


Article Figures & Tables
Figures
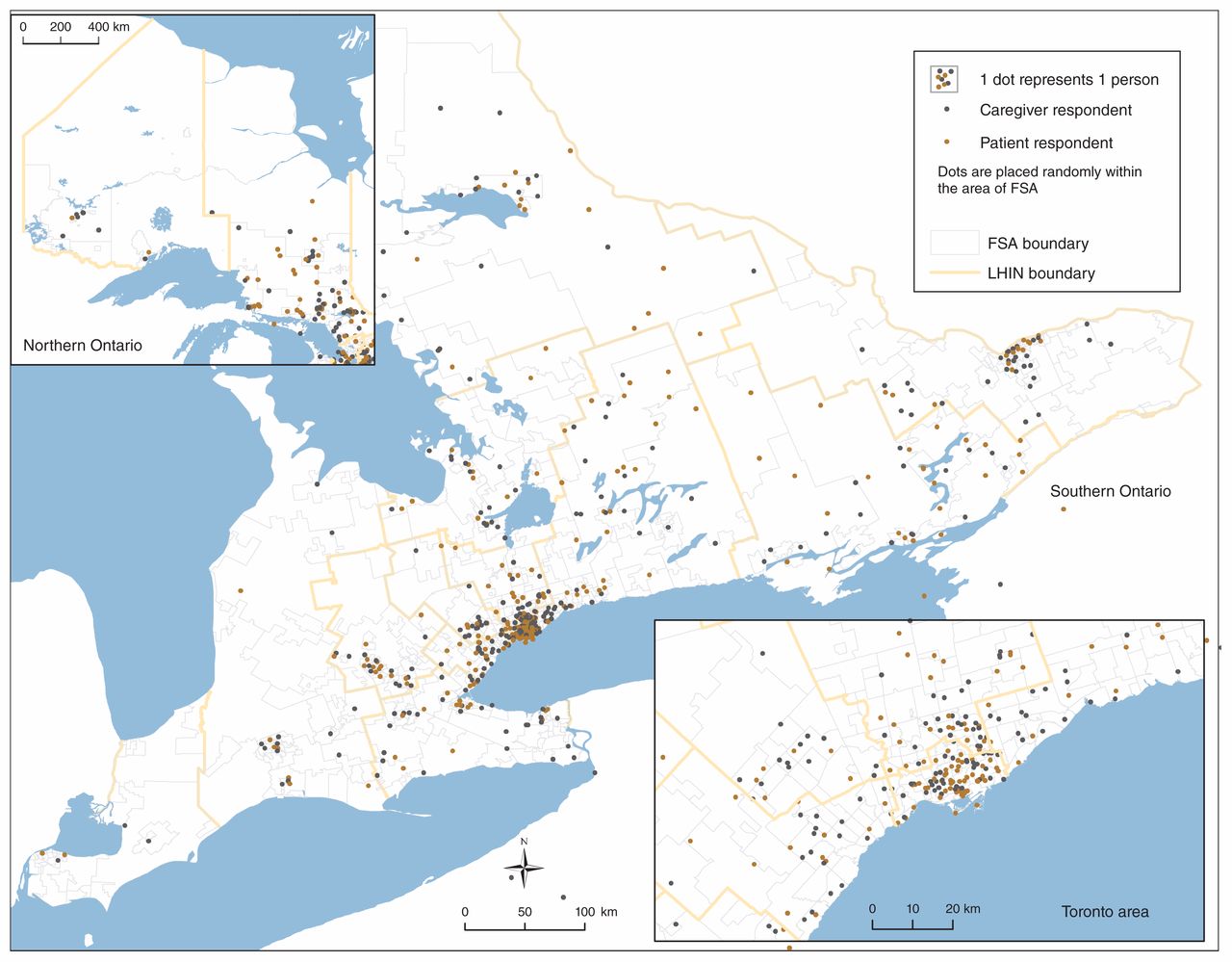
- Figure 1:
Geographic distribution of patients and caregivers who responded to the focal prompt online and provided the first 3 digits of their postal code. Caregivers reported postal codes of the person(s) they were caring for. Note: FSA = forward sortation area, LHIN = Local Health Integration Network.
