

Abstract
Background: Classroom-based education (CBE) is ubiquitous in postgraduate medical education (PGME), but to date no studies have synthesized the literature on the topic. We conducted a scoping review focusing on academic half days and noon conferences.
Methods: We searched 4 databases (MEDLINE [OVID], Embase [OVID], ERIC [EBSCO] and Web of Science) from inception to December 2021, performed reference and citation harvesting, and applied predetermined inclusion and exclusion criteria to our screening. We used 2 frameworks for the analysis: “experiences, trajectories and reifications” and “description, justification and clarification.”
Results: We included 90 studies, of which 55 focused on resident experiences, 29 on trajectories and 6 on reification. We classified 44 studies as “description,” 38 as “justification” and 8 as “clarification.” In the description studies, 12 compared academic half days with noon conferences, 23 described specific teaching topics, and 9 focused on resources needed for CBE. Justification studies examined the effects of CBE on outcomes, such as examination scores (17) and use of teaching strategies in team-based learning, principles of adult learning and e-learning (15). Of the 8 clarification studies, topics included the role of CBE in PGME, stakeholder perspectives and transfer of knowledge between classroom and workplace.
Interpretation: Much of the existing literature is either a description of various aspects of CBE or justification of particular teaching strategies. Few studies exist on how and why CBE works; future studies should aim to clarify how CBE facilitates resident learning within the sociocultural framework of PGME.
Workplace learning centred on authentic participation in patient care is the foundation of post-graduate medical education (PGME).1,2 Many residency programs supplement learning through regular, scheduled classroom-based education (CBE) by scheduling academic half days or noon conferences. Although workplace learning and CBE complement one another, they often compete for time and attention.3 Residents report an overabundance of “service” training and favour formal learning (“education”) such as lectures over work experience.4 These tensions between service and education in PGME are explored in detail by the experiences, trajectories and reifications (ETR) framework.5 This framework is used for examining practice-based learning in health care settings, wherein a range of situations lead to experiences; individuals’ experiences join to form their different developmental trajectories. The intersection of, and interaction between, individual trajectories in the workplace leads to reification of practice and learning.5 Reification refers to processes and products (objects or artifacts) by which we enact practices.6 One example of this is how residents dictate their discharge summaries, which is both a process and product of their practice. Practice creates, and is created by, recurring activities that are the result of, and shape, our experiences.
Classroom-based education helps to shape the interpretation and reification of clinical experiences.7 For example, residents on call may have a string of experiences, including seeing their first case of lobar pneumonia and presenting at a noon conference. Noon conferences afford opportunities for reflection and knowledge acquisition, and how to learn the more subtle aspects of microbiology and pharmacology. Together, experiences facilitate a trajectory toward being competent as a physician. Repetition of discrete experiences, presented later in the classroom, reifies the importance of overnight call as an educational activity (and not just “service”) and the complementary role of CBE in acquiring deeper knowledge. Although workplace learning theory has been well studied in PGME,8–10 less is perhaps known about CBE and its role. For example, there seems to be no compelling argument for or against CBE in residency, and lectures and other classroom activities are still widely used. Given the uncertainties and gaps in this domain, our research questions for this scoping review were as follows: 1) What is the scope of the literature on classroom-based learning in PGME? 2) What do residents and faculty see as the value of classroom-based learning in PGME? 3) What are the gaps in the literature and priorities for future studies in CBE?
Our literature search focused on retrieval of studies on academic half days and noon conferences, which are common forms of CBE in Canada and the United States.3,11 Postgraduate medicine learning is highly social and participatory, and not focused solely on individual acquisition of knowledge or skills.12 Thus, we examined individual cognitive aspects as well as sociocultural aspects.
Methods
Study design
In our scoping review, we were guided by Arksey and O’Malley’s framework for scoping reviews and, for our reporting, by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) scoping review extension.13–18 We used 5 steps for our review: formulating the research objectives; identifying relevant studies; selecting the studies; charting the data; and collating, summarizing and reporting the results.
