


Article Figures & Tables
Figures
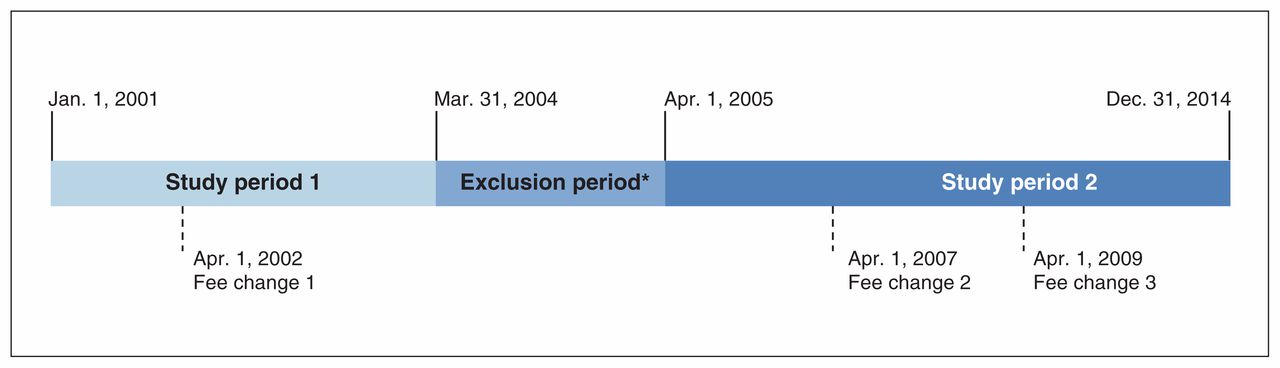
- Figure 1:
Division of the entire study period for analysis purposes. Fee change 1 = introduction of weekly billing code for patients receiving peritoneal dialysis at $32.16. Fee change 2 = increase in weekly billing code for patients receiving peritoneal dialysis from $49.15 to $70.94. Fee change 3 = introduction of weekly billing code for all dialysis modalities at $135. Note that, during the exclusion period, the weekly billing code for patients receiving peritoneal dialysis was increased from $32.16 to $49.15, but we did not analyze this increase owing to the simultaneous expansion of the salaried program. *Patients who started dialysis during this period were excluded.
- Figure 2:
Flow diagram showing participant selection.
- Figure 3:
Proportion of patients starting long-term dialysis who were receiving peritoneal dialysis at 90 days in each month. For illustrative purposes, separate dashed regression lines for the fee-for-service and salaried groups before and after each fee change are displayed on top of the raw data.


Tables
- Table 1:
Characteristics of patients in the fee-for-service and salaried groups during study period 1 (Jan. 1, 2001–Mar. 31, 2004)*
Characteristic Fee-for-service, no. (%) of patients† Salaried, no. (%) of patients† Before fee change 1
n = 197After fee change 1
n = 325Before fee change 1
n = 124After fee change 1
n = 233No. of months 15 24 15 24 Age, yr, mean ± SD‡ 62.6 ± 15.9 64.6 ± 15.7 62.7 ± 15.8 59.5 ± 16.1 Female sex 88 (44.7) 154 (47.4) 51 (41.1) 98 (42.1) Income quintile§ 1 (lowest) 53 (26.9) 72 (22.2) 34 (27.4) 64 (27.5) 2 36 (18.3) 73 (22.5) 27 (21.8) 41 (17.6) 3 33 (16.8) 60 (18.5) 17 (13.7) 49 (21.0) 4 30 (15.2) 46 (14.2) 25 (20.2) 38 (16.3) 5 (highest) 38 (19.3) 54 (16.6) 14 (11.3) 28 (12.0) Unknown¶ 7 (3.6) 20 (6.2) 7 (5.6) 13 (5.6) Comorbidities Alcohol use disorder 14 (7.1) 15 (4.6) 3 (2.4) 14 (6.0) Cancer, nonmetastatic 14 (7.1) 16 (4.9) 5 (4.0) 11 (4.7) Chronic heart failure‡ 79 (40.1) 148 (45.5) 40 (32.3) 82 (35.2) Chronic pulmonary disease‡ 45 (22.8) 113 (34.8)** 37 (29.8) 62 (26.6) Dementia 4 (2.0) 10 (3.1) 4 (3.2) 7 (3.0) Diabetes 115 (58.4) 183 (56.3) 74 (59.7) 130 (55.8) Myocardial infarction 15 (7.6) 31 (9.5) 10 (8.1) 21 (9.0) Peripheral vascular disease 21 (10.7) 38 (11.7) 6 (4.8) 19 (8.2) Stroke/transient ischemic attack 36 (18.3) 71 (21.8) 24 (19.4) 40 (17.2) Dialysis initiation as inpatient 62 (31.5) 88 (27.1) 39 (31.4) 64 (27.5) Distance between patient postal code and nearest hemodialysis facility, km‡†† < 50 166 (84.3) 290 (89.2) 102 (82.3) 192 (82.4) 50–150 31 (15.7) 33 (10.2) 17 (13.7) 29 (12.4) > 150 0 (0.0) 2 (0.6) 5 (4.0) 12 (5.2) Distance between patient postal code and nearest peritoneal dialysis training centre, km‡†† ** < 50 134 (68.0) 249 (76.6) 80 (64.5) 138 (59.2) 50–150 45 (22.8) 64 (19.7) 18 (14.5) 41 (17.6) > 150 18 (9.1) 12 (3.7) 26 (21.0) 54 (23.2) Note: SD = standard deviation.