Tables
- Table 1:
Facilitated group sessions regarding the transition from hospital to home conducted across Ontario
Organization Geographic location Facilitation No. of attendees Country Roads Community Health Centre Portland Facilitated by member of the study’s community advisory group 8 Waterloo Wellington LHIN Patient and Family Advisory Committee Waterloo Facilitated by Health Quality Ontario staff 20 North East LHIN Patient and Family Advisory Committee North Bay Facilitated by Health Quality Ontario staff through Ontario Telemedicine Network 16 Ottawa Cancer Foundation Ottawa Facilitated by local member 5 One More Thing Online (Facebook group) Facilitated by Health Quality Ontario staff 6 Powerhouse Project St. Catharine’s Facilitated by local member 5 St. Michael’s Hospital Patient and Family Advisory Committee Toronto Cofacilitated by hospital staff member and study team member (T.K.) 5 Champlain LHIN Ottawa Facilitated by member of Health Quality Ontario’s Patient, Family and Public Advisors Council 6 Note: LHIN = Local Health Integration Network.
Characteristic No. (%) of participants
n = 665Role* Patient 263 (39.5) Caregiver 352 (52.9) Both 50 (7.5) Patient age (n = 608) ≤ 5 9 (1.5) 6–18 23 (3.8) 19–25 15 (2.5) 26–49 100 (16.4) 50–64 139 (22.9) 65–79 185 (30.4) ≥ 80 137 (22.5) Patient gender (n = 607) Female 357 (58.8) Male 244 (40.2) Other† 6 (1.0) Discharge destination‡ Apartment, house, other place of residence 635 (85.8) Nursing or long-term care home 30 (5.8) Short-term rehabilitation facility, chronic care hospital or “other” 54 (8.0) Other patient characteristics (n = 591) Lives in community that is parallel to or north of Sudbury 61 (10.3) Lives in community with ≤ 30 000 residents 149 (25.2) Would take more than 60 min by car to get to hospital where they were last admitted 83 (14.0) Admitted to hospital more than once in previous year 202 (34.2) Does not have family doctor or nurse practitioner to attend to regular medical needs 31 (5.2) Does not have family or friends who can help when needed 33 (5.6) Lives alone 148 (25.0) Sometimes has difficulty making ends meet at end of month 79 (13.4) Does not have college diploma or university degree 172 (29.1) Came to Canada as immigrant within previous 10 yr 11 (1.9) Is most comfortable speaking language other than English with health care provider 46 (7.8) Identifies as member of LGBTQ2S community 16 (2.7) Has physical, sensory or developmental disability 126 (21.3) Admitted to hospital because of mental health condition 23 (3.9) Has dementia 55 (9.3) ↵* Participants could respond as a patient or caregiver or both. Caregiver participants reported the characteristics of the person they were caring for.
↵† Some respondents reported “other” because they were responding based on the experiences of more than 1 person (e.g., 2 different patients).
↵‡ Caregivers who were also patients responded with more than 1 location to indicate the discharge location for themselves and the patient, if they were different.
- Table 3:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: home and community care supports
Unique concept Representative quote* Home care support being in place when arriving home from hospital After moving home, it took over 3 weeks before we were linked to any home support services. (Female patient, age 26–49)
My father received home care after a week, not 24 hours, as indicated by hospital discharge staff. (Caregiver of male patient, age 50–64)Consistency of home care staff No consistency of care … too many different PSWs; at one point, my mother (with dementia) had 8 different PSWs in 1 week. (Caregiver of female patient, age ≥ 80)
My mother didn’t have enough home care support that was consistent; she had dementia, and she had 14 different workers in 7 days. (Caregiver of female patient, age ≥ 80)Reliability of home care staff Several days after [my husband came] home, case workers started to arrive to assess my husband to determine what I will be needing for home care help. Finally got some help coming to [the] house but not enough hours … as well as numerous no-shows as well as no phone calls to say they are not coming. Just because my husband cannot talk does not mean that his caregiver cannot talk to him. (Caregiver of male patient, age 65–79)
Three times a PSW never showed up to help, and no call was sent to let us know they could not make it. (Caregiver of male patient, age 50–64)Sufficiency of publicly funded home care We had to offset home care with private and family support. (Caregiver of male patient, age ≥ 80)
Limited hours offered by CCAC to support a failing 90-year-old woman in her own apartment. (Caregiver of female patient, age ≥ 80)
After leaving the hospital, my loved one did not have enough care for both morning (wake/bathe/dress) and evening (dinner preparation, clean-up, undress/hygiene/bedclothes) routine. (Caregiver of female patient, age ≥ 80)Having to advocate to get enough home care Had little to no help from CCAC coordinators. Had to fight to get help. (Female patient, age 50–64)
Patients who cannot express themselves well [because of] cognitive or other barriers are roughly treated, and, if there is no advocate, it doesn’t get addressed. (Caregiver of female patient, age 65–79)
It took a lot of work to access the home care services my loved one required and multiple phone calls. (Caregiver of female patient, age ≥ 80)Consistent coordination and level of home care between communities Home care is based on geography. When my relative moved from home to respite care back to her apartment, her care coordinator kept changing. (Caregiver of female patient, age ≥ 80)
