

Abstract
Background: Peer support can address the informational and emotional needs of people living with chronic kidney disease (CKD) and enable self-management. We aimed to identify preferences and priorities for content, format and processes of peer support delivery for patients with non-dialysis CKD and their loved ones.
Methods: Using a patient-oriented research approach, we conducted a half-day, virtual consensus workshop with stakeholder participants from across Canada, including patients, caregivers, peer mentors and clinicians. Using personas (fictional characters), participants discussed and voted on preferences for delivery of peer support across format, content and process categories. We analyzed transcripts from small- and large-group discussions inductively using content analysis.
Results: Twenty-one stakeholders, including 9 patients and 4 caregivers, participated in the workshop. In the voting exercise on format, participants prioritized peer mentor matching, programming for both patients and caregivers, and flexible scheduling. For content, participants prioritized informational and emotional support focus, and for process, they prioritized leveraging kidney care programs and alternative sources (e.g., social media) for promotion and referral. Analysis of workshop transcripts complemented prioritization results and emphasized tailoring of peer support delivery to accommodate the diversity of people living with CKD and their support needs. This concept was elaborated in 3 themes, namely alignment of program features with needs, inclusive peer support options and multiple access points.
Interpretation: We identified preferences for peer support delivery for people living with CKD and underscore the importance of tailored, flexible programming in this context. Findings could be used to develop, adapt or study CKD-focused peer support interventions.
Plain language summary: In this virtual workshop, patients, caregivers, peer mentors and clinicians across Canada discussed and voted on priorities for delivery of peer support for people with kidney disease. The top identified priorities included matching patients with similar peer mentors, flexible programming, increased program access and distinct caregiver supports.
People living with complex chronic conditions are tasked with self-managing their health.1,2 For the around 10% of adults in Canada with chronic kidney disease (CKD),3 unique challenges include balancing dietary guidance, medication burden and lifestyle strategies to slow progression of their disease with other competing priorities.2,4–6 Although multidisciplinary care models for CKD are well suited to supporting patients’ medical and informational needs, particularly among those at high risk of kidney failure,7–9 support gaps persist owing to factors such as time-constrained clinic visits, the dynamic trajectory of CKD and the care team’s lack of lived experience of the condition.10,11
Peer support offers a complementary approach to supporting patients’ emotional needs, validating their concerns and sharing knowledge through structured interactions with others with similar health-related experiences.12 Given the national interest in strategies to enhance self-management of chronic disease and patient-centred care, opportunities to integrate peer support into comprehensive kidney care models are being increasingly sought.13 Among people with non-dialysis CKD, formalized peer support can establish a sense of community and equip them with knowledge and confidence to face an often-uncertain future.14–16 However, little is known about the extent to which formalized peer support meets the needs for people living with advanced, non-dialysis CKD, whose disease experiences can differ substantially from those with kidney failure or those who receive kidney replacement therapy (i.e., dialysis or transplantation). In the context of our broader, patient-oriented research program, the aim of this stakeholder consensus workshop was to identify preferences and priorities related to delivery of peer support for patients with CKD and their caregivers in Canada.
Methods
Study design and setting
We held a half-day virtual workshop in June 2021 using the Zoom online platform to engage stakeholders in a modified nominal group technique. This established, consensus-building approach aims to generate and prioritize ideas by experts in the topic area over a series of group discussions (Appendix 1, Section 1, available at www.cmajopen.ca/content/11/4/E736/suppl/DC1).17,18 During the workshop we referred to 6 unique personas (i.e., fictitious descriptions of potential users),19 developed previously in partnership with patients to prompt discussion about needs and preferences related to the content, format and processes of delivery of formalized peer support (Appendix 1, Section 2).4,20 We reported this work in accordance with the Guidance for Reporting Involvement of Patients and Public (GRIPP2)21 and the Consolidated Criteria for Reporting Qualitative Research.22
Participants
We recruited adult participants aged 18 years or older who were comfortable communicating in English from one of the following stakeholder groups: people living with non-dialysis CKD, informal caregivers (e.g., family members, friends), clinicians and other relevant stakeholders with an understanding of CKD and interest in peer support, and peer mentor volunteers from the Kidney Foundation of Canada. We purposively recruited participants from across Canada using established partnerships with the Canadians Seeking Solutions and Innovations to Overcome Kidney Disease (Can-SOLVE CKD) patient-oriented research network and the Kidney Foundation of Canada.23 We identified additional participants from previous qualitative work in the non-dialysis CKD population who had consented to be contacted about future research (including those who had progressed to kidney failure).24 Our organizational contacts and research coordinator distributed email invitations to eligible adults, and those responding with interest were contacted by the research team to discuss the project and obtain consent. We sampled purposively across stakeholder roles to ensure sample diversity and aimed for 20–25 participants, which is acceptable for a virtual, consensus-based exercise.4,13
Study procedures
Two weeks before the workshop, we distributed materials by email, including a summary of the topic area, personas and a workshop overview. We asked participants to review the personas, consider how they might access peer support and reflect on how their own experiences may have shaped their views. Research team members were available by email or telephone for assistance. All participants completed a questionnaire to summarize their demographic characteristics.