↵* All covariates defined based on the date of dialysis initiation. χ2 test was used for categorical variables (Fisher exact test when ≥ 20% of cells had an expected value < 5), and 2-sided 2-sample t test for continuous variables.
↵† Except where noted otherwise.
↵‡ Significant at p < 0.05 for difference between fee-for-service and salaried groups after policy change.
↵§ Estimated with the use of the postal code.
↵¶ These patients had postal codes without neighbourhood income data available.
↵** Significant at p < 0.05 for within-group difference before and after fee change.
↵†† Significant at p < 0.05 for difference between fee-for-service and salaried groups before policy change.
- Table 2:
Characteristics of patients in the fee-for-service and salaried groups during study period 2 (Apr. 1, 2005–Dec. 31, 2014)*
Characteristic Fee-for-service, no. (%) of patients† Salaried, no. (%) of patients† Before fee change 2
n = 316Between fee changes 2 and 3
n = 335After fee change 3
n = 1065Before fee change 2
n = 279Between fee changes 2 and 3
n = 236After fee change 3
n = 889No. of months 24 24 69 24 24 69 Age, yr, mean ± SD‡ 64.1 ± 15.5 62.91 ± 15.7 63.4 ± 14.6 63.1 ± 15.1 63.2 ± 14.1 61.3 ± 15.6 Female sex 132 (41.8) 116 (34.6) 424 (39.8) 111 (39.8) 84 (35.6) 333 (37.5) Income quintile§ ¶ 1 (lowest) 85 (26.9) 87 (26.0) 300 (28.2) 80 (28.7) 56 (23.7) 238 (26.8) 2 73 (23.1) 78 (23.3) 235 (22.1) 60 (21.5) 57 (24.2) 208 (23.4) 3 62 (19.6) 66 (19.7) 187 (17.6) 41 (14.7) 42 (17.8) 153 (17.2) 4 53 (16.8) 60 (17.9) 154 (14.5) 53 (19.0) 41 (17.4) 133 (15.0) 5 (highest) 43 (13.6) 42 (12.5) 135 (12.7) 45 (16.1) 36 (15.2) 124 (13.9) Unknown** 0 (0.0) 2 (0.6) 54 (5.1) 0 (0.0) 4 (1.7) 33 (3.7) Comorbidities Alcohol use disorder 19 (6.0) 22 (6.6) 69 (6.5) 113 (40.5) 21 (8.9) 68 (7.6) Cancer, nonmetastatic 14 (4.4) 15 (4.5) 63 (5.9) 11 (3.9) 16 (6.8) 65 (7.3) Chronic heart failure†† 150 (47.5) 147 (43.9) 447 (42.0) 100 (35.8) 93 (39.4) 351 (39.5) Chronic pulmonary disease 101 (32.0) 105 (31.3) 328 (30.8) 85 (30.5) 96 (40.7) 265 (29.8) Dementia 14 (4.4) 15 (4.5) 43 (4.0) 6 (2.2) 8 (3.4) 38 (4.3) Diabetes 185 (58.5) 201 (60.0) 760 (71.4)¶ 151 (54.1) 139 (58.9) 565 (63.6)¶ Myocardial infarction 42 (13.3) 53 (15.8) 167 (15.7) 33 (11.8) 46 (19.5) 140 (15.7) Peripheral vascular disease 26 (8.2) 34 (10.1) 108 (10.1) 24 (8.6) 28 (11.9) 105 (11.8) Stroke/transient ischemic attack 69 (21.8) 65 (19.4) 264 (24.8) 55 (19.7) 52 (22.0) 211 (23.7) Dialysis initiation as inpatient‡†† 126 (39.9) 130 (38.8) 440 (41.3) 89 (31.9) 81 (34.3) 320 (36.0) Distance between patient postal code and nearest hemodialysis facility, km‡ < 50 286 (90.5) 299 (89.2) 957 (89.9) 239 (85.7) 209 (88.6) 776 (87.3) 50–150 28 (8.9) 29 (8.7) 89 (8.4) 37 (13.3) 23 (9.7) 102 (11.5) > 150 2 (0.6) 7 (2.1) 19 (1.8) 3 (1.1) 4 (1.7) 11 (1.2) Distance between patient postal code and nearest peritoneal dialysis training centre, km‡††‡‡ ¶ < 50 229 (72.5) 216 (64.5) 790 (74.2) 199 (71.3) 164 (69.5) 645 (72.6) 50–150 66 (20.9) 84 (25.1) 193 (18.1) 34 (12.2) 35 (14.8) 99 (11.1) > 150 21 (6.6) 35 (10.4) 82 (7.7) 46 (16.5) 37 (15.7) 145 (16.3) Note: SD = standard deviation.
↵* All covariates defined based on the date of dialysis initiation. χ2 test used for categorical variables (Fisher exact test when ≥ 20% of the cells had an expected value < 5); for continuous variables, analysis of variance when comparing time intervals within group, and 2-sided 2-sample t test when comparing between groups.
↵† Except where noted otherwise.
↵‡ Significant at p < 0.05 for difference between fee-for-service and salaried groups after policy change 2.
↵§ Estimated with the use of the postal code.
↵¶ Significant at p < 0.05 for within-group difference between the 3 time periods.
↵** These patients had postal codes without neighbourhood income data available.
↵†† Significant at p < 0.05 for difference between fee-for-service and salaried groups before policy change 1.
↵‡‡ Significant at p < 0.05 for difference between fee-for-service and salaried groups in the period between policy changes 1 and 2.
- Table 3:
Results of individual patient-level analysis of peritoneal dialysis use 90 days after initiation of long-term dialysis before and after fee changes*
Model† OR Differences-in-differences estimator (95% CI)‡ Fee-for-service post–pre Salaried post–pre Fee change 1 (Apr. 1, 2002) Unadjusted 0.81 1.12 0.72 (0.35–1.48) Adjusted§ 0.83 0.94 0.89 (0.44–1.81) Fee change 2 (Apr. 1, 2007) Unadjusted 1.10 0.88 1.24 (0.86–1.80) Adjusted§ 1.03 0.89 1.15 (0.73–1.83) Fee change 3 (Apr. 1, 2009) Unadjusted 1.17 0.90 1.31 (0.87–1.80) Adjusted§ 1.31 0.87 1.52 (0.96–2.40) Note: CI = confidence interval, OR = odds ratio.
↵* The same subset of data served for the periods after fee change 2 and before fee change 3.
↵† Fee change 1: weekly fee-for-service remuneration for peritoneal dialysis introduced at $32.16; fee change 2: weekly fee-for-service remuneration for peritoneal dialysis increased from $49.15 to $70.94; fee change 3: weekly fee-for-service remuneration for all patients receiving dialysis $135.
↵‡ The differences-in-differences estimator is the odds ratio for peritoneal dialysis use in the fee-for-service group after versus before a fee change, divided by the odds ratio for peritoneal dialysis use in the salaried group after versus before a fee change.
↵§ Adjusted model controlled for patient-level covariates shown in Tables 1 and 2.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.