Literature search
We iteratively developed searches in consultation with a medical librarian (D.G.) and a peer reviewer who used the Peer Review of Electronic Search Strategies (PRESS) checklist.19 We searched 4 bibliographic databases that index medical education research: MEDLINE and Embase on Ovid, Education Resources Information Center (ERIC) on EBSCO, and the Web of Science Core Collection, from inception to January 2022. We restricted searches to English but imposed no date limits. Search terms included relevant controlled terms and the free-text search phrases: “academic half day*”; morning conference*, noon conference*; flipped classroom*; resident lecture*, etc., and postgraduate medical education (Appendix 1, available at www.cmajopen.ca/content/11/3/E411/suppl/DC1). To increase search sensitivity of highly relevant papers, we performed reference harvesting of key included articles and citation searching in Google Scholar.
Our inclusion criteria were that studies from any publication be primary research examining CBE in PGME. We included qualitative and quantitative studies. We excluded studies if they were not primary research (e.g., editorials) or were not focused on CBE or postgraduate medical learners. Two authors (T.Q. and L.C.) iteratively developed a screening process based on the inclusion criteria to determine the final set of included studies for review. Our review focuses on traditional face-to-face CBE. However, the related topics of simulation, e-learning (or blended learning) and flipped classrooms were not included for 2 reasons: because they are not central in face-to-face teaching and learning, and because high-quality reviews already exist on those topics (e.g., simulation;20 e-learning or blended learning;21,22 and flipped classrooms23–25).
Data analysis
We used 2 frameworks to analyze the included studies. First, we tabulated the articles according to the ETR framework and whether they focused on resident experiences, trajectories or reifications. Within these tables, we also determined where each study best fit in the “description, justification and clarification” framework.26 This second framework addresses the purposes of medical education research. Description studies ask: “What was done?” Justification studies ask: “Did [the intervention] work?” Clarification studies ask: “Why or how did it work?” This framework can be used in parallel with ETR, and to our knowledge, this is the first article to use both. Two authors (L.C. [a clinician educator] and T.Q. [experienced in physical sciences and qualitative educational research]) categorized the included studies; disagreement was resolved by discussion and consensus.
Ethics approval
We did not require ethics approval as all data were available in published records.
Results
We screened 521 full-text studies and identified 90 that met our inclusion criteria (Figure 1). Most included articles were from Canada and the US, 3 from Europe27–29 and 1 from Thailand.30 Three studies reported on collaborations between North American or European and African training programs.31–33 Studies from numerous specialties, such as anesthesia, surgery, pediatrics, internal medicine, family medicine and psychiatry, were included. The results of the review are structured to show whether the purpose of the study can be classified as description, justification or clarification, followed by the main level(s) of analysis in the study according to the ETR framework; and finally, the principal research topics or questions addressed.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram of study identification and selection process. Note: CBE = classroom-based education, ERIC = Education Resources Information Center, PGME = postgraduate medical education.
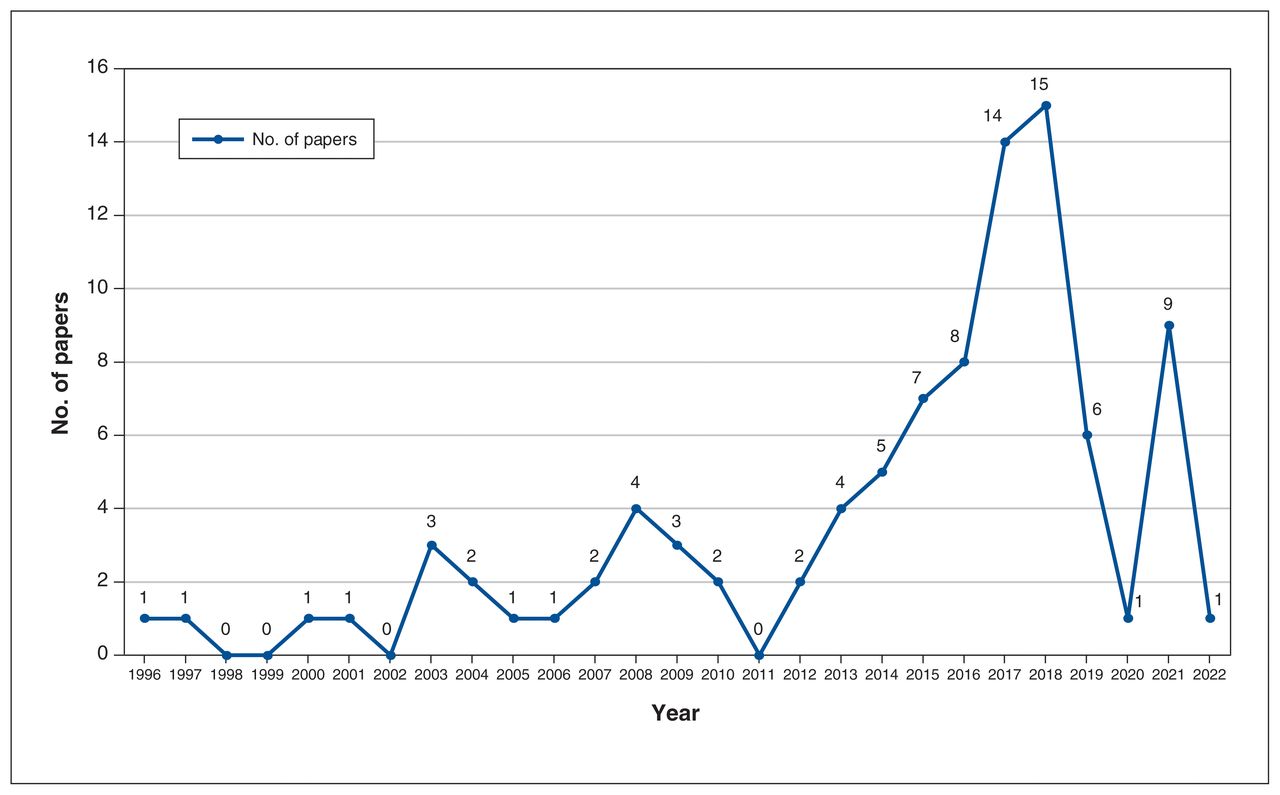
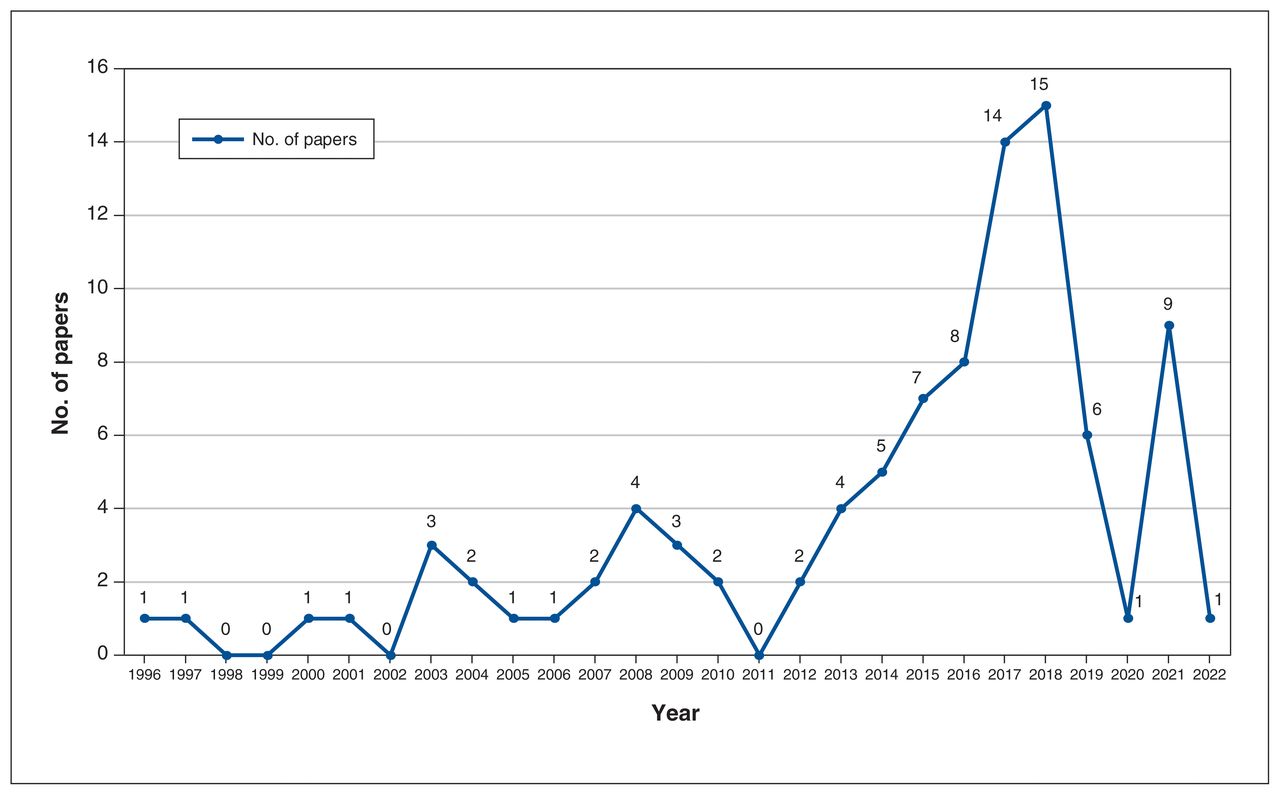
Tables 1, 2 and 3 provide an overview of included studies, grouped and labelled according to the ETR framework. Of these studies, 55 were primarily about resident experiences, 29 about learning trajectories and 6 about reifications. We classified 54 studies as description articles,27,31–83 28 as justification articles11,28,30,84–108 and 8 as clarification articles.3,7,29,109–113 Figure 2 shows the number of included studies published from 1996 to 2022.
Studies focusing on “experiences”
Studies focusing on “trajectories”
Studies focusing on “reifications”
{kind=link}
{kind=link}
Number of included studies (n = 94) published from 1996 to 2022.
Description studies
The level of analysis in nearly all these studies was on trainees’ experiences. Description studies (Table 1) focused on CBE format, such as transitioning from noon conferences to academic half days; some focused on specific content or topics for CBE, and others on the resources required to create and maintain CBE.
Format of CBE
A recurring topic is the merits of blocked versus dispersed formats. Dispersed formats are regular, short (e.g., 30–90 min) sessions such as noon conferences, which occur multiple times a week. Blocked formats such as academic half days are longer and less frequent (e.g., weekly 3- to 5-hour sessions).46 Dispersed formats entail minimal interruption of acute clinical services, as residents are typically onsite at academic hospitals. By contrast, blocked formats require attending physicians or others to cover clinical duties for residents who have 3 or more hours of “protected time.” Blocked formats emerged from American rural family medicine programs in the 1990s as an alternative to dispersed formats, with the purpose of improving attendance and facilitating novel educational methods such as simulation.108,114 Academic half days are relatively common in North America; for example, 20 of 21 Canadian neurology programs had academic half days in 2003,46 and 55.6% of American family medicine programs had them once a year in 2016.45,52 Other broad categories of CBE may include other trainees (e.g., medical students) and faculty with presentations or case discussions. Many programs have a “morning report,” in which a case from the previous call shift or recent admission is discussed.51,75 Morbidity and mortality rounds are an opportunity to discuss adverse events with the intention of improving quality and reducing medical errors.27,44 Many programs include journal clubs to teach evidence-based medicine and to enhance medical literature critical appraisal skills.72
Classroom-based education content and topics
The literature describes specific topics delivered in classrooms, ranging from traditional topics such as insulin pump use39 and psychopharmacologic interventions,54 to competencies such as communication skills and transition to practice.32,67,71 Accreditation Council for Graduate Medical Education and CanMEDS standards are cited often as the impetus for nonmedical expert topics such as global health and surgical safety.67,81
Resources required for CBE
Classroom-based education requires faculty, administrative and infrastructure resources. One academic psychiatry training program implemented “flipped” biannual academic half days for faculty development, wherein residents cover clinical services and faculty members are able to attend faculty development.42 Near-peer and peer-to-peer are effective and decrease faculty teaching load.63,79 One pediatric residency program reported that providing lunch with noon conferences was associated with statistically significant improvements in attendance and punctuality.48
Justification studies
We identified justification studies as surveys and quasi-experimental before-or-after intervention studies that examined the effectiveness of CBE as well as used different teaching strategies (Table 2). The outcomes examined in these studies included in-training examination scores and resident satisfaction. No studies examined patient care outcomes. Most studies focused their analysis on the learning trajectories of residents.
