Article Text

Abstract
Objective: To assess the effects of joint consultation on referral behaviour of general practitioners (GPs) in a prospective cohort study.
Methods: All patients with rheumatological complaints that 17 participating GPs, from the area of the University Hospital Maastricht, wanted to refer during a two year inclusion period (n=166) were eligible for inclusion. These patients were either referred to the outpatient clinic, or presented at a joint consultation held every six weeks at the practice of the GP, where groups of three GPs presented their patients to a visiting, consulting rheumatologist. The number of patients referred by each GP a year at the end of the trial, comparing participating and non-participating GPs, was the main outcome measure.
Results: During two years of inclusion, the 17 participating GPs presented 166 patients. The number of patients referred by each GP a year decreased for the participating GPs by 62% at the end of the whole study. By contrast, non-participating GPs maintained the same rate of referral. The range of diagnoses remained proportionally the same throughout the study, with the exception of fibromyalgia. The referral rate of this diagnosis decreased significantly (p=0.001).
Conclusions: Joint consultation seems to be a good strategy in influencing the referral behaviour of GPs in the area of rheumatology. The decrease in referral is substantial and can subsequently lead to a reduction of waiting lists.
- general practitioner
- referral
- joint consultation
- rheumatologist
Statistics from Altmetric.com
Doctor’s delay and long waiting lists bear the risk of compromising the accessibility and quality of the healthcare system. In The Netherlands, waiting lists grow constantly. Despite many efforts, no approach has yet been successful in effectively reducing these lists.
In the Dutch healthcare system, patients are generally only admitted to specialised outpatient care after referral by a general practitioner (GP). This implies that the GP, as a gatekeeper, has a strong regulating effect on the influx of patients to outpatient clinics and thereby a great influence on waiting lists.1–5 At the same time, the GP is primarily responsible for the treatment of the patient. Because of the reduced accessibility to outpatient clinics and the high prevalence of musculoskeletal complaints at the primary healthcare level (15% of all complaints the GP is faced with6), the GP plays an increasingly important part in the treatment of musculoskeletal complaints.
The performance of GPs and the referral pattern could be improved by further educating GPs, thereby improving their knowledge and skills. Problem based learning is by far the most effective way of teaching.7–15 Consequently, a model based on problem based learning could have a beneficial effect on rheumatological skills of the GP and on referral and thus on waiting lists, while assuring adequate treatment by the GP.16–19
We propose joint consultation as a model which, through close collaboration between specialists and GPs, meets the requirements for improving rheumatological performance as well as reducing waiting lists.
METHODS
During a period of two years (1999–2000), 17 GPs within the region of the University Hospital Maastricht, participated in our randomised trial. The rather isolated geographical position of the hospital created a situation in which patients would almost exclusively be referred to this one hospital. Responding to a questionnaire among all GPs (n=93) in the region, 60 (65%) said that they would be willing to participate in a joint consultation with a rheumatologist. Declining to participate was mostly based on a perceived lack of time. The final selection of participants was based on availability of GPs for this study and criteria that would match the participants to the general population of referring GPs: (a) practice characteristics (solo, group practice) and location (urban, countryside), and (b) referral behaviour (10–12 referrals to the department of rheumatology by each GP a year). Seventeen GPs were selected and agreed to participate (mean age 48.5 years, 12% women, 47% rural practice; no significant differences in characteristics were found compared with non-participating GPs). Referral pattern of the participating GPs matched the referral pattern of non-participating GPs. This overall referral pattern to the outpatient clinic of rheumatology was not influenced by guidelines or educational programmes, either before or during the study. There were no reasons to assume that the competency of GPS in dealing with musculoskeletal problems in this region differs from that of other Dutch GPs.
The 43 non-participants who had expressed a willingness to participate acted as a control group. The referral rates (and practice/personal characteristics) of non-selected GPs who were willing to participate in the study (n=43) were comparable with those of GPs who declined to participate (n=33).