At the start of the workshop, the main facilitator (M.J.E.) welcomed participants, provided a program overview and established expectations for respectful interactions. Over a series of 3 small-group sessions (each including 6–8 participants across stakeholder groups),25 participants discussed needs for delivery of peer support in relation to the personas. Small-group sessions were facilitated by team members (M.D., J.F., N.V.) with advanced training in focus group and workshop methodology and who were skilled in guiding balanced discussion across stakeholder roles. They referred to a topic guide (Appendix 1, Section 3) and prompted participants to assume the perspectives of the personas during discussions on 3 topic categories (content, format, process) identified from previous work and related frameworks of intervention reporting.15,26 We encouraged participants to contribute perspectives relevant to their role. Facilitators took measures to ensure equitable contributions of workshop participants to the discussion, including inviting individual participants to share their thoughts, probing the group for alternative views, respectfully redirecting the conversation to another participant or issue if anyone was dominating the discourse and ensuring discussions centred on the personas rather than overemphasizing any one participant’s perspectives. After each small-group session, facilitators presented a summary of their group’s ideas to the larger group and solicited feedback. Before the final prioritization exercise, the research team consolidated and categorized preferences discussed during the workshop. We used cumulative dot voting,27,28 whereby participants used the annotation feature of Zoom to vote anonymously on 3 individual ideas or suggestions under each of the 3 categories that they considered most important for peer support delivery for people living with advanced CKD (i.e., up to 9 votes per participant). All sessions were audio-recorded and transcribed. After the workshop, we emailed participants a survey assessing their satisfaction with the format and process (Appendix 1, Section 4).
Patient engagement
Two patient partners (N.V., D.S.) with lived experience of kidney disease collaborated on the design, conduct, interpretation and reporting of this project. Both contribute to our group’s self-management and peer support–related research initiatives within the Can-SOLVE CKD Network. One patient (N.V.) with qualitative research training and experience facilitated small-group sessions, and one (D.S.) participated in data collection (i.e., workshop participant). Patient partners reviewed final outputs and contributed to manuscript preparation. About 1 month after the workshop, all participants (including patients) had the opportunity to provide feedback and request clarification on a summary of findings circulated by email.
Data analysis
We summarized demographic and workshop data descriptively. To rank preferences within each category, we tallied the number of votes and ranked results as high (≥ 7 votes), medium (3–6 votes) and low (< 3 votes) priority, established a priori based on the anticipated number of participants and selections available within each topic area.1 Two research team members reviewed field notes and transcripts to verify that all key features raised during discussions were captured in the voting exercise. We summarized responses from the satisfaction survey descriptively.
We uploaded transcripts from small- and large-group sessions to NVivo 12 (QSR International) to facilitate data organization. Three research team members (M.J.E., S.L., B.B.) reviewed and inductively analyzed deidentified transcripts using conventional content analysis to identify themes related to delivery of peer support that were prioritized by stakeholders.29–31 Each team member independently reviewed transcripts, highlighted meaningful segments of text and developed initial codes using the first small- and large-group discussion. We discussed, refined and applied final codes to the remaining transcripts, from which we derived themes with representative quotes. We referred to our field notes about the interactions between workshop participants to refine our analysis and ensure that final themes reflected a diversity of participant roles and viewpoints. We ensured methodological rigour through a reflexive approach to data collection and analysis, researcher and data triangulation, and provision of rich descriptions to support our findings.32
Ethics approval
This study was approved by the University of Calgary Conjoint Health Research Ethics Board (REB21-0423). All participants provided written informed consent.
Results
The workshop included 21 participants (5 patients, 4 caregivers, 4 peer mentors, 6 clinicians and 2 organizational representatives). Three-quarters of participants were from Alberta (n = 15). Most participants identified as women (n = 16, 76%), were aged 40–64 years (n = 13, 62%) and had a university or professional degree (n = 15, 71%). Patient participants reported a range of CKD causes and disease durations (Table 1). All peer mentors reported having experience of both dialysis and transplantation. Eight participants (4 patients, 2 caregivers and 2 peer mentors) had contributed to previous related qualitative work on kidney disease–related self-management and peer support.
Participant characteristics
Prioritization results
Within the format area, the most highly prioritized options (≥ 7 votes) included matching peer mentors based on characteristics and need for support, offering peer support to both patients and caregivers and ensuring flexible programming to suit the wide variation in people’s needs (Table 2). Conventional formats such as group, one-on-one and telephone sessions were more highly prioritized than virtual, social media or informal activities. With respect to content, participants prioritized informational and emotional support over reassurance and validation (i.e., appraisal support) and assistance with day-to-day tasks. Within the process category, using social media to raise awareness about peer support and facilitating referrals through kidney clinic staff were highly prioritized.
Peer support in chronic kidney disease (CKD) topic areas with suggested options, corresponding dot counts and priority status
Thematic findings
Participants identified the need to individualize or tailor delivery of peer support for people with CKD as an overarching concept across sessions and stakeholder roles. Participants suggested the diversity of people with CKD should be reflected through a variety of flexible options across the format, content and process categories. We characterized 3 themes and provide a thematic summary, supporting quotes, and suggestions to enhance peer support delivery in Figure 1.
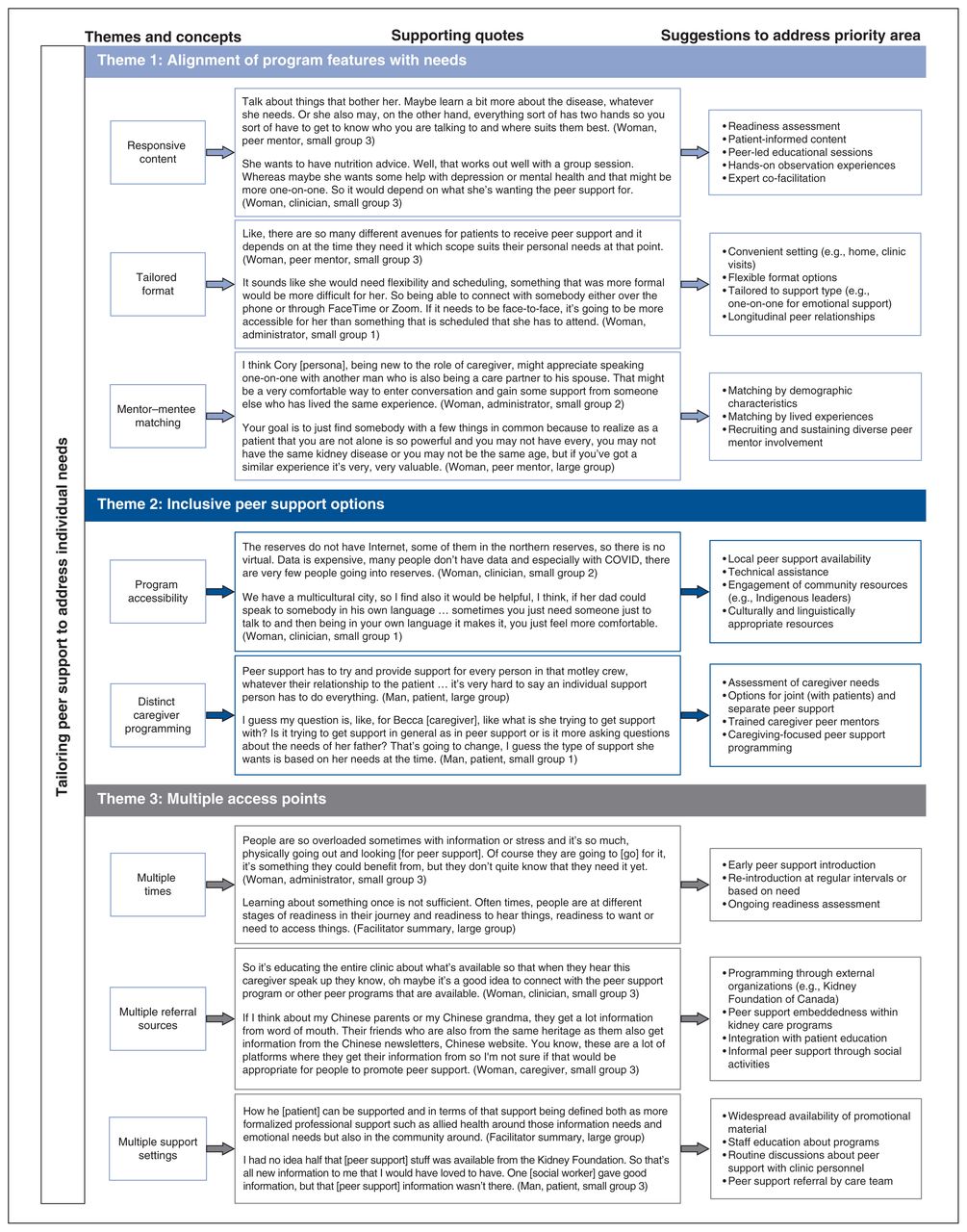
{kind=link}
Thematic summary, supporting quotes and suggestions to address priorities for peer support delivery.