Effectiveness of CBE
Residents reported that they were more likely to attend lectures and pursue self-directed learning when topics were clinically relevant, well presented and focused on clinical reasoning.89 Two studies found a positive association between noon conference attendance and in-training examination scores,93,94 but 4 did not.85,87,90,96 A transition from noon conferences to academic half days was associated with improvements in resident attendance, satisfaction and in-training examination scores.11,86,100 One prospective cohort study comparing dispersed versus massed delivery of a nutrition course for gastroenterology fellows showed better long-term knowledge in the dispersed cohort.99
Teaching strategies
Many studies focusing on teaching strategies were motivated by poor resident attendance, difficulty in planning CBE, and lack of perceived resident and faculty engagement in classroom learning. These studies aimed to revive or refresh attendance and impact of their classroom-based learning by applying principles of andragogy and active learning.50,57,104 Team-based learning improved resident engagement and satisfaction in a pediatrics program.105 The wide availability of Web-based resources has facilitated use of the flipped classroom model in several programs.28,102,103 Videos have been used in CBE to enhance teaching of topics such as bone marrow biopsy and communication skills.81,83
Clarification studies
A few studies were aimed at clarifying issues in CBE (Table 3). These included studies examining the role of CBE in resident education, the perspectives of faculty and residents on CBE, and the issue of learning transfer between classroom and workplace. We found all 3 levels of the ETR framework in the clarification papers, and many focused on the reification of learning in the classroom setting.
The role of CBE in resident education
One of the few multicentre studies examined the transition from noon conferences to academic half days in 3 internal medicine programs.109 This study retrospectively identified 6 core principles for implementation of CBE: protect time and space to facilitate learning, nurture active learning in residents, choose and sequence curricular content deliberately, develop faculty, encourage resident preparation and accountability for learning and employ a continuous improvement approach to curriculum development and evaluation. In identifying these principles, the investigators reified what they intended CBE in their institutions to be.
A qualitative study from internal medicine, orthopedic surgery and hematology showed that residents believe knowledge acquisition is CBE’s primary purpose.3 Specifically, residents believe that learning in the classroom should complement that in the workplace and guide self-directed learning. Moreover, CBE is an important space for social support and forming communities of practice. For residents rotating through many different disciplines and training sites, CBE can provide an academic “home base,” important to their individual professional identity formation.7
Faculty and resident perspectives on CBE
Two studies at the University of Colorado examined faculty perspectives of CBE. In one, faculty said they valued the opportunity to get to know residents in smaller classroom settings, but struggled with ascertaining the optimal content for academic half days and also expressed uncertainty about the long-term impact of their teaching.111 The second study focused on the impact of academic half days on faculty, which included increased difficulty in dealing with ward- and systems-based care issues while residents were away.115 These challenges were amplified by resident absences owing to duty hour restrictions and continuity clinics, highlighting the importance of considering the entire “curriculum” in residency when designing educational experiences. Another qualitative study of internal medicine and internal medicine–pediatrics residents explored learning preferences regarding noon conferences.112 Residents wanted content that was clinically relevant, practical and linked to evidence. They also wanted sessions that were structured around cases and questions, and that used active learning with resident engagement.
Transfer between classroom and workplace
Transfer of learning, defined as “the application and refinement of competencies in a context that is different from that in which the competencies were acquired,” is a challenge.116 Transfer can be affected by characteristics of the classroom (relevance of classroom activities to clinical practice), characteristics of the clinical workplace (attending-resident contact) or resident characteristics (e.g., motivation). One qualitative study examined transfer between the classroom and clinical workplace in first-year general-practice residents in Belgium.29 The study produced 3 key findings: 1) There are 3 distinct phases to the transfer process: a) preparing for transfer of learning; b) being at the workplace and connecting back to classroom-based learning; c) reflecting on transfer of learning and continuing the process. 2) Clarifying who is responsible for transfer of learning is critical. At times, the trainees felt medical teachers and workplace supervisors needed to take more responsibility for transfer of learning, and vice versa. 3) Participants’ conceptions about each phase of the transfer process reflected their opinions about who was responsible for enabling the transfer.