All six staff members of the department of rheumatology were assigned as consultants. Sample size was calculated for a minimal change of 20% for the primary outcome (which was the referral rate of the participating GPs) and resulted in n=84/group (α=0.05 and α=0.1)
Any patient the participating GPs wanted to refer had to be included into the study (excluding patients needing emergency referral). After informed consent, the patients entered the study after the GP had received the outcome of the randomisation by telephone. Patients were either referred to the outpatient clinic or they were invited to the next joint consultation session (intervention group). The six weekly joint consultation sessions consisted of three GPs, as well as one visiting rheumatologist, at the practice of a host GP. The GPs presented each patient. Next, the consulting rheumatologist re-examined the patient and formulated a diagnostic and therapeutic policy together with the GP.
The opinion of the rheumatologist was considered as the “gold standard” in the assessment of the diagnoses. These were divided into five categories by means of the standard diagnoses registration (SDR) form, which is used by most Dutch rheumatologists in the registration of rheumatological diseases at outpatient clinics.20 These five categories consist of arthritis, systemic illness, osteoarthritis, arthralgias, and a fifth category, which was subdivided for the purpose of this study into fibromyalgia (also comprising general pain syndromes) and other diagnoses (including bursitis and tendinitis)). The SDR database supplied data on the overall number of patients with the diagnosis fibromyalgia at the department of rheumatology for our hospital during the years 1995–2000.
Participation in this study would supposedly lead to a change in referral behaviour of the GPs; convenience (avoiding the extra effort of participating in a study) could lead to an increase of referral to other, related, specialists. Therefore, the medical administrative department of the University Hospital Maastricht was requested to supply data on the number of referrals to outpatient clinics of internal medicine, neurology, orthopaedic surgery, and rheumatology for both the 17 participating GPs and for the remaining 43 non-participating GPs (the control group).
For the analysis of the referral data to the department of rheumatology, 17 non-participating GPs were matched to the participants for location (urban-rural), work load (full time, part time), and overall referral rate to the outpatient clinic of rheumatology before the study.
The numbers of referrals from each GP for the year 2000 were compared with the preceding year (1999) and the difference between the two years was assessed for both the 17 participating GPs and for 17 non-participating GPs using the Mann Whitney U test. Data on the number of patients referred by each GP for the year 1998 were not available except for group level data. Therefore we chose to compare the first year of the study with the second year of the study.
In the statistical analyses of the diagnostic subcategory fibromyalgia, the variation in the number of diagnoses of fibromyalgia between the 17 participating GPs was taken into account. These data were obtained for two time points (beginning and end of the study: 1999–2000). As the data from each GP were considered to be related samples, the Wilcoxon signed rank test was used for this analysis.
The medical ethics committee of the University Hospital Maastricht approved the study.
RESULTS
During the two years of the study, 166 patients were included. Twenty three patients were referred to the outpatient clinic of rheumatology by the participating GPs without entering the study. Declining to participate by the patient (16/23) and the GP’s opinion that a patient was not suitable for joint consultation (4/23; 3/23 other reasons), were the main reasons for non-participation (mean age of non-participants 51.2 (SD 17.8) years; 30% were men). This non-participation was equally spread over the study period (24 months). The mean age of the participating patients was 53.7 (SD 14.0) years; 27% were men.
Before the beginning of the intervention (until 1999) both participating and non-participating GPs had an increasing yet comparable referral rate to the department of rheumatology. By the end of the study period (2000), the number of patients referred by each GP a year (3.7 patients/GP/year) by the participating GPs differed (−62%) from the number of patients referred (9.7 patients/GP/year) by the 17 matched non-participating GPs. We found an average reduction in the referral rate of −2.8 (SD 3.9) patients referred for participating GPs when comparing 2000 to 1999, versus a difference in the referral rate of zero (SD 2.1) patients referred for the 17 non-participating GPs, a difference which was significant (p=0.024; Mann-Whitney U test).
