


Abstract
Background: Topical nitroglycerin (TNG) ointment has been used for almost 3 decades to treat neonatal peripheral tissue ischemia, but this product is now no longer being produced by its Canadian manufacturer. Our aim was to investigate the efficacy and safety of TNG products in newborns in neonatal intensive care units.
Methods: In this systematic review we searched Embase, CINAHL, MEDLINE, PubMed and Web of Science from inception to April 2020 for studies on the use of TNG products (TNG ointment, TNG spray, glyceryl trinitrate [GTN] patch) for the treatment of neonatal tissue ischemia. We did not apply language or study design limitations. Animal studies and duplicate records were excluded. Two reviewers screened and extracted data. The Tool for Evaluating the Methodological Quality of Case Reports and Case Series was used to assess the risk of bias of individual studies.
Results: We included 23 articles (20 case reports, 2 case series and 1 retrospective audit) describing the use of TNG ointment, TNG spray or GTN patch in the treatment of 39 tissue ischemia events in 37 newborns. Twenty-three (62.2%), 12 (32.4%), 1 (2.7%) and 1 (2.7%) infants received TNG ointment, GTN patch, both TNG ointment and GTN patch, and TNG spray, respectively. Nineteen (76.0%) and 7 (53.8%) injuries treated with TNG ointment and GTN patch showed complete recovery, respectively. Two (16.7%) infants treated with GTN patch experienced adverse events (i.e., methemoglobinemia) requiring treatment discontinuation.
Interpretation: TNG ointment presents a safe therapeutic modality for salvage therapy of neonatal tissue ischemia. Engagement of stakeholders is essential to address its recent commercial inaccessibility in Canada.
Newborns admitted to neonatal intensive care units (NICUs) require venous access, with or without arterial cannulation, to meet their therapeutic needs, including hemodynamic and nutritional balance.1 Although vascular catheterization is imperative, peripheral tissue ischemia is a well-described complication.2–6 Peripheral tissue ischemia is attributed primarily to extravasation of intravenous medication, peripheral vasospasm or a thromboembolic event secondary to percutaneous arterial access.7,8 The subsequent tissue injury is associated with substantial morbidity among newborns discharged from the NICU. Evidence on the incidence of tissue ischemia among infants who survive to leave the NICU is variable, but tissue ischemia has been reported in up to 10% of extremely low birth weight (ELBW) newborns, and up to 4% can experience severe tissue injuries.3–6
The current approach to neonatal peripheral tissue ischemia consists of conservative treatment (including removal of the device, elevation of the affected limb and application of warmth to the opposite limb [reflex vasodilation]), pharmacologic therapy (antithrombotic and fibrinolytic agents) and surgical management (surgical thrombectomy). Although pharmacosurgical approaches are promising options in older children, their use in sick newborns is limited because of the high risk of complications7,9
Topical nitroglycerin (TNG) products, which are approved in Canada for the prevention of angina pectoris in adults, have been used off label as salvage therapy for tissue ischemia in newborns since the 1980s, as per neonatal clinical practice guidelines.10–15 The efficacy of TNG appears to result from the vasodilatory effect of nitroglycerin on vascular smooth muscle.16
In July 2018, the sole Canadian manufacturer discontinued the production of TNG ointment, which has resulted in a shortage of this product.17 There is a need to examine the potential impact that this drug shortage may have on vulnerable newborns in Canada. Our aim in this study was to investigate the efficacy and safety of TNG products (TNG ointment, TNG spray and glyceryl trinitrate [GTN] patch) in newborns with peripheral tissue ischemia in NICUs and to explore whether any of the alternative TNG products have an efficacy and safety profile similar to that of TNG ointment.
Methods
Study design
We conducted a systematic review, using the Joanna Briggs Institute Manual for Evidence Synthesis and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements for guidance.18,19 The protocol for this systematic review was not published. The PICO framework used for this review is described in Box 1.
PICO framework
Population: The population of interest was preterm and term newborns in the neonatal intensive care unit who have peripheral tissue ischemia.
Intervention: The intervention was the application of topical nitroglycerin products, defined as nitroglycerin ointment, nitroglycerin spray or glyceryl trinitrate patch, to the area of peripheral tissue ischemia.