Gregor and Taylor have reviewed the literature on morbidity and mortality rounds, applying experiential learning theory to show how this type of CBE can contribute to individual development of clinical mastery as well as systems-based quality improvement.110
Interpretation
The studies included in our review show that classroom-based learning in PGME is hindered by a lack of an agreed-upon conceptual terminology to describe educational interventions. This lack presents a number of challenges in gathering and studying this literature. For future studies, we propose the use of a more inclusive, umbrella term such as “classroom-based education” to facilitate better alignment of practice and theory, and the labelling of studies.
Further classifying the literature using the ETR and description, justification and clarification frameworks sheds light on which areas may benefit from clarification studies. Almost all description studies focus on experiences offered to residents, such as the format or topic of CBE or residents’ descriptions of their experiences. Several justification studies examined resident learning trajectories, albeit indirectly, through association between residents’ attendance at CBE and their in-training examination scores. Description studies generally examined CBE using an individual, cognitivist lens rather than sociocultural theories of learning.4 Clarification studies focus their analysis at the experience, trajectory or reification level by examining how CBE in residency affects learning and practice and how both interact. For example, resident academic half days, when combined with other resident absences owing to duty hour restrictions and continuity clinics, have unintended system outcomes of emotional strain and patient safety concerns for attending physician faculty members.115
The examination of CBE shows the tensions between residents’ clinical service and their ongoing education. Sociocultural theories such as cultural–historical activity theory, practice architectures and situated learning are highly relevant in understanding these tensions.4 Residents participate in CBE primarily for knowledge acquisition but also for its social aspects, including peer support and forming communities of practice.3 Peters and colleagues are in favour of placing learning in classrooms and workplaces as a contextual, socially mediated process rather than as individual cognitive processes.29 An investigator examining the various topics “covered” in CBE through the lens of cultural–historical activity theory, which uses the educational system rather than the individual learner as the unit of analysis, might ask how the various components of PGME fit together, and what role CBE might play in relation to other components such as workplace learning and self-study.
Classroom-based education should aim to promote the goals of residency programs and residents’ educational needs. Many residents and faculty view CBE as the primary way for training programs to promote their commitment to education.7,117 Activities that occur in the workplace are determined primarily by the needs of patients and health care systems, and only secondarily by the teaching and learning concerns of faculty and residents. The classroom is where faculty can exercise more control over the format and content of teaching, which may be used to carry out accreditation requirements in addition to primary teaching concerns. Both within and beyond these 2 spaces of classroom and workplace, residents can exercise agency in determining their own learning trajectories. Importantly, medical education should complement and enhance rather than thwart the health care system in which it occurs.1
This review has provided a foundation for research into academic half days, noon conferences and CBE in PGME. As a potential future direction, focusing on threshold concepts known as “portals of entry into expertise” during classroom time may present opportunities for meeting faculty and resident goals.118,119 Debriefing to facilitate transfer of learning between simulation and workplace has recently been described120 and could potentially be applied to link the classroom and workplace. The impact of CBE on resident wellness and affective dimensions such as empathy could be explored in future studies.121
Limitations
The protocol for our review was not formally registered. We did not set alerts for the searches. The searches were English only. We included only indexed, peer-reviewed studies and did not search the grey literature for this topic, except for those papers we found during reference harvesting, which may have had a negative impact on our overall yield. We chose the ETR and description, justification and clarification framework to examine this body of research, although other theories, such as the sociocultural theories reviewed by Cleland and Durning,4 would also be relevant to this body of literature.
Conclusion
This review provides an overview of classroom-based learning in PGME and recommends a common vocabulary and framework for future research. Classroom-based learning in PGME has been explored extensively from an individual, cognitivist perspective. Future studies using a sociocultural lens to examine CBE or examining the interplay of CBE with workplace learning may help to clarify the best use of time and resources.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work. Pim Teunissen, Luke Chen, Tien Quach and Riki Dayan contributed to the acquisition, analysis and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Luke Chen’s research is supported by salary support from the University of British Columbia Hematology Research Program for unrestricted educational research.
Data sharing: All data presented are available in the published record.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/3/E411/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors