Article Text

Abstract
Objective: To standardize the presentation of the more than 1200 ICD-10 “S” and “T” codes from Chapter XIX by cross classifying the body region of injury by the nature of injury using the ICD-10 injury mortality diagnosis matrix. This paper explains the rationale for decisions made when developing the matrix and presents mortality data using the matrix.
Design: ICD-10 codes are organized by diagnosis groups and body regions of injury for the purpose of standardizing presentation. The categories can be collapsed to facilitate analysis at varying levels of detail. Findings from the United States 2002 injury mortality data are used as an example.
Main outcome measures: All injury diagnoses mentioned in deaths with an underlying cause of injury.
Results: There were a total of 247,195 injury diagnoses mentioned in the 161,269 deaths with an underlying cause of injury in 2002 in the United States. The matrix can be used to show that 30% of all injury diagnoses mentioned were to the head and neck region; 28% were system wide injuries, 17% were to the torso. Open wounds accounted for 17% of all injury diagnoses mentioned, and close to half of all open wounds were traumatic brain injuries. Twenty eight percent of injury diagnoses mentioned were unspecified as to their nature and 9.5% had no body region specified.
Conclusions: Multiple cause of death data are a rich but underused source of injury data often due to the complexity of the data and of the ICD classification system. Analytic techniques will need to be refined to accommodate deaths with multiple contributing injury diagnoses. The injury mortality diagnosis matrix will facilitate analysis as it is a useful tool for summarizing diagnosis data associated with injury deaths.
- IMD, injury mortality diagnosis
- NCHS, National Center for Health Statistics
- TBI, traumatic brain injury
- ICD-10
- injury diagnosis
- multiple cause of death data
Statistics from Altmetric.com
- IMD, injury mortality diagnosis
- NCHS, National Center for Health Statistics
- TBI, traumatic brain injury
Injury deaths are described primarily by ICD codes for the external cause (for example, motor vehicle crash, firearm) and for the injury diagnosis (for example, crush injury to the head, open wound to the chest).1 Both external causes and injury diagnoses are commonly referred to as “multiple cause of death” data. The term “injury diagnosis” is used in this paper to denote the ICD-10 coded description of the body region and nature of the injury mentioned on the death certificate.2 Although understanding the external cause of the injury is a key component to preventing injuries, injury diagnosis data are important for prevention as well. For instance, by learning about the kinds of injuries sustained in fatal crashes, engineers may be able to improve vehicle design. This paper introduces the ICD-10 injury mortality diagnosis (IMD) matrix, a tool for categorizing the more than 1200 individual injury diagnosis codes by body region and nature of injury and for presenting multiple cause of injury diagnosis data.2 The IMD matrix is a tool that can be used in the first stages of analysis when multiple cause data are available.
BACKGROUND
In 2002 the Barell matrix was published as a tool to classify injury morbidity data based on ICD-9-CM codes into a standard format.3,4 It has been used to describe national trends in injury related hospital discharge data5 and to aid in analysis of injury data6 from trauma registries. It has been adopted by the State and Territorial Injury Prevention Director’s Association (STIPDA) as guidance to states in how to present their hospitalization data.7 The organization of the new IMD matrix is similar to the Barell matrix with rows for body region of injury and columns for nature of injury.
The IMD matrix is designed to complement the Barell matrix by providing a tool to organize injury diagnosis mortality data into meaningful groupings by body region and nature of injury. The ICD-10 IMD matrix was developed to be as similar to the Barell matrix as possible, acknowledging the differences in data quality and coding systems. Differences between the Barell injury diagnosis matrix and the ICD-10 IMD matrix are primarily due to differences between the level of detail typically found in morbidity and mortality data and the relative lethality of some injuries over others. For example, it is far less likely for a sprain or strain to be listed on a death certificate than on a hospital discharge record. Thus, sprains and strains are included with the nature of injury category “other specified injuries” in the matrix.
Morbidity data tend to include more detailed descriptions of the injury as compared to mortality data, and therefore the Clinical Modifications of the ICD (that is, ICD-9-CM, ICD-9-AM) have many more codes than the non-modified version. Consequently, categorization of nominally similar injury diagnosis descriptions into body region and nature varied between the matrices because allowances had to be made for the fewer codes and generally poorer data quality in the mortality data. The codes that define the traumatic brain injury (TBI) category are an important example. “Open wound of head” is categorized as “TBI” in the IMD matrix but as “other head injury” in the Barell matrix. This apparent inconsistency is based on the experience using the US mortality data and is consistent with the definition of TBI recommended by the CDC’s National Center for Injury Prevention and Control.8 In the US, 64% of death records with an underlying cause of death of suicide by firearm have a single injury diagnosis code. Over three quarters of those with a single code were in the range of ICD-10 S01 (.0–.9), “open wound of head”. Presumably these deaths were a result an intracranial injury and the open wound code is a result of very little diagnosis information available on the death certificate. Because categorization is not dependent on external cause, all open wounds to the head (ICD-10 S01) regardless of the external cause were categorized as TBIs. In contrast, morbidity data tend to have more detailed diagnostic descriptions available from which to code; thus, in the case of a self inflicted firearm injury to the head, there may be an open wound code in addition to a code for intracranial injury. If the injury did not involve the brain, “open wound to the head” would be categorized in the Barell Matrix with “other head injuries”. These differences in categorization are a recognized limitation for comparing across the two matrices.
The structure of the codes for injury diagnoses changed between revisions of the ICD. In ICD-9, the codes in the injury diagnoses chapter (chapter XIX) are organized by nature of injury and then body region within each nature.9 In ICD-10, the axes in chapter XIX are reversed so the main block headings are body regions and within the body region