study of almost 400 000 ARI visits to a pediatric primary care network found that antibiotic prescribing varied significantly by practice (P<0.001) and that this could not be explained by clinical factors, such as comorbidities or diagnosis, implying that provider level factors contributed to the observed variability.70
Interventions to improve the prescription of antibiotics in outpatient settings
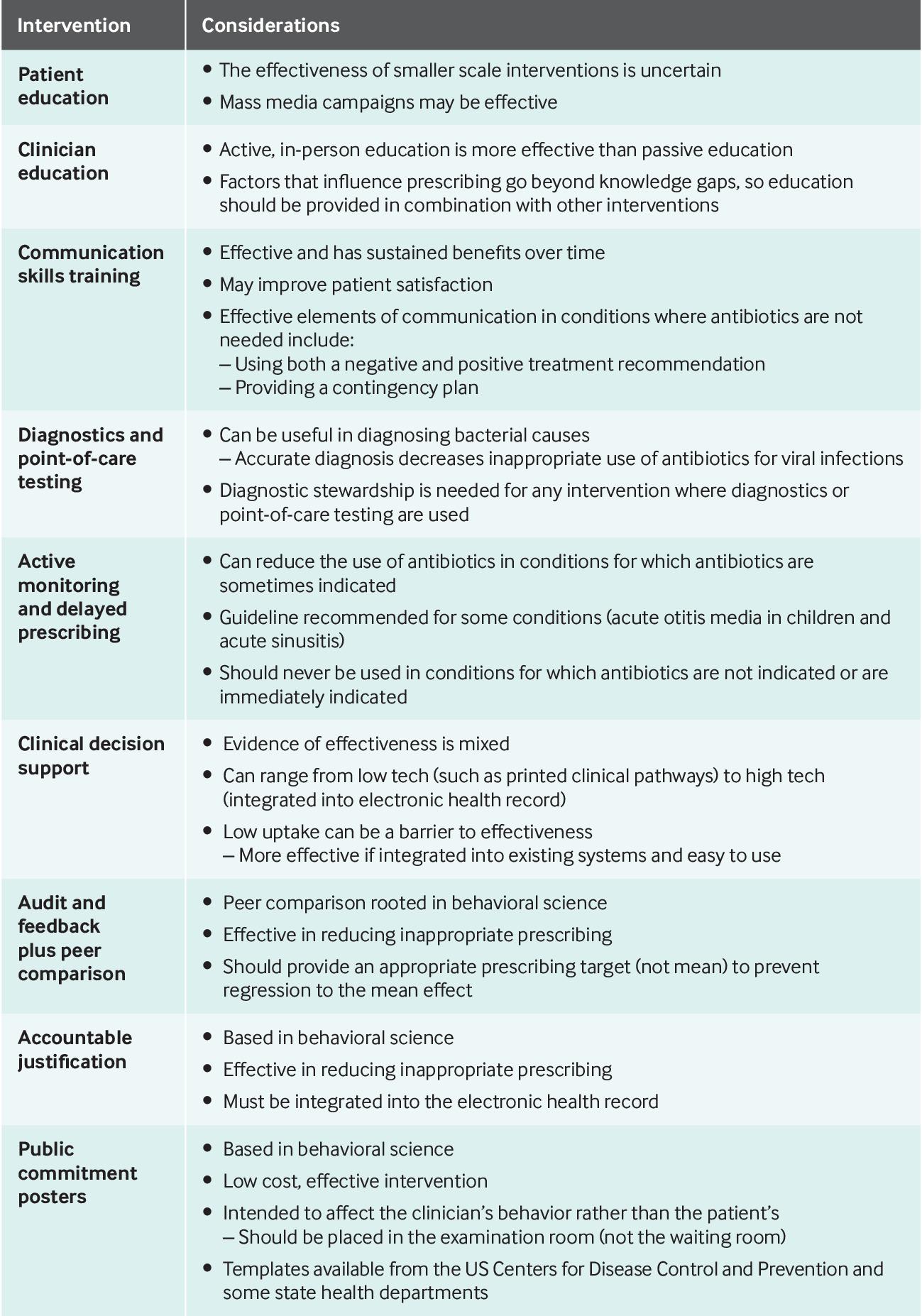
Interventions to improve the prescription of antibiotics in outpatient settings need to target the root causes of inappropriate prescribing and modify clinicians’ behavior. Here, we examine the existing literature on several potential interventions, including patient and clinician education, communication training, point-of-care testing, active monitoring and delayed prescribing, clinical decision supports, audit and feedback, accountable justification, and public commitment posters (fig 3). Although these interventions are examined individually, they could be implemented in combination, potentially to greater effect. A 2012 systematic review and meta-analysis of outpatient stewardship interventions in ARI management found that multi-part interventions were more likely to be effective than those with only one component (adjusted odds ratio 6.5, 1.9 to 22).71 These interventions (or combinations of interventions) can be implemented within a framework provided by the CDC’s Core Elements of Outpatient Antibiotic Stewardship (fig 1 and table 2). The core elements are commitment, action for policy and practice, tracking and reporting, and education and expertise and are based on much of the evidence discussed here.5

Summary of outpatient antibiotic stewardship interventions and considerations. A full discussion of these interventions and supporting evidence is available in the “Interventions to improve the prescription of antibiotics in outpatient settings” section of the text
{kind=link}
Association between the US Centers for Disease Control and Prevention’s Core Elements of Outpatient Antibiotic Stewardship and examined interventions
With increasing awareness of the complex factors involved in antibiotic prescribing, behavioral science has increasingly been used to inform antibiotic stewardship interventions, and this discipline merits special attention.72 Interventions that are informed by behavioral science have been of interest to and supported by public health agencies including the CDC,5 Public Health England,73 and the World Health Organization.74
Patient education
Clinicians cite patient demand as a factor in antibiotic prescribing and, as a result, there has been interest in patient education on the appropriate use of antibiotics. The quality of evidence on targeted patient facing education is limited and has contradictory findings. A 2016 systematic review identified two RCTs (from 2000 and 2009) that had 827 participants and evaluated written information for patients.75 Overall, the studies in this review found that written information reduced antibiotic prescribing in patients with ARI compared with usual care (risk ratio 0.47 (0.28 to 0.78) v 0.84 (0.81 to 0.86)).75 However, two other randomized trials in the UK examining educational leaflets, one a 2×2 factorial trial studying two interventions in 1581 general practices and the other a single intervention trial in 870 patients presenting to primary care practices with lower respiratory tract infection, found no significant associations between patient educational materials and decreases in antibiotic use (incidence rate ratio 1.01 (1.00 to 1.02 v 1.27 (0.86 to 1.87)).7677
Mass media campaigns have been associated with reductions in antibiotic use in observational studies, although it is difficult to evaluate causation. In an observational study of national reimbursement data (453 407 458 records), the French campaign, “Antibiotics are not automatic” was associated with a 27% reduction in the population based rate of antibiotic usage from 2000-01 to 2002-07.78 In an observational study, a media campaign in north east England was associated with a 6% reduction in antibiotic prescriptions during the winter compared with nearby areas with no campaign.79 In the US, the CDC leads a national effort, Be Antibiotics Aware: Smart Use, Best Care, to educate patients, caregivers, and clinicians about appropriate use of antibiotics (www.cdc.gov/antibiotic-use).80 In addition, the CDC observes US Antibiotic Awareness Week each November,81 which coincides with WHO’s Antibiotic Awareness Week82 and European Antibiotic Awareness Day,83 as well as other global observances.
Clinician education
Two older systematic reviews have shown that active and intensive clinician educational efforts, such as academic detailing, are more effective than passive education.8485 A more recent quasi-experimental study tested academic detailing versus provider and patient mailings and found a significant change in antibiotic prescribing among clinicians who received the academic detailing (odds ratio 0.49, 0.26 to 0.89) but no significant change among the mailing group.86 National efforts, such as the CDC’s Be Antibiotics Aware80 and TARGET in the UK,87 provide education and resources on antibiotic use for clinicians.