Comparison: The comparator was standard of care or any other therapeutic intervention without the application of topical nitroglycerin products (ointment, nitroglycerin spray or glyceryl trinitrate patch).
Outcome: The outcome of interest was the effect of application of topical nitroglycerin products (nitroglycerin ointment, nitroglycerin spray, or glyceryl trinitrate patch) on the area of peripheral tissue ischemia, such as no effect, partial resolution (e.g., loss of finger or toe or reported neurovascular changes in the affected limb) or complete resolution.
Data sources
We systematically searched Ovid MEDLINE (1946–April 2020), PubMed (1809–April 2020), Embase (1974–April 2020), CINAHL (1937–April 2020) and Web of Science (1900–April 2020). The search strategy was developed in MEDLINE (OVID interface) and translated as appropriate for the other databases. The search strategies contained database-specific subject headings and text word terms for the concepts of nitroglycerin and neonatal intensive care. This strategy was developed and peer reviewed using the Peer Review of Electronic Search Strategies (PRESS) guideline in consultation with professional librarians (Appendix 1, available at www.cmajopen.ca/content/9/1/E252/suppl/DC1).20 We searched the bibliographies of relevant articles for additional references. Using Google Scholar, we searched for studies that are not commercially published, such as conference abstracts, dissertations and policy documents.
Study selection
All randomized controlled trials (RCTs), cohort studies, case reports and study abstracts describing the use of TNG ointment, TNG spray or GTN patch in the NICU-based treatment of tissue ischemia in newborns of any gestational age and postnatal age were eligible for inclusion, irrespective of the dose, administration frequency and duration of treatment. We did not apply any language or study design limitations. Animal studies and duplicate studies were excluded. Standard practice or any other therapeutic intervention was the comparator in studies with a control group. If there was no comparator group, the reported efficacy and safety of TNG ointment or GTN patch were extracted.
Data extraction
Following the database searches, 2 reviewers (K.S., S.S-Z.) screened all articles independently and in duplicate at the title and abstract level. They then independently reviewed all full-text articles meeting the inclusion criteria and extracted data. Any disagreements were resolved through discussion with a third reviewer (C.L.). We used a standardized data collection form to extract the relevant data from the included studies (Table 1).
Study design, patient and injury characteristics in studies of the use of topical nitroglycerin ointment, topical nitroglycerin spray and glyceryl trinitrate patch in neonatal peripheral tissue ischemia
Data quality assessment
We used the Tool for Evaluating the Methodological Quality of Case Reports and Case Series21 to assess the risk of bias of individual studies. All studies were independently assessed by 2 reviewers (K.S. and S.S-Z). Disagreements were discussed and resolved among 3 reviewers (K.S., S.S-Z., C.L).
Data analysis
We conducted a narrative synthesis of the study results, the structure of which was based on the modality of nitroglycerin application. For each modality, we described the number of newborns and injuries treated, the time from injury to treatment initiation, the time from application to first effect, the treatment duration, the number of injuries showing complete recovery, adverse events and adjunctive therapy. As none of the included articles reported effect estimate statistics, a meta-analysis was not conducted.
Ethics approval
We did not seek ethics approval as we used publicly available evidence for our study.