blocks are the codes for the nature of injury.2 We do not know if this modification affects the data because there is not a comparable ICD-9 injury mortality diagnosis matrix. If an ICD-9 IMD matrix were developed, the 1996 US mortality data coded using both ICD-9 and ICD-10 could be used to explore the differences. For complete documentation of the dual coded publicly available file and downloading instructions see the NCHS Data Warehouse.10
METHODS
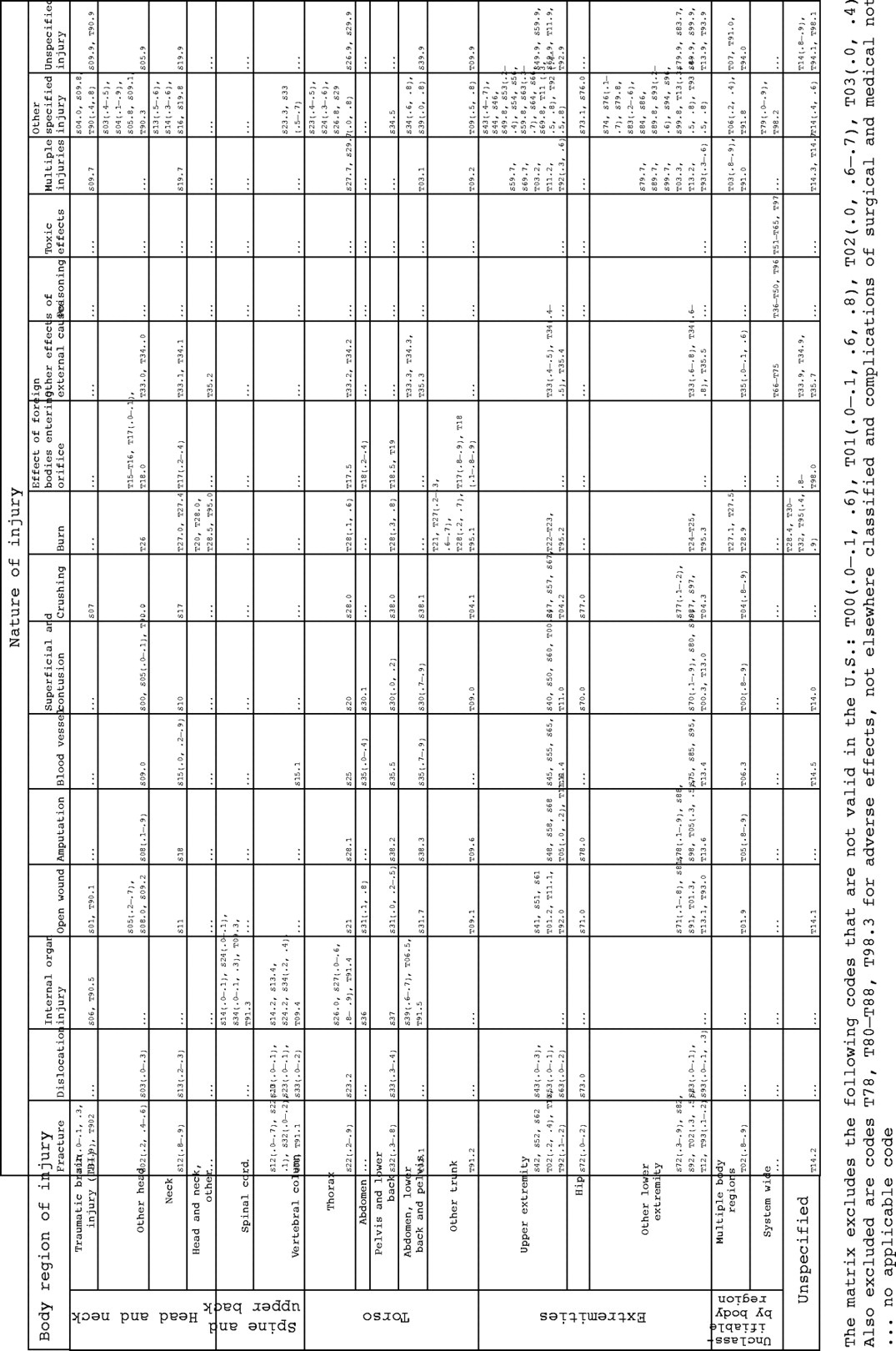
The ICD-10 IMD matrix was developed by NCHS based on an initial draft developed by Richard Hockey from Australia in 2002 along with programming assistance from the US Pacific Institute for Research and Evaluation. The injury descriptions in ICD-10’s chapter XIX (“S” and “T” codes) were reviewed and categorized into body region and nature categories with the attempt to be as similar as practicable to the Barell matrix. To maintain consistency with the external cause of injury mortality matrix (for both ICD-9 and ICD-10), adverse effects, not elsewhere classified (T78), and complications of surgical and medical care, not elsewhere classified (T80–T88) as well as their sequelae (T98.3) were excluded.1 In addition, certain codes are invalid for use in the US and are shown at the bottom of figure 1.11

ICD-10 codes used to define cells of the injury mortality diagnosis (IMD) matrix.
At its most detailed level, the ICD-10 IMD has 20 nature of injury categories and 43 body region categories. In this paper, the detailed structure is collapsed into 16 nature of injury diagnosis categories and 17 body region of injury diagnosis categories. Categories for both axes were combined based on characteristics of the body region (for example, foot and ankle injuries are part of “other lower extremities”) as well as the number of injury diagnoses mentioned in a category (for example, if there were too few). The latter was generally a reflection of the low lethality of the diagnosis (sprains and strains, for example). For some analyses, the body regions can readily be combined into six broad groups to make the data more readily interpretable by other dimensions, such as external cause of injury or age. Tables 1 and 2 show the matrix categories for each axis at different levels of detail.
Injuries mentioned according to body region of injury by categorical level of detail among all deaths with an underlying cause of injury: US, 2002
Total number of injury diagnoses mentioned according to nature of injury among all deaths with an underlying cause of injury: US, 2002
Figure 1 shows the ICD-10 codes that are in each of the possible injury diagnosis matrix cells formed by crossing the 17 body region categories by the 16 nature of injury categories. ICD-10 codes for the complete 20×43 matrix can be found on the NCHS Injury Data and Resources website http://www.cdc.gov/nchs/about/otheract/ice/projects.htm under Reporting Frameworks. Similar to the Barell matrix there are some cells for which no ICD-10 codes apply (for example, fracture of the abdomen). Like the Barell matrix, injuries acting on the entire body including poisoning, toxic effects, and early complications of trauma are assigned the body region of “system wide” and populate only that body region. The nature of injury category “other effects of external causes” which was included with “system wide” in the Barell matrix is also included in the ICD-10 IMD matrix with one exception—codes for frostbite (T33–T35) are included across appropriate body regions. In the Barell matrix, the category “effects of foreign body entering through orifice” (ICD-9-CM 930-949) is included with “system wide” injuries. We have reconsidered this for the ICD-10 IMD matrix and chosen to assign them a unique nature of injury category and spread the codes in the appropriate body region. Unlike the Barell matrix, ICD-10 codes for sequelae of injuries (referred to as “late effects” in ICD-9-CM) are included with their respective diagnoses. For example, sequelae of burns (T95[.0-.9]) is included with all burn injuries and assigned to the appropriate body regions. Although it could be argued that injuries such as “dislocations” and “superficial injuries and contusions” are less likely as other injuries to be fatal, these categories were retained for two reasons: there were more than 500 total mentions in each of these categories and for consistency with the Barell matrix.
Deaths with an underlying external cause (that is, injury) may have one or more injury diagnoses mentioned and, therefore, the unit of analysis (for example, deaths, total injury diagnoses mentioned) must be determined in order to summarize the data using the rows, columns, or cells of the IMD matrix. We have considered four methods to summarize the 2002 US multiple cause data: (1) total mentions of injury diagnoses;1 (2) any mention of an injury diagnosis (or at least one mention);1 (3) each mention of an injury diagnosis weighted proportionally to the number of injury diagnoses mentioned on the death certificate;12 and (4) multiple injury profiles as suggested for use with the Barell matrix.6,13
As the aim of this paper is to introduce the matrix, we chose to present the data using only one method—total mentions. The unit of analysis when counting total mentions is each injury diagnosis mentioned in a death. Regardless of the way the data are categorized (that is, the level of detail used in the matrix), the total number of diagnoses mentioned will always add to the same number of diagnoses. For example, suppose a person was fatally injured in a motor vehicle traffic related crash and sustained three extremity fractures—one upper, one lower, and one to the hip. Assuming all three injuries are mentioned on the death certificate, the number of “total mentions” will be three regardless of the number of extremity categories of the matrix used.
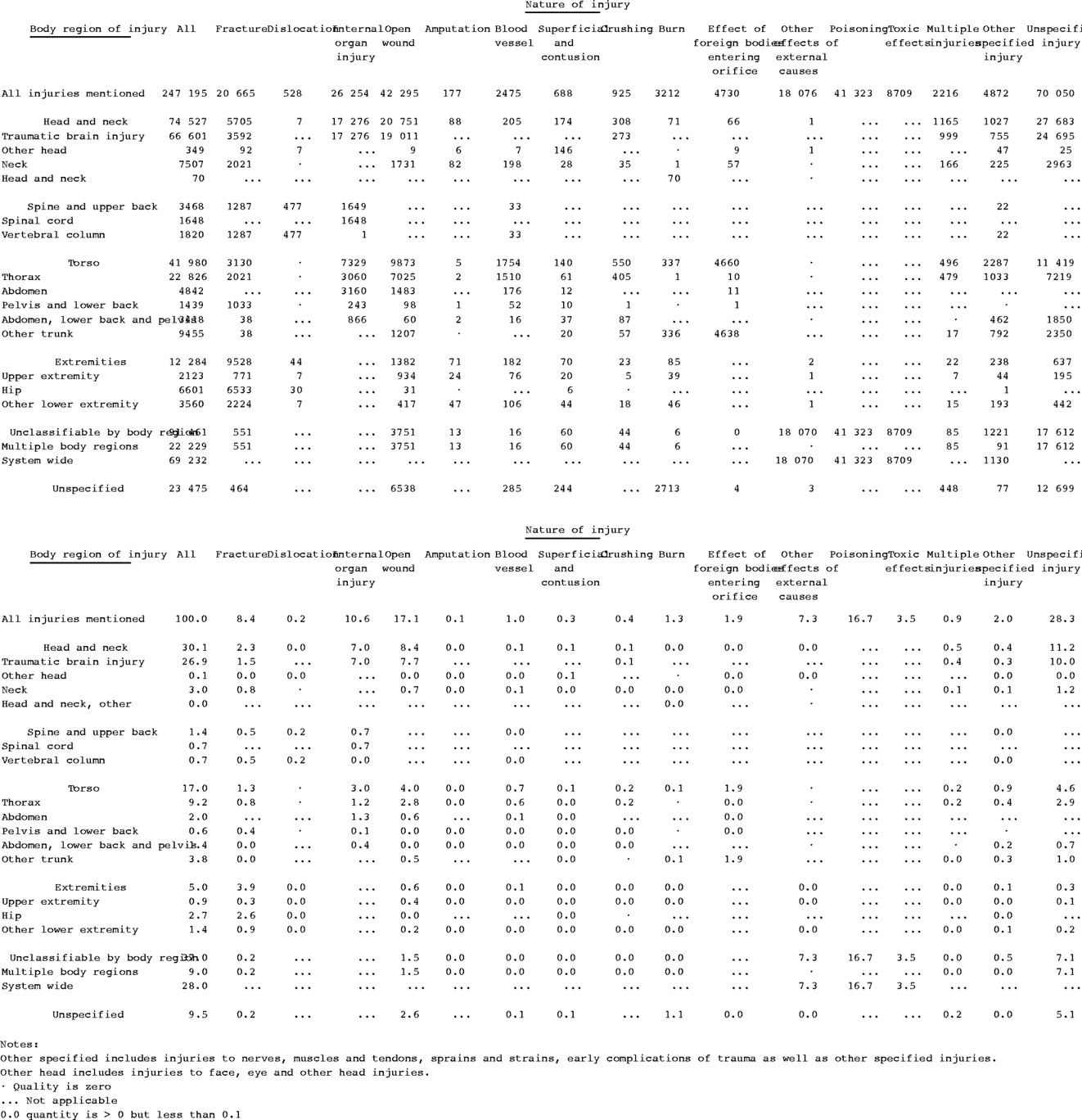
We illustrate the effective presentation of the injury diagnosis mortality matrix using the 2002 US multiple cause of death file produced annually by the National Center for Health Statistics.14 In the data presented in figure 2, the total number of mentions and percent distribution of injury mentions in the matrix are restricted to those deaths for which the underlying cause was an injury (*U01-*U03, V01-Y36, Y85-Y87, Y89) as defined elsewhere.1
{kind=link}
{kind=link}
Total mentions of injuries and percent of injuries classified by the ICD-10 injury mortality diagnosis matrix among all deaths with an underlying cause of injury: US, 2002.
RESULTS
In 2002, there were 247,195 injury diagnoses mentioned on death certificates where an external cause of injury was the underlying cause of death (n = 161,269 deaths), for an average of 1.5 injuries mentioned per death. This ratio varied by intent and by mechanism of injury. Details of those differences are reported elsewhere.14
Head and neck accounted for 30% of all injury diagnoses mentioned with the vast majority classified as TBI. TBI injuries were primarily spread across injuries of unspecified nature (11%), open wounds (8%), internal organ injuries (7%) (fig 2). “System wide” injuries accounted for 28% of the injury diagnoses mentioned. These include poisoning (17%), other effects of external causes (that is, submersion or asphyxiation) (7%), and toxic effects (nearly 4%).
Seventeen percent of all injury diagnoses were to the torso, 9% were to the thorax region of the torso. A third of the thorax injuries were open wounds and another third were classified as unspecified nature of injury. Extremity injuries accounted for only 5% of all injuries mentioned while spinal cord and vertebral column were even less likely to appear on death certificates.
By nature of injury, open wounds accounted for 17% of all injury diagnoses mentioned, and 45% of all open wounds were classified as TBIs. The nature of injury was unspecified for 28% of injury diagnoses mentioned compared with 9.5% of all injury diagnoses having no body region specified.
CONCLUSION
The IMD mortality matrix is a framework for presenting diagnosis specific mortality data. The Barell matrix was initially designed for non-fatal injury data involving both single and multiple diagnoses.3 The IMD matrix is designed for mortality data also using either single or multiple diagnoses (generally dependent on what is available from a country’s dataset).
If a single injury is selected from among multiple injury diagnoses in the data (for example, first listed, primary diagnosis, or main injury), presentation using the matrix is uncomplicated. However, important information may be lost when analyzing by a single injury. For example, events involving multiple injuries may be more severe than those involving a single injury. Multiple injury profiles show combinations of injury diagnoses by body region, nature of injury, or cross classification of the two.6 As they present the commonly occurring combinations, they are useful to describe multiple cause data.
Key Points
-
The ICD-10 injury mortality diagnosis (IMD) matrix was developed to be as similar to the Barell matrix as possible given the differences in data quality and coding systems between morbidity and mortality data.
-
Having a uniform method of categorizing injury diagnoses is important for comparative analyses.
-
At its most detailed level, the ICD-10 IMD matrix has 20 nature of injury categories and 43 body region categories.
-
To maintain consistency with the external cause of injury mortality matrix (for both ICD-9 and ICD-10), adverse effects, not elsewhere classified (T78), and complications of surgical and medical care, not elsewhere classified (T80–T88) as well as their sequelae (T98.3) were excluded from the ICD-10 IMD matrix.
In about a third of the injury deaths in the US, there is more than one injury diagnosis listed as contributing to the death.1 Given the range in the training and experience of the certifiers, we believe there is variability in the way death certificates are completed. For example, in the case of a motor vehicle crash, some certifiers will write down a single injury, (for example, crushed chest), some certifiers will write down each injury sustained (for example, open wound of chest, fractured rib, fractured femur), while others will record “multiple injuries”. Choosing to present total injury diagnoses mentioned is a straightforward method albeit not the only one.
For countries that have their own clinical modification of ICD-10, the matrix presented here will need to be modified to be compatible with morbidity data and expanded to accommodate the additional codes. However, basic differences between the mortality and morbidity matrices will remain until causes of death are better documented. For example, the “open wounds to the head” in the mortality data will be classified as TBI and in morbidity data will be classified to other head injuries.
More detail on the matrix can be found in the 2002 annual report on injury mortality from the National Center for Health Statistics.14 The injury mortality diagnosis data provide a systematic approach for presenting the myriad of injury diagnoses in the International Classification of Diseases.
Acknowledgments
Richard Hockey of the Queensland (Australia) Injury Surveillance Unit for initial guidance, Ted Miller of the Pacific Institute for Research and Evaluation for programming assistance; Robert Anderson, Ari Minino, and Ken Kochanek of the Mortality Statistics Branch of NCHS for comments on the matrix, and to the members of the International Collaborative Effort on Injury Statistics for reviewing early drafts of the matrix.
Supplementary materials
Files in this Data Supplement:
- view PDF - Figure 1. ICD-10 codes used to define cells of the injury mortality diagnosis (IMD) matrix.
Linked Articles
- Correction