Communication skills training
Communication skills training for clinicians can improve antibiotic use. Such training teaches clinicians to communicate effectively with patients, to understand patients’ concerns and expectations, to provide information on expected disease course and recommended treatment options, and to provide a contingency plan if symptoms do not improve.88 A multi-arm, cluster randomized trial examined training in communication skills or C reactive protein (CRP) testing, or both among primary care clinicians in 246 practices in six European countries.88 It found that the risk of antibiotic prescribing for ARIs was significantly lower among those who received communication training (adjusted risk ratio 0.68, 0.50 to 0.87) or CRP training (0.53, 0.36 to 0.74) compared with controls.88 The risk of antibiotic prescribing was lowest in the group with both interventions (0.38, 0.25 to 0.55).88
A cluster RCT in 20 Dutch primary care practices (N=379) also assessed the effect of CRP and communication training on antibiotic prescribing for ARIs.89 Clinicians in the CRP and communication training groups prescribed fewer antibiotics than control groups (CRP: 31% of visits received antibiotics v 53% in the no test group, P=0.02; communication training: 27% of visits received antibiotics v 54% in the no training group, P<0.01).89 The group with both CRP testing and communication training prescribed the fewest antibiotics (23% of visits).89 However, 3.5 years after the interventions were removed, clinicians who received communication training still prescribed fewer antibiotics (antibiotics prescribed in 26.3% (20.6% to 32.0%) of visits for ARI) than the control group (39.1%, 33.1% to 45.1%; P=0.02), whereas there were no differences between the CRP group and the control group at follow-up.89 In quantitative and qualitative studies, clinicians who received communication skills training provided positive feedback about the training and reported increased confidence in their ability to improve antibiotic prescribing.909192
Clinicians may perceive that they are improving patient satisfaction by prescribing antibiotics; however, evidence shows that patients may still be satisfied without antibiotics providing their communication expectations are met. In a descriptive study of surveys of almost 300 patients with sore throat in Belgian primary care practices, patients listed seeking symptomatic relief, information about disease course, and reassurance about the cause of the disease as their top three reasons for visiting a physician, while obtaining an antibiotic was rated as the 11th (of 13) most important reason.93 An observational study of 5169 visits for acute sinusitis in a large integrated health system found that 79.5% of visits in which an antibiotic was prescribed resulted in a favorable patient satisfaction score compared with 75.4% of visits with no antibiotic prescription.94 This difference was significant (adjusted odds ratio 1.2, 1.0 to 1.6); however, the actual difference in the proportion of visits with a favorable score was only 4 percentage points, and the factor with the greatest effect on satisfaction was patient-clinician bonding (2.0, 1.6 to 2.3).94
An observational study of 1285 pediatric visits for ARI found that receipt of an antibiotic prescription was not significantly associated with a high satisfaction score (adjusted risk ratio 1.13, 0.95 to 1.34) whereas communication was.95 Parents who received both a negative treatment recommendation (noting that antibiotics would not help the child get better) and a positive treatment recommendation (provision of non-antibiotic strategies to help the child feel better) were more likely to rate the visit highly than patients who received no treatment recommendation (1.16, 1.01 to 1.34).95
Even among patients and caregivers who expect antibiotics, the provision of specific types of communication may maintain satisfaction. The previously discussed 2001 mixed methods study showed that satisfaction scores increased significantly among caregivers who expected an antibiotic and did not receive one when a contingency plan was provided.66 The mean satisfaction score for the no contingency plan group was 59 (53 to 65) whereas the mean score for the contingency plan group was 76 (66 to 86).66
Rapid and point-of-care diagnostic tests
When rapid diagnostic, including point-of-care, tests are available, have good sensitivity and specificity, and are not cost prohibitive, they can help guide the diagnosis and management of disease, thereby improving antibiotic prescribing. Most US patients and clinicians are familiar with the rapid antigen detection test for group A streptococcus, which is recommended in the US by the Infectious Diseases Society of America to establish a diagnosis of streptococcal pharyngitis before prescribing antibiotics.96
There has been recent interest in procalcitonin and CRP testing. Procalcitonin and CRP are biomarkers that, although not highly specific, may indicate increased risk of bacterial infection. A systematic review and meta-analysis of 26 studies examining procalcitonin testing in the management of ARI found that rates of antibiotic prescriptions per visit in primary care were significantly lower among those who used procalcitonin testing compared with controls (22.9% v 63.1%; adjusted odds ratio 0.13, 0.09 to 0.18).97 However, a more recent RCT (N=1656) of procalcitonin testing in adult patients diagnosed with acute lower respiratory tract infection in the emergency department found no significant difference in the mean number of days of exposure to antibiotics between the procalcitonin intervention group (4.2 days) and the usual care control group (4.3 days; difference −0.05 day, −0.6 to 0.5; P=0.87).98 A meta-analysis examining six trials of CRP in the management of ARI found that antibiotic use was reduced with CRP testing (pooled risk ratio 0.78, 0.66 to 0.92) compared with usual care.99 However, the authors of this meta-analysis noted that owing to heterogeneity in the studies, these results should be interpreted with caution.99
Although these tests may improve antibiotic prescribing, it is important to reiterate that communication skills training is as effective as CRP testing at reducing antibiotic prescriptions for ARIs and has sustained benefits that CRP testing does not.8889 In addition, the appropriate use of testing—diagnostic stewardship—is crucial. Testing should only be performed when the clinical presentation is consistent with bacterial infection and test results will influence management.100
Active monitoring and delayed prescribing
Active monitoring (also called watchful waiting) and delayed prescribing are treatment strategies that require patients and caregivers to observe the progression of the illness and return (active monitoring) or fill an antibiotic prescription (delayed prescribing) if symptoms do not improve or worsen. These strategies are recommended by guidelines in the US for the management of acute otitis media in children101 and acute sinusitis,102103 and they have been successful in reducing unnecessary antibiotic use. Delayed prescribing and active monitoring should not be used in conditions where antibiotics are not indicated or are immediately indicated. A meta-analysis of delayed prescribing for ARIs found that delayed prescribing resulted in significantly lower odds of antibiotic use than immediate prescribing (seven studies, N=1963; odds ratio 0.04, 0.03 to 0.05) with no significant difference in patient satisfaction (six studies, N=1633; 0.65, 0.39 to 1.10).104
A 2016 randomized trial in 405 visits by adults for ARI in 23 Spanish family practice clinics examined the effect of antibiotic prescription strategies on several outcomes, including antibiotic use.105 Antibiotic use was significantly different among groups: 91% of patients who received immediate antibiotic prescriptions used antibiotics, compared with 33% of patients who had delayed antibiotic prescriptions, 23% of patients who were instructed to return to the clinic to pick up a prescription if needed, and 12% of patients not prescribed antibiotics (P<0.001).105 This trial found no differences in patient satisfaction, complications, adverse events, or unscheduled return visits between groups.105 Furthermore, in a mixed methods study of children with acute otitis media, most parents who used pain management and delayed prescribing instead of immediate antibiotic treatment reported that they would be willing to treat future episodes without antibiotics.106
Clinical decision support
Studies examining clinical decision support (CDS), which provides information and decision support at the time of diagnosis or treatment, have shown mixed results. A cluster randomized trial of 33 primary clinics used both printed and electronic CDS for acute bronchitis in otherwise healthy adolescents and adults who had 9808 visits during the baseline and 6242 visits during the intervention period.107 Antibiotic prescribing for acute bronchitis decreased significantly in printed CDS sites (80.0% to 68.3%) and at electronic CDS sites (74.0% to 60.7%) but not at control sites (72.5% to 74.3%).107 Prescribing was not significantly different between printed and electronic CDS sites.107 However, notably, the appropriate rate of antibiotic prescribing for acute bronchitis in patients included in this study was zero. Another cluster randomized trial of a CDS intervention in 27 primary care clinics with 21 961 visits for ARI found that the CDS tool was used in as few as 6% of visits in the intervention group and was not effective.108
An additional cluster randomized trial in 104 family practice facilities in England and Scotland found that about 25% of intervention practices used the CDS tool rarely or not at all.109 CDS design is important for its uptake and effectiveness; a 2015 systematic review of randomized trials found that CDS tools for which decision support was integrated into existing processes were more likely to improve prescribing than systems that required active initiation by the clinician.110
Finally, any achieved benefits may not be sustainable once the intervention is removed. A quasi-experimental study in the US Department of Veterans Affairs health system (N=1131 ARI visits) found that a CDS tool for the management of ARI improved guideline concordant prescribing; however, after the tool was removed, inappropriate prescribing increased.111
Audit and feedback with peer comparisons
There is strong evidence to support the tracking of antibiotic prescribing practices and reporting them back to clinicians—a practice known as audit and feedback, which is recommended by the CDC’s core elements.5 The core elements also specify that effective audit and feedback interventions should include comparisons of clinicians’ prescribing with their peers.5 A cluster randomized trial in 18 pediatric primary care practices (N=1 291 824 visits) evaluated an intervention whereby pediatricians received education and feedback on prescribing patterns for themselves, their practice, and their network.112 The intervention was associated with a 12.5% decrease in the prescription of broad spectrum antibiotics for ARIs, with a statistically significant difference in differences of 6.7% (P=0.01) versus controls.112 Unnecessary prescription for ARIs was low at baseline and did not change significantly during the intervention for any group (P=0.93).112 However, a follow-up observational study found that when the intervention was removed, antibiotic prescribing patterns returned to pre-intervention levels.113