Results
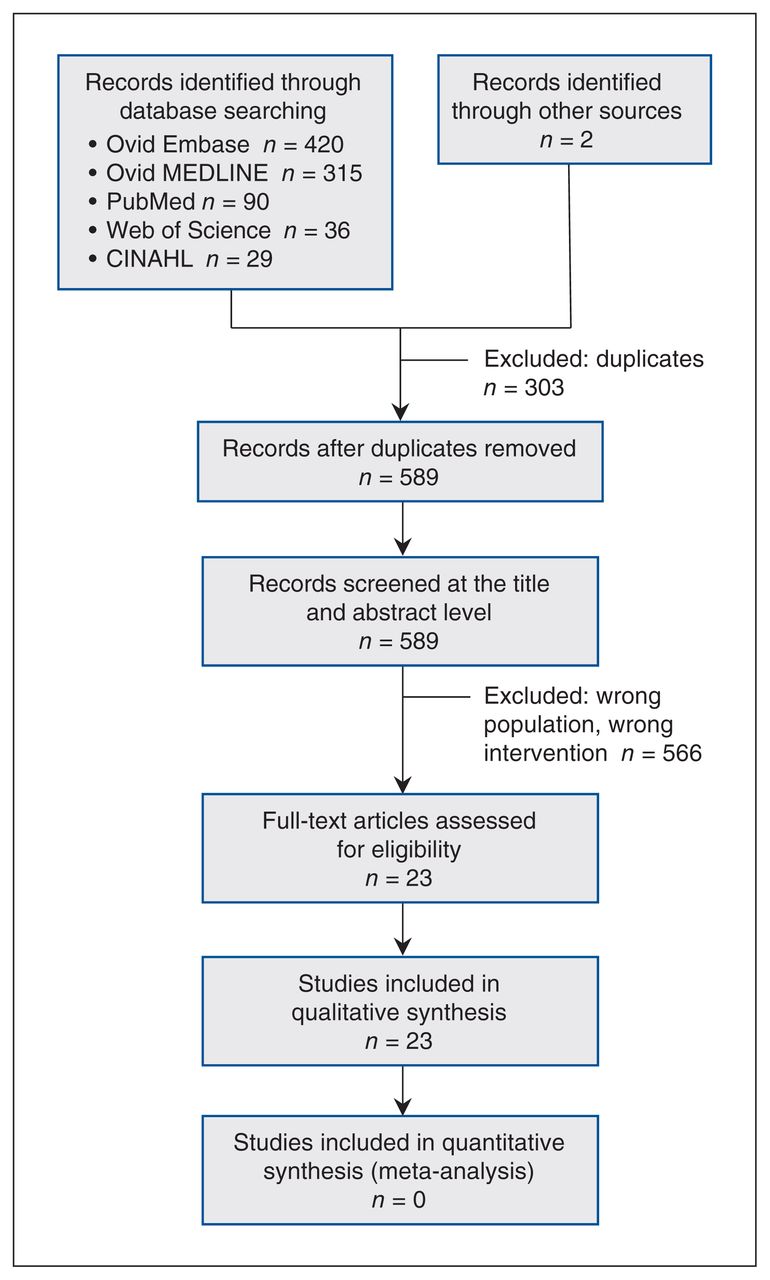
A total of 892 articles were identified (Figure 1). Following removal of duplicates, 589 articles were screened at the title and abstract level and 23 at the full-text level. Twenty-three studies were included in the final review.22–44 Twenty articles were case reports,22–39,41,43,44 2 were case series35,40 and 1 was an abstract of a retrospective audit42 (Table 1, Table 2).
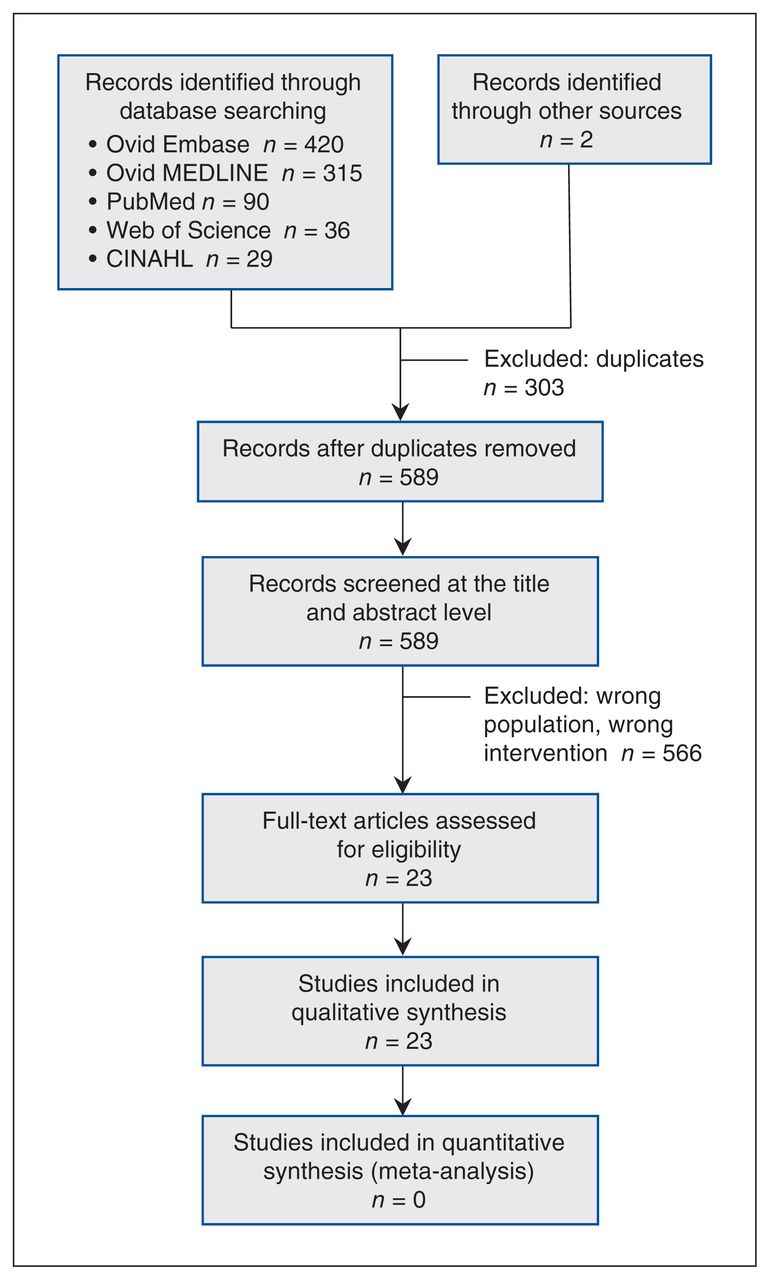
Flow diagram showing the study screening and selection process.
Interventions and outcomes in studies of the use of topical nitroglycerin ointment, topical nitroglycerin spray and glyceryl trinitrate patch in neonatal peripheral tissue ischemia
Characteristics of studies
We identified 23 studies describing 37 newborns with 39 peripheral tissue ischemic events treated with TNG ointment (23 newborns, 62.2%), GTN patch (12 newborns, 32.4%), TNG ointment plus GTN patch (1 newborn, 2.7%) and TNG spray (1 newborn, 2.7%) (Table 1, Table 2). The majority of the newborns were born extremely or very preterm (25 newborns, 67.6%) and were within the first 2 weeks of life at the time of injury (26 newborns, 70.3%). The mean gestational age was 29.1 weeks (range 23 wk to term). Placement of an umbilical artery catheter or peripheral arterial line (PAL) was the most common cause of identified tissue ischemia (22 events, 56.1%), followed by intravenous drug administration (5 events, 12.8%). Mean treatment duration was 10.4 days (range 1 dose to 36 d).
Treatment details
TNG ointment
Twenty-three neonates received TNG ointment for 25 peripheral tissue ischemic events (Table 1, Table 2).22,24,25,27,29,30,32–38,40,43 Initiation of treatment was delayed by up to 6 days. Time from application to first effect varied from 15 minutes to 23 days. Treatment duration ranged from 1 dose to 36 days; 19 (76.0%) injuries showed complete recovery.24,25,27,29,30,32,33,35,37,40,43
Four adverse events were reported in newborns treated with TNG ointment: 3 were mild blood pressure and heart rate changes that resolved without discontinuation of treatment, and 1 was an occurrence of swelling bulla that resolved with the application of Xeroform gauze and limb elevation.25,34,40 Six of the 23 newborns treated with TNG ointment received adjunctive therapy, which included tissue plasminogen activator, heparin, intravenous nitroglycerin, 100% humidity and milrinone.27,29,33,34,36,37 One infant who experienced embolization of a broken arterial catheter tip was first treated by removing the catheter fragment using angiography.33
Four infants with peripheral tissue injury treated with TNG ointment did not experience a complete recovery. They ranged in gestational age from 26 to 34 weeks and experienced a peripheral tissue injury following placement of 1 umbilical venous catheter, 1 PAL, and 2 peripheral intravenous lines.22,34,36,38 Treatment initiation was delayed up to 6 days and treatment duration was up to 21 days. Outcomes ranged from reduced limb movement and reflexes to death.
GTN patch
Twelve newborns received GTN patches for 13 peripheral tissue ischemic events (Table 1, Table 2).23,26,28,31,41,42 Time of application of GTN patch after injury ranged from immediately to 12 hours. Maximum duration of treatment was 7 days; treatment was discontinued in 2 patients because of serious adverse events.26 Seven of the 13 injuries (53.8%) showed complete recovery.23,26,28,31,41,42 Six of the 12 newborns treated with the GTN patch received adjunctive therapies that included enoxaparin, heparin and tissue plasminogen activator.31,42
Two newborns experienced methemoglobinemia subsequent to the use of the GTN patch.26 In both cases, a 9-cm2 patch (18.7 mg) was applied to the sites of injury. The first newborn received 3 GTN patches for 2 tissue ischemic events (1 spontaneous event after birth and 1 event after PAL insertion) over 48 hours. Two patches were applied on the first day of life and the third patch was applied on the second day of life. Within 6 hours following application of the third patch, the infant’s oxygen requirements increased from 21% to 40% and methemoglobin level rose from 1.1% to 8.4%. In the second case, GTN patches were applied for tissue injury following PAL insertion. One patch was applied on the third day of life and changed daily until the seventh day of life, when 2 patches were applied and changed twice daily, with a total of 10 patches used in 5 days. Within 24 hours of the application of 2 patches on the seventh day of life, the infant’s oxygen requirement increased from 23% to 70% and the methemoglobin level increased to 23.3%. Symptoms of methemoglobinemia ceased within 24 hours of patch removal. One other infant experienced a decrease in blood pressure, which resolved with inotropic adjustment.41
GTN patch and TNG ointment
One infant was treated with GTN patch and TNG ointment (Table 1, Table 2).39 The patch was applied to the injury for 5 days as an alternative to TNG ointment as the latter was initially unavailable. Once the ointment became available, the patch was removed and ointment was applied for 11 days, along with an antibiotic cream. Following ointment application, rapid improvement was observed, with increased vascularization and hyperemia of the ischemic tissue. No adverse events occurred throughout treatment with either the patch or the ointment. Following treatment, partial loss of the distal phalange of 1 finger and 1 toe occurred.
TNG spray
One neonate with 2 peripheral tissue injuries (on 1 toe and 1 finger) was treated with TNG spray (Table 1, Table 2).44 Nitroglycerin was sprayed on a compress that was applied to the sites of injury every 8 hours for 7 days. Upon application of the compress, the area of tissue injury became warm, and capillary refill normalized. However, necrosis was still visible on the toe and finger after 7 days, at which time treatment was discontinued. Follow-up at 2 months of age found that the tip of the affected finger and toe had fallen off.
Risk of bias assessment
All included studies were evaluated across 4 domains to determine the risk of selection bias, ascertainment bias, causality bias and reporting bias. Selection and causality were identified as 2 domains through which bias might have been introduced in the majority of studies (Table 3).
Risk of bias assessment
Interpretation
In this systematic review, treatment of tissue ischemic injuries in newborns with TNG ointment appears to be efficacious, with complete recovery of 76.0% of injuries treated with ointment. In the 4 cases in which recovery was incomplete, extenuating circumstances might have mitigated the ointment’s efficacy. In 1 case, the infant had reduced limb movement and reflexes with muscle atrophy at discharge as a result of purple glove syndrome,36 a condition that is known to progress to compartment syndrome requiring fasciotomy, skin grafting or amputation in adults. Several mechanisms have been described for the pathophysiology of this syndrome, from tissue infiltration to venous obstruction secondary to extravasation of a highly alkaline substance (phenytoin).45 Given this complex pathology, application of TNG ointment may not be sufficient in such cases. In the remaining cases, short duration of treatment or prolonged lag time to the start of treatment might have contributed to incomplete recovery.22,34,38
On the basis of the limited available evidence, TNG ointment seems to be well tolerated in newborns, with no serious adverse events identified as being drug related. Reports of mild decreases in blood pressure were in newborns receiving inotropes for hypotension before TNG ointment was applied,25,40 or the low blood pressure resolved spontaneously without intervention. The results of our review point toward the efficacy of TNG ointment for the treatment of neonatal peripheral tissue ischemia. Further investigation through experimental trials is needed to confirm the optimal efficacy–safety profile of this drug.
In contrast, the efficacy profile of GTN patches in this review is less favourable. Although the GTN dose administered in the 2 cases with methemoglobinemia was higher than the doses administered in any of the other studies and the amount of data available is limited, the occurrence of serious adverse events raises concerns about the use of GTN patches in this vulnerable population. Furthermore, there may be less dosing flexibility with a patch than with an ointment, which may increase the risk of adverse events (overdosing) or therapeutic failure (underdosing). As for the TNG spray, evidence is available only for 1 patient and thus conclusions cannot be drawn regarding the efficacy and safety of this product.
Peripheral tissue ischemia is a well-known and serious morbidity among ELBW infants. Given the low weight of these patients and their high rate of comorbidities, most available therapeutic options for older children and adults are less viable in this population. Surgical or radiologic thromboembolectomy is not considered an option for ELBW newborns.46 The use of thrombolytic agents or anticoagulants is a challenge, considering the limited evidence for the use of these treatments among this group and the high risk of adverse events.47,48 Therefore, critically ill neonates in the NICU with a limb-threatening acute event present a therapeutic challenge. Although no randomized controlled trials have been published, the current evidence on the use of TNG ointment in newborns with peripheral tissue ischemia suggests that it has an acceptable efficacy–safety profile.
If TNG ointment remains unavailable in Canada indefinitely, the care of newborns in Canadian NICUs may be adversely affected.49 To our knowledge, this product continues to be marketed in comparable jurisdictions such as the United States and the United Kingdom, where, although it is used off label, it remains available for the prevention of potentially life-altering morbidity in sick newborns.50,51 This drug shortage is a clear example of a how national drug shortage can seriously threaten patient safety and quality of care, especially for the vulnerable patients of NICUs.49
The multistakeholder steering committee on drug shortages in Canada has established guidelines on the best strategies to identify risks and the optimal approaches to address manufacturing-related drugs shortages.52 A collaborative effort by representatives from Health Canada, other federal and provincial government departments and the pharmaceutical industry as well as health care providers is required so that adverse outcomes in this patient population can be avoided.
Limitations
We attempted to collect all available literature on the efficacy and safety of TNG products for salvage therapy of neonatal tissue ischemia. Nevertheless, this review consisted of studies that are at the lowest level of medical evidence and are subject to vulnerabilities such as danger of over-interpretation, publication bias and inability to establish cause–effect relationships. As the evidence on this topic was reported exclusively using case report and case series methodology, we were unable to compare outcomes among infants who were exposed and unexposed to TNG products. We were unable to assign a risk of bias for each included study, as the tool that we used for data quality assessment does not specify a cut-off score.21 Another limitation is that the protocol for our review was not registered or published.
Conclusion
The best currently available evidence suggests that TNG ointment has a favourable efficacy–safety profile in the prevention of morbidities associated with peripheral tissue ischemia in newborns. With the indefinite discontinuation of TNG ointment by the Canadian manufacturer, clinicians treating critically ill NICU patients have lost a valuable therapeutic option, and no good alternative is currently available. Timely engagement of stakeholders is needed to address the severe impact that this important drug shortage might have on the care of newborns in Canada.
Acknowledgements
We thank Megan Fournier and Vivian Bui, pharmacists at McMaster Children’s Hospital, and Dr. Gerhard Fusch, assistant professor in the Department of Pediatrics at McMaster University, for their contributions to the conceptualization of this systematic review. We also thank Jack Young and Denise Smith, librarians at McMaster University’s Health Sciences Library, for their assistance in the development of our electronic search strategies.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All authors contributed substantially to the conception and design of the study, the acquisition of the data and the analysis and interpretation of the data. Katelyn Sushko and Samira Samiee-Zafarghandy drafted the article. All authors revised the article critically for important intellectual content, gave final approval of the version to be published and agreed to act as guarantors of the work.
Data sharing: We used publicly available data for the analysis in this study (detailed in the Methods).
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/1/E252/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 Joule Inc. or its licensors
In this issue

{kind=link}
Article tools