There was a gap with CCAC because there were 2 LHINs involved, but once the communication was done, we were contacted. (Caregiver)Consideration of home safety and accessibility during discharge planning There was no consideration whether the home environment was safe to go back to. It wasn’t, but the hospital didn’t care. They said it wasn’t their problem. (Caregiver of male patient, age 65–79)
When I took my brother home, his apartment was not accessible, and I had to make all the necessary changes to help. (Caregiver of male patient, age 26–49)Medically necessary equipment being in place at home when discharged I was not given enough time to arrange how to get my necessary equipment. (Female patient, age 50–64)
CCAC did not have the equipment ready for us when we arrived home. It took 2 days to receive a crucial piece of equipment. (Caregiver of female patient, age ≥ 80)Cost of medically necessary equipment All the needed equipment — canes, walkers, raised toilet seats and bath seats — were bought by the patient’s family. (Caregiver of male patient, age 65–79)
Beds, support equipment free for 28 days. Is it expected that a person is back to normal in 28 days???? The [Assistive Devices Program] does not cover all the equipment. (Caregiver of female patient, age ≥ 80)Availability of community mental health supports Mental health support was not considered or offered. (Caregiver of male patient, age 6–18)
A suicidal child was discharged home; connection was made with community agency, but 1-year wait time for intensive therapy. (Caregiver)Availability of community palliative care supports Lack of community resources for patient. (Caregiver of person age ≥ 80)
Palliative care doc was accessible and responsive. He came late at night, explained everything. He answered texts directly and quickly. (Caregiver of female patient, age 50–64)Timeliness of publicly funded community-based physiotherapy, occupational therapy and other rehabilitation supports Community therapy services were only available on a fee-for-service basis while waiting for 10 weeks for an OHIP-funded program. (Caregiver of male patient, age 19–25)
Six weeks after my hospital discharge, I still had to wait 3 weeks for CCAC, [occupational therapy] and [physiotherapy]. (Female patient, age 65–79)Sufficiency of publicly funded community-based physiotherapy, occupational therapy and other rehabilitation supports [Physiotherapy] only once per week is not enough for someone who could perhaps learn to be mobile and more self-sufficient. Again, we are lucky to afford our own support, but this shouldn’t be necessary. (Caregiver of person age ≥ 80)
[The] only [rehabilitation] was five 1-hour visits paid for by OHIP in second month after surgery. (Female patient, age 65–79)Availability of support services such as housecleaning, laundry and meals People who need more supportive care are given restricted [care] — only bathing or extremely minor assistance. Of no real help to keep people housed independently; their home is left unclean, and no help with food. I needed someone to help with some cleaning. (Caregiver of female patient, age 65–79) Arranging support services such as housecleaning, laundry, and meals The need to figure out where to find support services for services beyond what CCAC would provide [such as] housecleaning, laundry for someone with very limited income. (Caregiver of male patient, age 65–79)
Community services were not in place, and [patients are expected to organize] support such as CCAC, Wheel-Trans. (Facilitated group participant)Reliance on family and friends to provide care after discharge No one is available to get my mom to bed at night, so we have to do it. We go from 6:30 to 10 or 11 at night and get up for work at 5:30 am. (Caregiver of female patient, age 65–79)
After leaving hospital, my family member didn’t have enough home care support to help him bathe and dress, so my spouse had to take time off work to assist his father. (Caregiver of male patient, age ≥ 80)Living alone without family and friend support I live alone and had no support with meal preparation. (Facilitated group participant)
Great concern for people sent home without family to advocate for and help them. (Caregiver of female patient, age ≥ 80)
I lived alone and was scared to be by myself. (Female patient, age 26–49)Assumptions about family and friend support during discharge planning Disheartening. It is unfair to assume family members could just drop everything to be home with their loved ones, especially after long, unexpected illness. (Caregiver of female patient, age ≥ 80)
No questions about home environment — it seemed to be assumed I’d be there 24/7. (I was). (Caregiver of male patient, age 65–79)Respite for caregivers My dad and mom moved into my sister’s house as qualified help was not available on a consistent basis (not even private care). My sister received daily calls of no care available. In 3 months, she has received respite twice so she could buy groceries. (Caregiver of person age ≥ 80)
Respite care has been meagre. It’s a struggle to get 1 day away from the house to be able to travel out of town for shopping, business. (Caregiver of female patient, age ≥ 80)Note: CCAC = Community Care Access Centre, LHIN = Local Health Integration Network, OHIP = Ontario Health Insurance Plan, PSW = personal support worker.
↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
- Table 4:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: medical follow-up after discharge
Unique concept Representative quote* Timely follow-up with family doctor, nurse practitioner or specialist My family doctor, who is a member of [primary care organization], called to arrange a follow-up appointment. (Female patient, age 50–64)
My family doctor knew my daughter was admitted to hospital because I phoned to let her know. I knew that, if we ran into trouble after discharge, our doctor would fit us in to be seen. (Caregiver of female patient, age ≤ 5)
Told to call [the doctor’s] office (which was stated on a form they gave me) in 6 weeks. When I called, the nurse laughed and said [the doctor] hadn’t seen patients that he had operated on for more than 6 months prior to my operation. I kept calling, and it took over a year to see him. (Female patient, age 65–79)Having a trusted family physician No attempt to connect me with a family physician was made by [hospital]. (Male patient, age 65–79)
I had a trusted family doctor that I could consult if I was uncertain about anything. (Female patient, age 50–64)Having specialist follow-up arranged or being able to arrange it Discharge summary listed 2 critical follow-ups needed within 1 week: cardiology and nephrology clinics — NEITHER appointment was made when we left hospital. (Female patient, age 50–64)
Clear, concise written instructions for follow-up appointments with various doctors were given, so that was a handy guide. (Female patient, age 65–79)Family physician receives complete and timely information about hospital admission I wish that my primary care physician had received notification about my [hospital admission]. When I phoned about constipation issues and the bed sore, they had no idea what had happened or care that had been provided in the hospital and would have liked to have been more proactive on these issues. (Female patient, age 26–49)
Family doctor received nothing from hospital to allow a seamless transition home. (Caregiver of female patient, age 65–79)Information transfer between facilities Lack of transitional support for journey from home to hospital to retirement home which was a bridge to long-term care. Information transfer was lacking at each stage, so needs were not able to be met initially at each stage. A case manager seemed to be lacking. (Female patient, age 50–64)
Detailed notes and test results were sent to the [rehabilitation] hospital. (Caregiver of female patient, age ≥ 80)Challenges getting to and from appointments once discharged Routine visits to clinic were very difficult post stroke but were not offered through telemedicine. (Caregiver of female patient, age ≥ 80)
Having to follow up with a doctor whose office was out of town and I do not drive. (Female patient, age 26–49)
The hospital parking for follow-up was poor. The garage with elevators and easy access is reserved for staff. It’s not just the cost of parking — it’s also the ease of use. (Female patient, age 65–79)Having a doctor who does home visits Family doc doesn’t make house calls, so totally lost contact with a doctor. How can a person in bed with discomfort in a wheelchair get an assessment from a doctor? Totally a huge logistical challenge and exhausting and painful for patient to use wheelchair taxi to go to physician office. (Caregiver of person age ≥ 80) ↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
- Table 5:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: discharge process
Unique concept Representative quote* Being discharged too early None of us felt [the patient] was ready to leave the hospital but felt he was being pushed out to free up a bed. (Caregiver of male patient, age 65–79)
Discharged too early. I felt I hadn’t healed and was afraid of reinjuring. (Male patient, age 65–79)
Reason for mental health crisis had not been resolved; although the person was no longer in a suicidal state, they still had suicidal ideation. (Caregiver of male patient, age 50–64)Discharge being delayed Long wait to be discharged. (Caregiver)
On the discharge day (Saturday), we waited several hours for the doctor to sign the discharge papers. By the time she did, the pharmacy was closed, so they had to give us enough for 24 hours, and we had to make another trip (20 minutes each way) the next day to fill the prescription. (Caregiver of female patient, age ≥ 80)Discharge process being rushed Felt a little rushed to leave room as someone was waiting for bed, but staff made sure I understood my discharge papers. (Female patient, age 50–64)
I had almost no preparation time to leave, it was, like, “Get out of bed, you’re going home.” (Female patient, age 19–25)
Rushed process, nurse run ragged and [information] passed on in 3 minutes. (Facilitated group participant)Receiving clear and consistent communication about health status in preparation for going home I was nervous as they still didn’t know what [had] caused the horrible leg infection [the patient] had. (Caregiver of male patient, age 65–79)
The doctors were not honest about [the patient’s] prognosis — they [glossed] over it, and the patient did not fully understand what was happening. (Caregiver of female patient, age 65–79)Being involved in discharge planning Discharge planning was well done. My mother was involved in her discharge planning, as were her caregivers. (Caregiver of female patient, age ≥ 80)
Family/caregiver were not involved in [patient’s] care plan or discharge plan, although [they were] expected to [provide] support outside hospital and provide housing during crisis. (Caregiver of male patient, age 50–64)Having short notice of discharge time I was notified that same day that my spouse was being discharged and had to arrange to leave work and pick him up. (Caregiver of male patient, age 65–79)
No warning was given that [the patient] was being discharged; one day it was a week away, the next day it changed to that day. (Caregiver of female patient, age ≥ 80)Seeing the doctor at time of discharge Did not see the doctor at time of discharge, [which left] many, many unknowns and [added] to fear. (Female patient, age 26–49)
None of the doctors took the time to tell me anything on discharge. The only doctor who did explain anything was not present the day of discharge. He had explained a further test I needed before discharge. I never got the test. (Male patient, age 50–64)Having challenges with transportation home The person I cared for was unable to get into the car and [couldn’t] afford to transfer back home in an ambulance. (Caregiver of male patient, age ≥ 80)
My caregiver wasn’t given a wheelchair to put me in to take me to the car. She had to go down to the lobby to get one and come all the way back up. (Female patient, age 26–49)
I did not have anyone to pick me up or any money to get home. So I had to walk, it was a 5-mile walk. (Female patient, age 50–64)
Had to drive over 200 km to my home. Travel grant doesn’t cover the full cost of an overnight stay. Very exhausting. (Female patient, age 65–79)↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
- Table 6:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: patient education
Unique concept Representative quote* Receiving a written summary of the hospital admission at discharge After getting a hospital discharge, my father received no discharge instructions. (Caregiver of male patient, age 50–64)
We were provided with a detailed discharge summary that included next steps, including follow-ups, medications and signs to look for re: common complications. (Caregiver of male patient, age ≤ 5)Having contact number(s) of someone to call if there is a problem once home There was no one I could call once discharged home for the first time to talk about my symptoms. [Having someone to call] might have sent me to the emergency department earlier, thereby avoiding some undue suffering and optimizing my recovery process. (Female patient, age 50–64)
The doctor made sure I had his contact information so that if I experienced any complications or had concerns I could call him. I did have complications from a procedure he performed, and being able to contact him helped me get readmitted to the hospital and treated faster. (Female patient, age 50–64)Being prepared by hospital staff to manage symptoms and care at home There was a good booklet provided about recovery from cardiac surgery, but it would have been great if the most important details were highlighted or individually detailed. (Female patient, age 50–64)
Paucity of information on how to manage care at home (what to watch for in changes, improvement or deterioration). (Caregiver of male patient, age 50–64)
There was little discussion or instructions with family or long-term care about how to care differently for our loved one upon return to long-term care. (Caregiver of male patient, age ≥ 80)↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
- Table 7:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: medications
Unique concept Representative quote* Medication effects, adverse effects and schedule explained clearly before leaving hospital My medication schedule was explained clearly to me before I left the hospital. (Female patient, age 50–64)
The person I care for did not understand how to take the medications, and no one spent the time explaining. (Caregiver of female patient, age 65–79)No training or support on how to manage complex medication needs once home Managing the [medications is] extremely complex when your loved one is dying — more nursing care is required at home. (Caregiver of female patient, age 50–64)
Having to inject medication for yourself is a big responsibility. (Female patient, age 65–79)Errors about medications on the discharge summary or prescription After one discharge, the medications on the discharge summary were not correct. (Caregiver)
When I left, I was given 2 inhalers, 1 Ventolin and another bronchial powder inhaler. I was a bit surprised but only noticed a month later that they were both addressed to someone else. (Female patient, age 50–64)Having challenges filling a prescription soon after discharge Not able to get discharge prescriptions prior to discharge, no offer to fax to drug store, so by time I got [the patient] home and the analgesic picked up, he was at least 2 hours late in getting [it]! (Caregiver of male patient, age 50–64)
My family member’s medications were not readily available at any pharmacy, and she was sent home on a Saturday evening, so hospital outpatient pharmacy closed. (Caregiver of female patient, age 26–49)No plan for pain management once discharged [Alternative] treatments other than pain [medications] not considered or offered. (Female patient, age 26–49)
Before leaving, a plan for pain management was not adequately addressed, [such as] dosage ranges to accommodate movement at home versus hospital. (Caregiver of female patient, age 6–18)Pain medications prescribed at discharge are too strong or not strong enough My 11-year-old was prescribed morphine for pain. After the first night at home, she had a reaction, so I switched to Children’s Advil and she was fine. Why an opioid for a child? (Caregiver of female patient, age 6–18)
My father has been on prescription pain medications for too long. Need support getting him off these drugs given to him by doctors. (Caregiver of male patient, age 65–79)Having to pay out of pocket for medications and medical supplies Cost of medicine or supplies out of pocket are high. (Female patient, age 26–49)
The staff on the floor “forgot” to return patient’s [prescribed] medications that we brought in to use because they were not on their formulary ... necessitating extra expense/money to replace these. (Caregiver of female patient, age 65–79)↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
- Table 8:
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: kindness and caring of health care team in hospital
Unique concept Representative quote* Hospital staff being kind and caring Once home, I recalled each day the words of encouragement and advice I had received while in the hospital, to my benefit. (Female patient, age 65–79)
Some of the hospital [physiotherapists] were just going through the motions — did not seem to care. (Male patient, age 65–79)
The doctor was amazing. Caring and kind and treated my 92-year-old dad the same way he would treat a 25-year-old. (Caregiver of male patient, age ≥ 80)Health care team in hospital respecting and listening to caregivers The nurses, doctors and specialists [took] our concerns seriously since we know our child best. (Caregiver of male patient, age ≤ 5)
Not enough weight was given to the concerns of the relatives of the patient. They weren’t always included, and the patient, being 85, did not advocate for the support needed. (Caregiver of female patient, age ≥ 80)Doctors and nurses taking the time to listen and answer questions in hospital Doctor took time to answer questions and ensure I was equipped to manage on my own. (Female patient, age 26–49)
The doctor and nurses did not answer all my questions and were not helpful with things like what to expect post surgery. (Caregiver of male patient, age 65–79)Physiotherapy/occupational therapy support being provided in hospital No [physiotherapy, occupational therapy] or discharge planning on the weekends. (Caregiver of male patient, age ≥ 80)
[Physiotherapy] made sure I could safely move enough before I was discharged. (Female patient, age 26–49)Speech, hearing, visual or mobility needs being accommodated in hospital We felt that the staff did not make sure that their message was heard and understood by our parents. [Our parents’] lack of hearing was not recognized by the hospital staff. (Caregiver of female patient, age ≥ 80)
There is no accommodation for someone with aphasia, which is contrary to the [Accessibility for Ontarians with Disabilities Act]. (Caregiver of female patient, age ≥ 80)Dementia being accommodated and managed appropriately in hospital Every new nurse working with [the patient] had no idea he [had dementia] and little notion how to accommodate care. Care plan was inadequate or not read. (Caregiver of male patient, age ≥ 80)
Nurses at hospital had parent in hospital for over 1 week and did not recognize there were cognitive deficits. (Caregiver of female patient, age ≥ 80)Providing culturally safe and appropriate care for Indigenous people in hospital This was a First Nations patient, and there are unique needs to consider with the history of First Nations’ distrust [of] the health care system. (Caregiver) Being able to communicate in preferred language in hospital When I was translating for my dad, the doctor was losing patience with me as I tried to find the right words. (Caregiver of male patient, age 65–79)
No translation services were provided for patient, who did not speak English. (Facilitated group participant)↵* Respondent age and gender are provided when available; caregiver respondents provided the age and gender of the patient they were caring for.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.