Alignment of program features with needs
Participants suggested that the “what” and “how” of peer support delivery should match an individual’s needs at that moment in time. Perceived need and receptivity for support depended on factors such as disease duration, rate of progression and understanding of their prognosis. For example, whereas patients with a recent diagnosis might benefit from emotional and informational support to promote disease acceptance and understanding, those with progressive disease may turn to peers for assistance with treatment decision-making. Stakeholders emphasized matching peer support users with mentors on defined demographic characteristics when facing relatable life challenges, such as matching the young woman persona who had questions about family planning with another young woman with CKD. Matching based on mentor experiences (e.g., dialysis, transplantation) was considered important when people sought information about what to expect from kidney failure and its therapies. Participants suggested a one-on-one delivery format was better suited to interpersonal connection, whereas structured group sessions with peer facilitation could integrate educational information.
Inclusive peer support options
Participants highlighted challenges in the accessibility of peer support related to the geographic and ethnocultural diversity of people living with CKD in Canada. Several clinicians noted inconsistent access to technology and limited options to connect with peers in rural, remote and Indigenous communities. Stakeholders emphasized a need for peer support programming appropriate to the needs of ethnocultural minority populations. They encouraged peer matching with mentors fluent in patients’ primary languages, engagement of community or faith-based organizations and support resources that respected cultural traditions. A gap in distinct programming for caregivers was noted, whereby access to peer support, independently from their affected loved one and from trained caregiver mentors, could help normalize their experiences and provide strategies for managing in this role.
Multiple access points
Participants acknowledged individuals’ varying levels of disease acceptance and readiness to engage in peer support throughout their illness journey. They prioritized peer support as a complementary strategy to multidisciplinary CKD care at multiple time points and from multiple sources. Although patients may not be ready to access peer support early in their disease course, participants suggested introducing it at diagnosis or upon intake into a multidisciplinary CKD program, revisiting it regularly thereafter and referring patients once they express interest. They also encouraged promotion of peer support by multiple sources, such as care teams and community organizations, and using traditional (e.g., brochures) and nontraditional (e.g., social media) approaches.
Satisfaction survey
Sixteen participants completed a satisfaction survey after the workshop (Appendix 1, Section 4). Although most had a positive workshop experience overall (81%) and appreciated the convenience of the virtual platform (88%), about one-third of respondents suggested that the allotted time was insufficient to comprehensively cover the volume of material.
Interpretation
In our patient-oriented consensus workshop, stakeholders collaboratively identified priorities for delivery of peer support in the non-dialysis CKD context. Top priorities across format, content and process categories included mentor–mentee matching, distinct caregiver programming and engagement of kidney care teams in introducing and referring to peer support programs. Our thematic findings highlight a need for tailored, flexible peer support to mirror the dynamic nature of CKD and patients’ varied experiences. Participants acknowledged potential accessibility challenges and identified repeated program endorsement as a key driver to enhance uptake.
In Canada, the Kidney Foundation has been the main source of kidney-focused peer support that connects any interested individual affected by kidney disease with trained peer mentors using telephone, in-person and virtual formats (i.e., Kidney Connect, https://kidney.ca/support/).33 As highlighted by workshop participants, access to such programs can connect patients with peer mentors who have a breadth of transplant- and dialysis-related experiences to help them navigate their kidney disease trajectory. In contrast, few multidisciplinary CKD clinics embed peer support within their care programs.34 Patients with advanced, non-dialysis CKD often lack overt manifestations yet face challenges related to high symptom burden, metabolic complications, and difficult treatment-related decisions (e.g., choosing among dialysis types).35 Thus, our findings endorse an inclusive but tailored approach to peer support that purposefully addresses CKD-specific support gaps and connects individuals within the broader kidney community. This includes distinct peer support programming for caregivers who experience high physical, mental and financial burden, yet whose needs are often overlooked.36,37
Workshop participants prioritized peer mentor matching based on shared characteristics or circumstances, which can promote bonds and positive social comparisons among people with chronic conditions.12 Some patients with CKD prefer mentors with more advanced disease (e.g., dialysis, transplantation) to help them navigate their disease trajectory,14 whereas others prefer matching on factors such as gender, age or ethnicity, depending on context.38 However, mentor–mentee matching by similarity may not always enhance intervention effectiveness.39 Some have raised questions about its value and impact on the peer support relationship and emphasize instead finding the right fit based on current needs.16,40
Workshop participants highlighted important gaps in access to peer support. Nearly one-fifth of the Canadian population resides in rural or remote areas, among whom recognized disparities in access to kidney-related care exist.41–43 Findings from a scoping review suggest that peer support programs for other chronic conditions are tailored to address both unique issues faced by people living rurally and barriers to access.44 Research on existing support structures, preferences for peer support and barriers to program use for rural- or remote-dwelling people with CKD is needed. Other accessibility issues raised during our workshop (e.g., perceived lack of ethnoculturally appropriate peer support resources) draw attention to the need for community engagement to ensure program inclusivity and culturally safe practices. Approaches to integrating peer support across regional and national providers (e.g., CKD programs, external organizations) and evaluating the effectiveness of peer support are additional knowledge gaps requiring further study.
Limitations
Most patients had limited experience with peer support, yet were engaged in the topic and contributed to the discussion. Although all peer mentors had experience of dialysis or transplant, they contributed important perspectives on peer support delivery for people with non-dialysis CKD. To minimize the influence of social desirability on the discussion and final priorities, skilled facilitators encouraged respectful interactions and input from all participants, and voting was anonymous. As we were unable to determine stakeholder role from audio recordings or dot votes, we could not attribute priorities to specific participant groups and thus present integrated findings. The virtual format may have limited interpersonal connection and interaction, and although participants were satisfied with the format, they suggested that additional time to discuss this nuanced topic would have been helpful. Lastly, participants were English speakers, mostly White, and had Internet access, technological proficiency and high educational attainment. Although accessibility issues were raised, it is possible that participants with different characteristics may have identified additional considerations.
Lessons learned from patient engagement
We used a patient-oriented research approach to address a priority area for patients with CKD and learned from the lived experience of our patient partners through their contributions to study design and conduct. In synthesizing and reporting our findings, patient partners provided suggestions to ensure key messages resonate with nonacademic readers. Importantly, our patient partners are deeply invested in this topic and in improving the lives of people with kidney disease, on which we commit to furthering our collaboration through future work.
Conclusion
In our consensus workshop, patients and other stakeholders prioritized flexibility, tailoring and inclusivity of peer support delivery for people with non-dialysis CKD. These program features should be considered when developing and implementing peer support interventions in this context. Findings will inform future work to enhance supports for people with CKD through continued engagement with patient partners.
Acknowledgements
The authors thank the patient partners and workshop participants from across Canada for contributing their time and perspectives to this work. They also acknowledge Ms. Sabrina Jassemi and Ms. Sarah Gil for their assistance with note taking and technical expertise, respectively, during the workshop. They thank Ms. Corri Robb for her transcription services.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Meghan Elliott, Maoliosa Donald, Nancy Verdin, Danielle Fox and Brenda Hemmelgarn contributed to the conception, design and methodological approach of this study. Meghan Elliott, Maoliosa Donald, Janine Farragher, Nancy Verdin, Shannan Love and Kate Manns contributed to data collection. Meghan Elliott, Shannan Love and Brigitte Baragar undertook data analysis and summarized findings. Nancy Verdin and Dwight Sparkes provided important insight into study findings from their perspectives as patient partners. All author contributed to data interpretation. Meghan Elliott and Shannan Love drafted the manuscript. All authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This project was supported by funds from the Baay Chair in Kidney Health Research at the University of Calgary. Meghan Elliott was also supported by a Kidney Research Scientist Core Education and National Training (KRESCENT) Program New Investigator Award (cosponsored by the Kidney Foundation of Canada and Canadian Institutes of Health Research).
Data sharing: This study used potentially identifiable, participant-level data collected from discussions during a consensus workshop. Our deidentified dataset may be made available upon reasonable request in writing to the corresponding author.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/4/E736/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors