
Abstract
Background
Practice variation is common for nephrotic syndrome (NS) treatment.
Methods
A cross-sectional, web-based survey on NS treatment was administered to 58 Canadian pediatric nephrologists with the aim to document existing practice variation and compare practice with the recommendations of the Kidney Disease Improving Global Outcomes Clinical Practice Guideline for NS.
Results
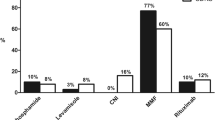
Of the 58 nephrologists asked to participate in the survey, 40 (69 %) responded. Among these, 62 % prescribed initial daily glucocorticoid (GC) therapy for 6 weeks, 26 % for 4 weeks by 26 %, and 10 % prescribed ‘other’. Alternate-day GC was continued for 6 weeks by 63 % of respondents and for >6 and <6 weeks by 32 and 6 %, respectively. For biopsy-confirmed minimal change disease, 65 and 46 % of respondents chose oral cyclophosphamide for frequently relapsing and steroid-dependent phenotypes, respectively; calcineurin inhibitors or mycophenolate were the second most popular choices. Kidney biopsy was ‘always’ performed by 16, 39, and 97 % of respondents for frequently relapsing, steroid-dependent, and steroid-resistant patients, respectively. Rituximab had been administered by 60 % of respondents; 22, 56, and 72 % reported that they would consider rituximab for frequently relapsing, steroid-dependent, and steroid-resistant patients, respectively. Most notable differences between practice and Guideline recommendations were first presentation GC duration, GC-sparing agent choices in frequently relapsing and steroid-dependent patients, and biopsy practices.
Conclusions
There is substantial Canadian practice variation in NS treatment. Assessment of factors driving variation and strategies to implement Guideline recommendations are needed.



Similar content being viewed by others


References
Gipson DS, Massengill SF, Yao L, Nagaraj S, Smoyer WE, Mahan JD, Wigfall D, Miles P, Powell L, Lin JJ, Trachtman H, Greenbaum LA (2009) Management of childhood onset nephrotic syndrome. Pediatrics 124:747–757
Churg J, Habib R, White RH (1970) Pathology of the nephrotic syndrome in children: a report for the International Study of Kidney Disease in Children. Lancet 760:1299–1302
Churg J, Habib R, White RH (1979) Alternate-day versus intermittent prednisone in frequently relapsing nephrotic syndrome. A report of "Arbetsgemeinschaft fur Padiatrische Nephrologie". Lancet 1:401–403
Ehrich JH, Brodehl J (1993) Long versus standard prednisone therapy for initial treatment of idiopathic nephrotic syndrome in children. Arbeitsgemeinschaft fur Padiatrische Nephrologie. Eur J Pediatr 152:357–361
Lande MB, Leonard MB (2000) Variability among pediatric nephrologists in the initial therapy of nephrotic syndrome. Pediatr Nephrol 14:766–769
MacHardy N, Miles PV, Massengill SF, Smoyer WE, Mahan JD, Greenbaum L, Massie S, Yao L, Nagaraj S, Lin JJ, Wigfall D, Trachtman H, Hu Y, Gipson DS (2009) Management patterns of childhood-onset nephrotic syndrome. Pediatr Nephrol 24:2193–2201
Hodson EM, Willis NS, Craig JC (2008) Non-corticosteroid treatment for nephrotic syndrome in children. Cochrane Database Syst Rev (1):CD002290. doi:10.1002/14651858.CD002290.pub3
Haute Autorité de Santé (2008) Syndrome néphrotique idiopathique de l’enfant. Protocol national de diagnostic et de soins pour une maladie rare. Haute Autorité de Santé, Saint-Denis La Plaine, pp 1–22. Available at: www.has-sante.fr
Bagga A, Ali U, Banerjee S, Kanitkar M, Phadke KD, Senguttuvan P, Sethi S, Shah M (2008) Management of steroid sensitive nephrotic syndrome: revised guidelines. Indian Pediatr 45:203–214
Kidney Disease Improving Global Outcomes (KDIGO) Glomerulonephritis Work Group (2012) KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl 2:139–274
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, Robinson N (2006) Lost in knowledge translation: time for a map? J Contin Educ Health Prof 26:13–24
Grol R (2001) Improving the quality of medical care: building bridges among professional pride, payer profit, and patient satisfaction. JAMA 286:2578–2585
McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, Kerr EA (2003) The quality of health care delivered to adults in the United States. N Engl J Med 348:2635–2645
Straus SE, Tetroe J, Graham I (2009) Defining knowledge translation. CMAJ 181:165–168
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med 147:573–577
Hodson EM, Willis NS, Craig JC (2007) Corticosteroid therapy for nephrotic syndrome in children. Cochrane Database Syst Rev (1):CD001533. doi:10.1002/14651858.CD002290.pub3.
Hirano D, Nishizaki N, Kanai H, Hara S, Ohtomo Y, Umino D, Fujinaga S (2010) Long-term outcome of children treated with the ISKDC regimen for the first episode of INS. Nihon Jinzo Gakkai Shi 52:1029–1036
Hussain F, Mallik M, Marks SD, Watson AR (2010) Renal biopsies in children: current practice and audit of outcomes. Nephrol Dial Transplant 25:485–489
Magnasco A, Ravani P, Edefonti A, Murer L, Ghio L, Belingheri M, Benetti E, Murtas C, Messina G, Massella L, Porcellini MG, Montagna M, Regazzi M, Scolari F, Ghiggeri GM (2012) Rituximab in children with resistant idiopathic nephrotic syndrome. J Am Soc Nephrol 23:1117–1124
Eddy AA, Symons JM (2003) Nephrotic syndrome in childhood. Lancet 362:629–639
Greenbaum LA, Benndorf R, Smoyer WE (2012) Childhood nephrotic syndrome–current and future therapies. Nat Rev Nephrol 8:445–458
Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, Rubin HR (1999) Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 282:1458–1465
Grimshaw JM, Shirran L, Thomas R, Mowatt G, Fraser C, Bero L, Grilli R, Harvey E, Oxman A, O’Brien MA (2001) Changing provider behavior: an overview of systematic reviews of interventions. Med Care 39:II2–45
Campbell H, Hotchkiss R, Bradshaw N, Porteous M (1998) Integrated care pathways. BMJ 316:133–137
Panella M, Marchisio S, Di Stanislao F (2003) Reducing clinical variations with clinical pathways: do pathways work? Int J Qual Health Care 15:509–521
Rotter T, Kinsman L, James E, Machotta A, Gothe H, Willis J, Snow P, Kugler J (2010) Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev (3):CD006632. doi:10.1002/14651858.CD006632.pub2
Acknowledgments
We sincerely thank all the Canadian pediatric nephrologists who completed the online survey regarding their management practices in childhood nephrotic syndrome. We gratefully acknowledge the support provided by the Canadian Kidney Knowledge Translation and Generation Network and the Canadian Association of Pediatric Nephrologists in the conduct and completion of this study.
Disclosures (funding)
SS received salary award support from the Kidney Research Scientist Core Education and National Training Program (Kidney Foundation of Canada, Canadian Institutes for Health Research, Canadian Society of Nephrology) and Canadian Child Health Clinician Scientist Program. MZ received salary support from the Fonds de Recherche du Québec–Santé.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Samuel, S., Morgan, C.J., Bitzan, M. et al. Substantial practice variation exists in the management of childhood nephrotic syndrome. Pediatr Nephrol 28, 2289–2298 (2013). https://doi.org/10.1007/s00467-013-2546-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-013-2546-0