Behavioral science has been used in two recent audit and feedback studies to increase the effectiveness of the intervention.76114 In the first, a randomized trial, 3227 letters were sent to UK general practitioners. The letter informed physicians that they were prescribing antibiotics at higher rates than 80% of general practitioners in their area (provided social norm information). The letter was signed by a high profile figure, England’s chief medical officer, to increase credibility, and it gave three specific actions that clinicians could take to reduce unnecessary antibiotic prescribing.76 During the intervention phase prescription rates in the letter intervention group were significantly lower than in controls, 126.98 (125.68 to 128.27) antibiotics per 1000 weighted population versus 131.25 (130.22 to 132.16; incidence rate ratio 0.97, 0.96 to 0.98; P<0.001).76
The second study, a cluster randomized trial in 47 primary care practices in Boston and Los Angeles, US, examined three stewardship interventions designed using behavioral science principles: peer comparison, accountable justification, and suggested alternatives.114 In the peer comparison intervention arm, clinicians with the lowest inappropriate antibiotic prescribing rates for ARIs received an email informing them that they were top performers, reinforcing the desired behavior, while all other clinicians received emails informing them that they were “not a top performer.”114 The intervention was designed to drive performance to a goal, rather than the mean, and therefore did not include an average prescribing comparison. This peer comparison was associated with a significant decrease in inappropriate antibiotic prescribing for ARIs from 19.9% to 3.7% (difference in differences compared with controls, −5.2, −6.9% to −1.6%).114 One year after the interventions were discontinued, the peer comparison was the only intervention arm (of three) that had significantly lower prescribing rates than the control group.115
Accountable justification
Accountable justification, in which clinicians must document explanations for non-indicated antibiotic prescriptions, was associated with a reduction in inappropriate antibiotic prescribing in the previously mentioned study of 47 primary care practices.114 The intervention was based on the behavioral science principles that accountability improves decision making and public justification creates social and reputational concerns that improve behavior.114 Clinicians knew that antibiotic justification notes in the medical record would be visible to other clinicians, thus increasing accountability for inappropriate prescribing. The intervention was associated with a significant reduction in prescribing for ARIs from over 23.2% to 5.2% (difference in differences, −7.0%, −9.1% to −2.9%; P<0.001).114 By contrast, the suggested alternatives in this study, where the electronic health record suggested non-antibiotic treatments, did not significantly improve prescribing compared with the control group (P=0.66).114
Public commitment posters
Lastly, evidence shows that the use of public commitment posters, a simple, low cost intervention, reduces inappropriate antibiotic prescribing. Commitment posters are behavioral nudges for clinicians that are designed to utilize clinicians’ desire to remain consistent with previous public commitments.116 An RCT of 954 visits by adults with ARIs in five outpatient clinics tested the use of public commitment posters in patient examination rooms.116 The posters included a letter from the clinician committing to use antibiotics appropriately and the clinician’s picture and signature.116 This intervention was associated with an absolute reduction in inappropriate prescribing for ARIs of 19.7% (5.8% to 33.0%) compared with the control group (P=0.02).116 Commitment posters have been adopted by state health departments, healthcare systems, and the CDC.5117
Emerging interventions
A search of clinicaltrials.gov for the terms “antibiotic” and “outpatient” yielded 24 active studies. Three of these 24 studies examined interventions to improve antibiotic prescribing in outpatient settings. The first, an RCT in Switzerland, is in the enrollment phase and will evaluate a nationwide antibiotic stewardship program that uses routine feedback and clinician and patient education on overall and broad spectrum antibiotic use and rates of hospital admission (NCT03379194). The second is an RCT that will examine education and communication skills interventions among clinicians, looking at the outcomes of parental ratings of shared decisionmaking and satisfaction, inappropriate antibiotic prescribing, re-visits, and adverse drug events (NCT03037112). This trial is currently in the recruitment phase and the estimated date of completion is June 2019. The third study is recruiting clinicians in France to investigate the effect of regional antibiotic consumption and bacterial resistance data on prescribing practices and antibiotic resistance (NCT02816528); however, information on this study has not been updated since June 2016.
Guidelines
The CDC’s Core Elements of Outpatient Stewardship offers guidance for implementation of outpatient antibiotic stewardship.5 In addition, many guidelines for common outpatient conditions provide specific recommendations on antibiotic prescribing that, if followed, could reduce unnecessary prescription and improve agent selection and treatment duration when antibiotics are indicated. The Healthcare Infection Control Practices Advisory Committee (HICPAC) has provided recommendations on incorporating antibiotic stewardship principles into treatment guidelines, emphasizing diagnostic testing and the treatment of infectious diseases.118 In addition, the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America have developed guidelines for the implementation of antibiotic stewardship programs in inpatient settings,119 and some of the strategies in these guidelines may be beneficial in outpatient settings as well.
Conclusion
About 270 million outpatient prescriptions for antibiotics are dispensed in the US each year, and at least 30% of these are unnecessary.437 The use of antibiotics is not without risks, such as antibiotic resistance and adverse events. Antibiotics should be considered when the clinical benefits outweigh the risks, such as for sepsis or suspected sepsis. The use of antibiotics only when needed and using the right agent, dose, and duration at the right time is a matter of patient safety.
In addition to clinical factors, the prescription of antibiotics in the outpatient setting is also driven by psychosocial factors including lack of self awareness, fear of complications, perceived patient expectations, and time constraints and fatigue. Many different outpatient antibiotic stewardship interventions have shown some success, and the use of multiple, complementary intervention strategies can reduce inappropriate antibiotic use. The most effective combination of interventions will depend on the outpatient setting and practice; however, behavioral science based interventions (public commitment posters, accountable justification, and feedback with peer comparison) and communications training have shown promising results and should be included in any antibiotic stewardship intervention package. The Core Elements of Outpatient Antibiotic Stewardship can facilitate the implementation of stewardship interventions in outpatient settings. The appropriate use of antibiotics is an important component of best patient care and should be a cornerstone of effective outpatient practice.
Questions for future research
What effects do outpatient antibiotic stewardship interventions have on adverse events?
What effects do outpatient antibiotic stewardship interventions have on antibiotic resistance?
What is the return on investment of outpatient antibiotic stewardship interventions?
Which antibiotic stewardship interventions help improve agent selection, dose, and duration in conditions where antibiotics are indicated?
Is there a correlation between inappropriate antibiotic prescribing and inappropriate prescribing of other drugs, such as opioids?
Do pay-for-performance or other financial incentives, similar to the Quality Premium program in the UK, improve antibiotic prescribing in US outpatient practices?
Patient involvement
No patients were involved in the creation of this article
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Contributors: All three authors made substantial contributions to the conception of the manuscript, approved the final version of this manuscript, and agree to be accountable for all aspects of the work. LMK conceptualized the review, performed the literature review, and wrote the article. KEF-D and LAH conceptualized the review and provided critical revisions for important intellectual content. LAH, as guarantor, accepts full responsibility for the work, had access to the references reviewed, and controlled the decision to publish. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Competing interests: We have read and understood BMJ policy on declaration of interests and declare that we have no competing interests.
Provenance and peer review: Commissioned; externally peer reviewed.
Disclaimer: The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
License: This work was conducted by employees of the US Federal Government. For employees of the US Federal Government employees acting in the course of their employment, no copyright exists and the Contribution is in the public domain so no license is required to be granted.