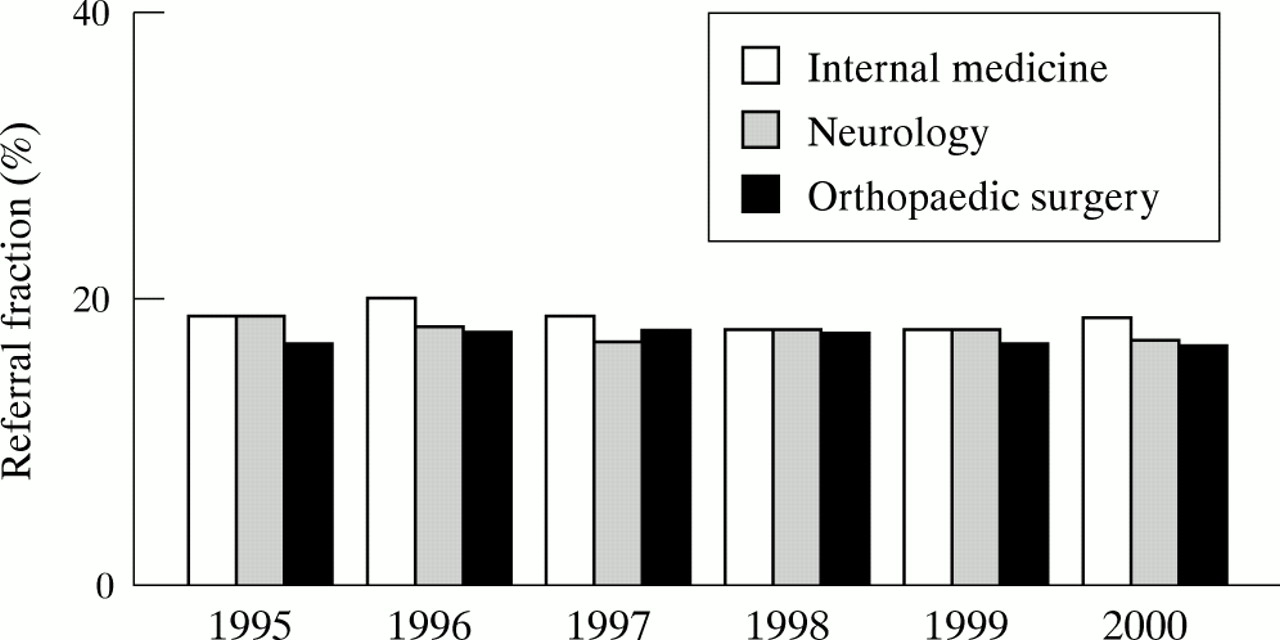
This remarkable change was not found for non-rheumatological referrals by the 17 participating GPs (fig 1).
{kind=link}
Proportion of referrals by the 17 participating GPs expressed as a fraction (%) of all referrals by all 76 non-participating GPs for internal medicine, neurology, and orthopaedic surgery. Note that there are no changes after the start of the intervention (1999).
Moreover, we found a shift in the range of diagnoses over time (table 1). Whereas all the other standard diagnosis registration categories showed no significant change proportionally, the subcategory fibromyalgia showed a significant decrease (p=0.001; Wilcoxon signed rank test), comparing the first year of the intervention (in 1999, 40 out of the 144 diagnoses comprised fibromyalgia) to the second year of the intervention (in 2000, eight out of 72 diagnoses comprised fibromyalgia). The overall number of patients with the diagnoses fibromyalgia (as referred by all 93 GPs from the region) remained stable for the years 1995–2000 (1995: 186 patients, 1996: 192 patients, 1997: 190 patients, 1998: 180 patients, 1999: 208 patients, and 2000: 184 patients).
Number of diagnoses in time for each standard diagnoses registration (SDR) category, which consisted of arthritis (1), systemic illness (2), osteoarthritis (3), arthralgias (4), other diagnoses (including burstitis, tendinitis) (5), and fibromyalgia (6). More diagnoses per patient were recorded
In the two year study period, 54 joint consultation sessions (for 87 intervention group patients) were held with an average of 1.4 hours a session. There were 47 follow up consultations for this group, with a standard duration of 15 minutes. A primary consultation at the department of rheumatology was a standard 45 minutes (for 79 control group patients) and the 96 follow up consultations that resulted from these were a standard 15 minutes. This resulted in a total of 87.4 hours invested by the rheumatologists in joint consultation versus 83.3 hours in total at the outpatient clinic. For each patient, joint consultation takes 1.0 hours versus 1.1 hours for each patient at the patient clinic. If all 166 patients had been examined in joint consultation sessions, this would have led to 144.2 hours of joint consultation sessions and 22.5 hours of follow up consultations, resulting in 166.7 hours in total. If the 17 participating GPs had only referred to the outpatient clinic (and joint consultation education had not caused a decrease in referral), 292 would have been referred, based on the referral rate of the 17 participants before joint consultation. These 292 would have taken 219.0 hours of primary consultations and 88.8 hours of follow up consultations, resulting in 307.8 hours in total. Joint consultation would have led to a decrease of 46% in the time spent by the rheumatologists.
DISCUSSION
In the process of reducing waiting lists, transferring patients from the secondary healthcare level back to the primary healthcare level is an often used and important strategy.
Many outpatient clinics have long waiting lists and incur more direct medical expenses compared with primary health care. Therefore, preventing access to specialist care or transferring patients to primary care seems a logical solution. There are, however, some specific aspects that have to be taken into consideration.
Firstly, the level of knowledge and skills of a specialist is not straightforwardly comparable with that of a GP. In joint consultation however, the patient is primarily treated by the GP, but the specialists’ skills are transferred as well to the primary healthcare level. Therefore, the standard of medical care will not be compromised in any way.
Secondly, the daily workload of GPs increases steadily, which makes any extra burden not very attractive at first sight. Although joint consultation may lead to an increased patient workload for the GP, we think that a skilled and confident GP ultimately needs less time and effort to treat comparable patients. Improving the ability to treat confidently more patients appropriately with a certain ailment, does not automatically imply a larger workload, especially not in the long term. The large decrease in the number of patients referred with fibromyalgia (which was not found in non-participating GPs) supports this view. Fibromyalgia is a condition that can be diagnosed and treated adequately by a skilled GP.
The impact of joint consultation rheumatology on referral behaviour is substantial (62% decrease in referrals by the end of the study). The non-participating GPs maintained a constant high level of referrals throughout the duration of the study. Also, adjacent medical fields such as internal medicine, neurology, or orthopaedic surgery showed no change in referral rate by the participating GPs. Hence, it seems reasonable to attribute the decrease in referral rate for the outpatient clinic of rheumatology to the joint consultation intervention. Moreover, the decrease in referral for the participating GPs seemed specific for rheumatology, and is supposedly not a manifestation of a general trend of decrease in referral rate by the participating GPs.
A reduction in referral of the magnitude accomplished in this study seems promising for a long term evaluation of the joint consultation as a joint care model. This is confirmed by study of the time invested by the participating rheumatologists. Because of the large decrease in follow up consultations after joint consultation (and the decrease in referrals due to participation in joint consultation), there is “time effectiveness” compared with the time invested at the department of rheumatology. Seemingly labour intensive, joint consultation apparently does not take up more time.
Obviously, other aspects have to be taken into consideration before any definitive conclusions can be drawn. Cost assessment, durability of the effects, long term evaluation of the opinion of all stakeholders, and also qualitative and quantitative assessment of diagnostic and therapeutic performance are among the issues that need to be considered in detail. Provided that these issues accord with the reported results, joint consultation would be an important step in diminishing the waiting list problem while simultaneously assuring rheumatological care for patients with these highly prevalent diseases.