


Abstract
Background: Patient ambulation is frequently recommended to help prevent venous thromboembolism during hospital admission. Our objective was to synthesize the evidence for ambulation as a prophylaxis for venous thromboembolism in hospital.
Methods: We conducted a systematic review. We searched MEDLINE, Embase, Scopus, Web of Science and Cochrane Central Register of Controlled Trials indexed from their inception through April 2020 for studies of adult patients admitted to hospital, in which ambulation or mobilization alone or concomitant with prophylaxis was indicated for prevention of venous thromboembolism. We searched ClinicalTrials.gov for unpublished trials. We included randomized controlled trials (RCTs) and observational studies. Two reviewers independently screened articles and assessed risk of bias using 2 validated tools. We scored studies on quality of reporting, internal and external validity and study power; combined scores determined the overall quality.
Results: Eighteen articles met the inclusion criteria: 8 retrospective and 2 prospective cohorts, 7 RCTs and 1 secondary analysis of an RCT. The intervention (ambulation or mobilized) groups varied across studies. Five studies examined exercise as a therapeutic prophylaxis for thrombosis and 9 described an ambulation protocol. Five studies attempted to quantify amount and duration of patient ambulation and 3 reported ambulation distance. In the 5 studies rated as good or excellent statistical quality, findings were mixed. Incidence of venous thromboembolism was lowest when pharmacologic anticoagulants were added as part of the prescribed prophylaxis regimen.
Interpretation: We did not find high-quality evidence supporting ambulation alone as an effective prophylaxis for venous thromboembolism. Ambulation should not be considered an adequate prophylaxis for venous thromboembolism, nor as an adequate reason to discontinue pharmacologic prophylaxis for venous thromboembolism during a patient’s hospital admission.
Venous thromboembolism is a global problem, and in the United States alone, it affects up to 600 000 patients annually.1 Prolonged immobility is a cited risk factor for developing venous thromboembolism.2 Randomized controlled trials (RCTs) report significant reductions in venous thromboembolism events among surgical and medical patients who received pharmacological prophylaxis while in hospital.3–5 Clinical practice guidelines describe risk-specific recommendations by patient population,6–9 and accrediting bodies endorse prevention of venous thromboembolism as a top practice for patient safety.10–13
At our hospital, we significantly increased the proportion of patients who were risk assessed for venous thromboembolism and were prescribed risk-appropriate venous thromboembolism prophylaxis,15–18 but also found up to 15% of prescribed doses were not administered to patients admitted to hospital.19,20 Upon surveying health care providers on the wards, we discovered that based on the patient’s ambulation status, many were presenting prophylaxis doses for venous thromboembolism as optional.21,22 Several national and international clinical guidelines recommend ambulation as adequate prophylaxis for venous thromboembolism.7,9 Further, “ambulatory patient” is ubiquitous in electronic medical records as a valid reason for not prescribing prophylaxis for venous thromboembolism.23 To our knowledge, evidence supporting such recommendations is not provided.24,25
Our objective was to synthesize the evidence for ambulation as a prophylaxis for venous thromboembolism among patients admitted to hospital.
Methods
We used the Cochrane Handbook for Systematic Reviews of Interventions26 for guidance in designing and implementing this review.
Data sources and searches
The systematic review protocol was developed by a multidisciplinary group of clinicians, researchers and quality improvement experts focused on venous thromboembolism prevention (Appendix 1 available at www.cmajopen.ca/content/8/4/E832/suppl/DC1). A librarian with a master’s degree in library sciences (S.S.) helped develop the search strategy and search terms consistent with ambulation in patients admitted to hospital (Appendix 1 and Appendix 2 available at www.cmajopen.ca/content/8/4/E832/suppl/DC1). We searched MEDLINE (1948–Apr. 28, 2020), Embase (1980–Apr. 28, 2020), Scopus (Apr. 28, 2020), Web of Science (Apr. 28, 2020) and the Cochrane Central Register of Controlled Trials (Apr. 28, 2020). We hand searched reference lists from included articles. ClinicalTrials.gov was searched for unpublished RCTs (Aug. 27, 2018).
Study selection
Two reviewers (P.M. and A.J.N.) independently screened titles, abstracts and full-text articles in duplicate using inclusion and exclusion criteria and resolved any discrepancies through third-party adjudication. We included studies published in English and with adult patients admitted to hospital, in which ambulation was indicated for venous thromboembolism prevention, either as a single mode of prevention or concomitant with prophylaxis. We included all studies of ambulation for prevention of venous thromboembolism even if the ambulation amount was not quantified by time, distance or frequency. Emed and colleagues found severe heterogeneity in definitions of their exposure variable, “immobility,” used in studies of thromboprophylaxis among patients admitted to medical wards, re-emphasizing the problem of inconsistency in definitions when performing studies without a standard measure.27 We excluded case-series reports, studies not specifying ambulation and studies done in outpatient, intensive care unit or rehabilitation settings. To be inclusive of all possible evidence regarding the efficacy and effectiveness of ambulation to prevent venous thromboembolism, we included both RCTs and observational studies.
Data extraction
Using standardized forms, each reviewer (P.M. and A.J.N.) independently extracted data and convened to compare and resolve any discrepancies. Data were extracted in duplicate from included studies for the following variables: country of origin, study design, patient population, participant characteristics (age, sex), interventions, comparisons, outcome and definition of ambulation.
Data analysis
DistillerSR (Evidence Partners, Ottawa, Canada) was used for screening and data extraction. We planned to conduct a meta-analysis when data were sufficient (from at least 3 RCTs) and studies were sufficiently homogeneous with respect to key variables (population characteristics, study duration and medication dosing).
Assessment of evidence
Two reviewers independently assessed the quality of the included studies and the risk of bias using the Downs and Black tool28 for nonrandomized trials and observational studies recommended by Cochrane (version 5.1).26 To maintain consistency of quality assessment, the Downs and Black tool was also used for assessment of RCTs. Each study was scored on the quality of reporting, both external and internal validity, and study power, and the combined scores determined overall quality (scale: poor, ≤ 14; fair, 15–19; good, 20–25; and excellent, 26–28).
The Agency for Healthcare Research and Quality evidence grading scheme for conducting comparative effectiveness reviews was adapted for use.29
The conclusion of this systematic review was based on a combination of both RCTs and other nonrandomized studies, as it is accepted that systematic reviews can be strengthened with observational studies after considering any study limitations. Evidence described as “high strength” probably reflected an actual effect, “moderate strength” indicated that further research may change the result and “low strength” indicated low confidence in an actual effect and that further research would be very likely to change the result. Insufficient evidence meant no evidence or that the body of evidence had unacceptable deficiencies that precluded a conclusion.
Ethics approval
As this study was solely based on literature, it was not eligible for institutional ethics approval, and none was sought.
Results
Of 20 917 titles identified from the different sources, 6545 duplicates were removed, leaving 14 372 articles. After title, abstract and full-text reviews using inclusion criteria, 14 354 articles were excluded, leaving 18 articles for analysis (Figure 1). Of the included articles, 2 studies were prospective cohort studies;30,31 1 was described as a case–control study, although it was a matched retrospective cohort study;32 7 were retrospective cohort studies involving surgical patients;33–39 and 7 were RCTs40–46 with an additional study of a secondary analysis of the randomized Medical Patients with Enoxaparin (MEDENOX) trial (Table 1).47
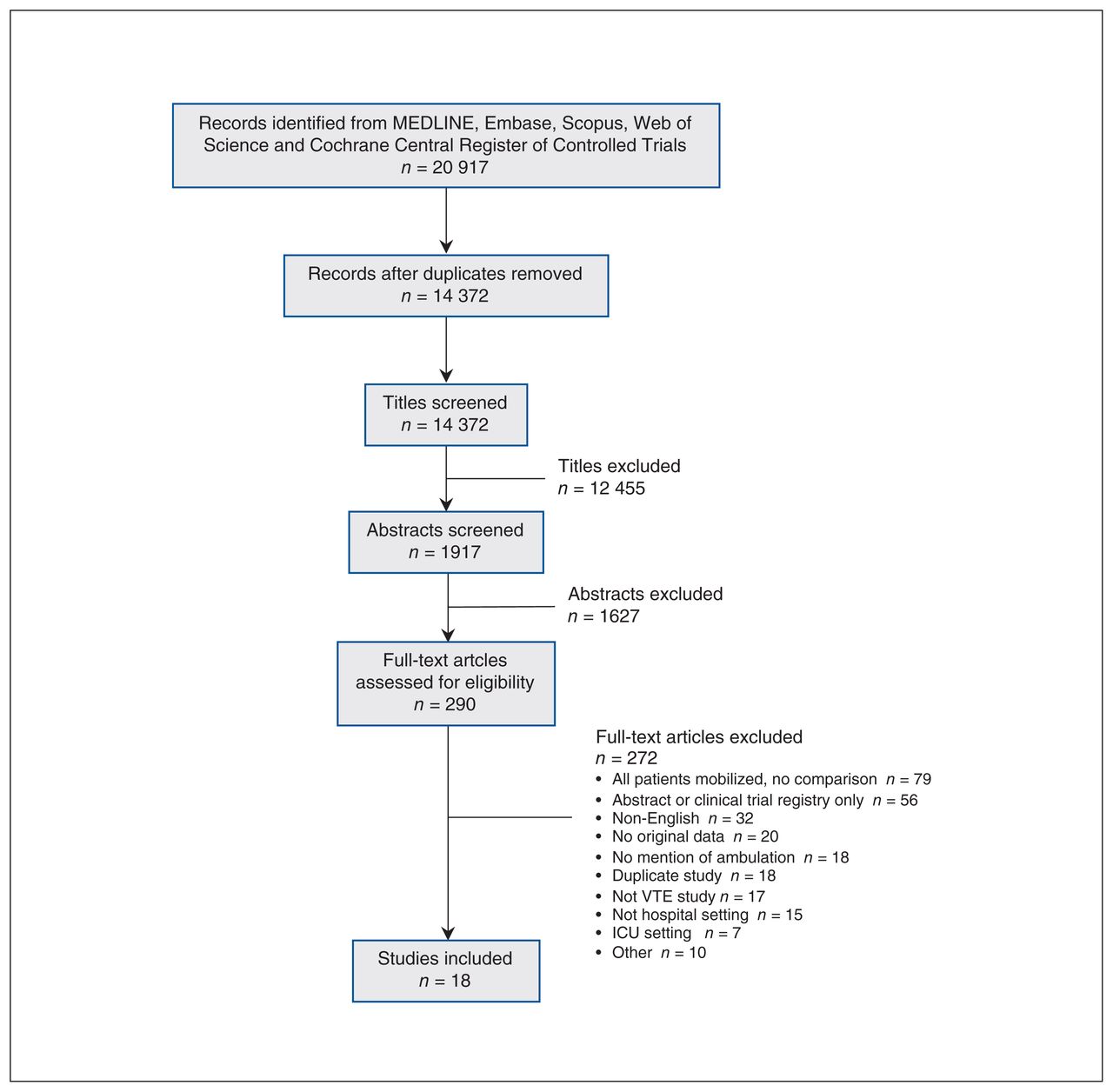
Selection process for studies describing ambulation as a therapy for preventing venous thromboembolism in patients admitted to hospitals. Note: ICU = intensive care unit, VTE = venous thromboembolism.
Characteristics of included studies of ambulation to prevent venous thromboembolism
Study quality and heterogeneity
The studies varied in definitions of both ambulation and outcome (Table 2). The statistical quality ratings for included studies were poor (n = 3), fair (n = 10), good (n = 4) and excellent (n = 1) (Table 3).28 Although 3 studies included a power calculation for the primary outcome, only 1 assessed if the sample size was appropriate to detect a clinically meaningful difference in venous thromboembolism, or appropriately powered if no difference was found.46 A venous thromboembolism event was a secondary outcome in 7 studies.31,32,37,39,42,43,45 The use of pharmacologic prophylaxis for venous thromboembolism varied: 6 studies prescribed prophylaxis for all patients, 8 did not report prophylaxis use, 2 did not use prophylaxis and 2 had different regimens by group. The heterogeneity of studies regarding patient populations, pharmacologic prophylaxis and ambulatory interventions precluded the aggregation of data for meta-analysis.
Results of included studies of ambulation to prevent venous thromboembolism
Quality of included studies and assessment of bias, as evaluated by Downs and Black28
Ambulation definition
The intervention (ambulation) groups varied across studies. Six studies evaluated exercise (in or out of bed) as a therapeutic prophylaxis for thrombosis and 12 described an ambulatory protocol (Table 2). Five studies attempted to quantify the amount and duration of ambulation31,32,36,45,47 and 3 reported the distance of ambulation.36,45,47 Amin and colleagues had the most rigorous definition of ambulation (attain autonomous walking distance > 10 m), although they did not differentiate by time to achieve this measure.47 de Almeida and colleagues quantified ambulation, where ability to walk 3 m independently was the primary outcome.45 Most studies described “early mobilization” or specific prescriptions of mobility, such as twice daily physiotherapy, but failed to report adherence to the defined protocol.
Three studies compared mobility with prolonged immobility. Miller and colleagues compared sitting and standing at the bedside for 30 minutes 3 times a day, starting the first day following myocardial infarction, to 5 days of bed rest,40 Lassen and Borris compared mobilization starting on postoperative day 4 to postoperative day 9,30 and Silver and colleagues compared 12-hour versus 24-hour bed rest following stroke.39
Venous thromboembolism diagnosis
Most studies used clinical suspicion to test for venous thromboembolism, but 8 studies used screening modalities to determine the presence or absence of venous thromboembolism (Table 2). The most common screening modalities were 125I-fibrinogen and phlebography. Most studies failed to clarify the diagnostic modality used to confirm the clinical suspicion, particularly studies in which venous thromboembolism was not the primary outcome. Most studies did not report on pulmonary embolism separately.
Ambulation as prophylaxis
Most studies reported a reduction in venous thromboembolism events with either implementation of an ambulation protocol or promotion of ambulation (Table 2). In the 5 studies rated as good or excellent statistical quality, the findings were mixed (Table 4). Sorbello and colleagues targeted patients admitted to hospital for stroke and found no difference in events among groups (randomized to very early mobilization with physiotherapy v. standard of care).43 Cassidy and colleagues conducted a retrospective analysis using the National Surgical Quality Improvement Program database and found a reduction in events from 3% to 0.8% after introducing a hospital-wide quality improvement protocol for venous thromboembolism.38 The protocol included a standardized risk-stratification protocol combined with a postoperative mobilization program.38 This mobilization program required the patient to be out of bed at least 3 times a day starting the day of surgery and “early ambulation” was encouraged.
Results of included studies rated “good” or “excellent” quality
de Almeida and colleagues compared twice daily graduated exercise protocols to once daily in surgical oncology patients to determine if increased mobility improved functional capacity (ability to walk 3 m), and although events were secondary outcomes, no difference was seen.45 Guo and colleagues evaluated prescribed “functional exercises” including deep breathing, active ankle mobility and calf massage, and although ultrasonography screening was used, there was no difference in the rates of deep venous thrombosis among groups.46
Amin and colleagues’ study best quantified the actual ambulation of medically ill patients and accurately determined the use of pharmacologic prophylaxis for venous thromboembolism (placebo, enoxaparin 20 mg or enoxaparin 40 mg).47 In the ambulatory group, with patients achieving autonomous ambulation more than 10 m, the incidence of venous thromboembolism was 8.4%, which was half the incidence of the group not achieving autonomous ambulation. When pharmacologic prophylaxis (enoxaparin 40 mg) was considered with autonomous ambulation, the incidence of venous thromboembolism was further reduced to 3%. In patients achieving ambulation more than 10 m independently (but not receiving pharmacologic prophylaxis), the event rate was 10.6%.
Two additional studies at higher risk of bias quantified ambulation or exercise. Bhatt and colleagues did not report any venous thromboembolism events in their study of postoperative use of a pedal exerciser.32 Chandrasekaran and colleagues screened all included patients with a duplex ultrasonography on postoperative day 4 and found that patients walking more than 5 m did not have any deep venous thrombosis or pulmonary embolism compared with the control group (32% v. 6% pulmonary embolism, respectively).36
Interpretation
Our systematic review showed a paucity of evidence to support ambulation as an adequate prophylaxis to prevent venous thromboembolism. We found 18 studies over a 69-year span that studied ambulation, most indirectly, to prevent venous thromboembolism; only one-quarter were rated good or excellent quality. We planned a meta-analysis, but the heterogeneity of studies and the varied ambulation definitions made it impossible to quantify any therapeutic ambulation dose.
Four of the 7 RCTs had fewer than 100 patients, and the largest RCT (n = 408) defined ambulation as dorsal and plantar flexion for 1 to 2 minutes every hour.41 The highest quality study did quantify ambulation and conducted a secondary analysis to compare venous thromboembolism rates with and without pharmacologic prophylaxis.47 Although patients achieving autonomous walking in that study had a lower rate of venous thromboembolism events, it is unclear if there were uncontrolled variables to account for this difference. Moreover, the study was designed to investigate the effect of pharmacological prophylaxis on events, which showed a substantial effect in the study. The authors concluded that patients who ambulated more than 10 m independently and received 40 mg enoxaparin had fewer venous thromboembolism events, though the incidence was still 3.3%, and the ambulation-only group had an event rate of 10.6%.47 The only other RCT receiving an excellent quality rating primarily investigated the ability to walk after major oncologic resection, but observed no difference in deep venous thrombosis events among groups.45
Ambulation or mobilization remains a commonly reported approach, often as the sole prophylaxis, against venous thromboembolism. Most concerning is that ambulation is often a cited reason to discontinue pharmacologic prophylaxis for venous thromboembolism. At our hospital, nurses and residents perceived that independently ambulating patients did not need pharmacologic prophylaxis for venous thromboembolism.21,22,48 However, there is overwhelming evidence supporting pharmacologic prophylaxis in nearly every applicable population admitted to hospital.
Immobility is a risk factor for development of venous thromboembolism. However, our systematic review found that mobility, ambulation or mobilization have not been shown to reduce VTE events. Many of the major guidelines recommend early ambulation for prevention of venous thromboembolism. For example, the American College of Chest Physicians recommends early ambulation as the only prophylactic measure needed for low-risk nonorthopedic surgical patients, as measured by the Caprini or Rogers risk assessment tool.49 Our results challenge early ambulation as appropriate prophylaxis for venous thromboembolism. A patient’s risk should be assessed and evidence-based treatment given, considering the risks and benefits. We are not suggesting that ambulation in medical and surgical inpatients is useless. Immobility has many deleterious effects and patients admitted to hospital should be actively encouraged to ambulate. Based on our results, however, we caution the use of ambulation as the sole prophylaxis for prevention of venous thromboembolism or as the impetus to hold pharmacological prophylaxis when ill patients are in a hypercoagulable state.
Although diagnostic and preventive practices for venous thromboembolism have evolved, we searched decades back because the concept of ambulation is long-lived and we needed to find where the concept originated. As early as 1951, Leithauser and colleagues described the “abuse of ambulation.”50 They suggest, and we agree, that early ambulation is not having the patient “dangle the feet over the edge of the bed or sit in a chair.”50 Several studies in our review described sitting or standing as ambulation.40,43 Cassidy and colleagues counted walking to the washroom as 1 of 3 required mobilization events,38 and Sorbello and colleagues defined ambulation as sitting or standing within 24 hours.43 Rather, the attending physician should prescribe ambulation therapy, including timing, frequency and duration, and the prescribed ambulation should be monitored to ensure the patient undertakes it. The results of our review suggest that such a program has not been studied.
Limitations
While comprehensive, our review was limited by the quality of the literature. The RCTs were small and often rated as low quality, and most were negative studies. Most studies failed to define the quality and quantity of ambulation. Older studies did not report or did not use pharmacologic prophylaxis for venous thromboembolism. Therefore, the results must be considered in the modern practices of prevention, which include pharmacologic prophylaxis for venous thromboembolism for most patients admitted to hospital.
We considered only studies published in English and only the ClinicalTrials.gov registry for unpublished studies; it is possible that we failed to identify a relevant study.
Further, most studies were eliminated after title or abstract review, and we may have missed studies with ambulation as a secondary intervention or venous thromboembolism as a secondary outcome. Systematic reviews that find little to no evidence are still important to perform and publish. This key step is critical to delineate clear gaps in the published literature for several reasons. First, researchers can plan new studies to address these concerns.51 Second, concepts about the robustness of the evidence can be combatted. This is particularly true for ambulation, which is now ubiquitous as a preventive measure for venous thromboembolism despite a lack of evidence. Third, clinical practice might change, in particular using the concepts of implementation or de-implementation science.52,53 Although we used a study protocol, it was not registered with PROSPERO (https://www.crd.york.ac.uk/prospero/).
Conclusion
Our systematic review failed to find high-quality evidence to suggest that ambulation alone is an appropriate or effective prophylaxis for venous thromboembolism. Although some studies suggest that ambulation may reduce venous thromboembolism events among patients admitted to hospital, we could not draw conclusions about how early, how much, how vigorous or how often ambulation should occur to reduce events effectively. In the context of substantial evidence for pharmacologic prophylaxis to prevent venous thromboembolism, ambulation should not be considered an adequate prophylaxis, nor should ambulation be a reason to discontinue pharmacologic prophylaxis during hospital admission. Our findings point to an important function of systematic reviews, which is to evaluate existing evidence. We rigorously evaluated data from studies over a 69-year span and can conclude that research is needed to assess prescribed therapies for ambulation and determine whether any are effective in preventing venous thromboembolism events.
Footnotes
Competing interests: Elliott Haut, Michael Streiff, Brandyn Lau and Dauryne Shaffer are supported by a grant from the Agency for Health Research and Quality (R18HS027415). Brandyn Lau, Michael Streiff and Elliott Haut are supported by a grant from the Agency for Health Research and Quality (1R01HS024547) entitled “Individualized Performance Feedback on Venous Thromboembolism Prevention Practice,” a contract from the Patient-Centered Outcomes Research Institute (PCORI) entitled “Preventing Venous Thromboembolism (VTE): Engaging Patients to Reduce Preventable Harm from Missed/Refused Doses of VTE Prophylaxis,” a contract CE-12-11-4489 “Preventing Venous Thromboembolism: Empowering Patients and Enabling Patient-Centered Care via Health Information Technology” from PCORI, and a grant from the National Institutes of Health/ National Heart, Lung, and Blood Institute (R21HL129028) entitled “Analysis of the Impact of Missed Doses of Venous Thromboembolism Prophylaxis.” Brandyn Lau is supported by the Institute for Excellence in Education Berkheimer Faculty Education Scholar Grant and a contract (AD-1306-03980) from the PCORI entitled “Patient Centered Approaches to Collect Sexual Orientation/Gender Identity Information in the Emergency Department.” Deborah Hobson has given expert witness testimony in various medical malpractice cases. Michael Streiff has received research funding from Boehringer-Ingelheim, Janssen, Portola and Roche, consulted for Bayer, CSL Behring, Daiichi-Sankyo, Janssen and Pfizer and has given expert witness testimony in various medical malpractice cases. Elliott Haut is a paid consultant and speaker for the “Preventing Avoidable Venous Thromboembolism — Every Patient, Every Time” VHA/Vizient IMPERATIV Advantage Performance Improvement Collaborative. Elliott Haut receives royalties from Lippincott, Williams, Wilkins for a book — “Avoiding Common ICU Errors.” Elliott Haut is a paid consultant and speaker for the Illinois Surgical Quality Improvement Collaborative “ISQIC.” Elliott Haut was the paid author of a paper commissioned by the National Academies of Medicine, which was used to support the report titled “A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury.” No other competing interests were declared.
This article has been peer reviewed.
Contributors: Brandyn Lau takes responsibility for the content of the manuscript, including the data and analysis. Brandyn Lau and Patrick Murphy contributed equally to the conception and design, search strategy development, acquisition of data and synthesis, drafting of the manuscript and approval of the final version of the manuscript. Patrick Murphy and Anthony Nastasi screened for relevant articles and scored the quality of included studies. Stella Seal helped develop the search strategy and both Stella Seal and Anthony Nastasi contributed to manuscript revisions and approval of the final version of the manuscript. Peggy Kraus, Deborah Hobson, Dauryne Shaffer, Christine Holzmueller, Jonahthan Aboagye, Michael Streiff and Elliott Haut contributed to conception of study and interpretation of data, revisions of the manuscript and approval of the final version of the manuscript. Elliott Haut provided supervision of the study. Brandyn Lau and Patrick Murphy contributed equally and should be credited as co–first authors. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: No data will be made available beyond the search strategy, which is described in the appendix.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/4/E832/suppl/DC1.
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.