


Abstract
Background: Improving the quality of care for patients who return home after a hospital stay is an international priority; however, few jurisdictions have engaged broadly with patients and caregivers to understand what most affects their experience transitioning home. We performed Ontario-wide group concept mapping, beginning with a brainstorming phase, to understand patient and caregiver priorities in the transition.
Methods: We used group concept mapping to engage patients and caregivers who had lived experience transitioning from hospital to home in Ontario in the previous 3 years. We report on the first phase, brainstorming, conducted over 10 weeks beginning Jan. 11, 2018 via an online survey or facilitated group discussion. Participants responded to a single focal prompt: “When leaving the hospital for home, some thing(s) that affected the experience were: ____.” The study team identified recurrent concepts and overarching themes. Patients and caregivers informed the study design, recruitment and data interpretation.
Results: In all, 665 people (263 patients [39.5%], 352 caregivers [52.9%] and 50 people who were both patient and caregiver [7.5%]) participated in brainstorming online, and 71 people participated in 1 of 8 group discussions. Participants identified 6 key areas affecting their experience of transition from hospital to home: home and community care, the discharge process, medical follow-up after discharge, medications, patient and caregiver education, and the kindness and caring of the health care team in hospital. Most notable were challenges with the timeliness, sufficiency, reliability and consistency of publicly funded home care services.
Interpretation: Patients and caregivers from across Ontario noted a range of issues affecting their experience transitioning from hospital to home, particularly the quality and sufficiency of publicly funded home care. Our findings will be used to inform a provincial quality standard on the transition from hospital to home.
Plain language summary:
Transitioning back home after a hospital admission can be a tricky time for patients and their caregivers. Patients have experienced changes in their health and ability to function independently, and, at the same time, are relying on different parts of the health care system to work well together. We wanted to understand what most affected patient and caregiver experience in the transition from hospital to home and use our findings to develop a provincial quality standard that outlines what good care looks like when patients are discharged from hospital to home. We conducted public outreach over 10 weeks beginning Jan. 11, 2018 to recruit patients and caregivers who had a lived experience transitioning from hospital to home in Ontario in the previous 3 years. We asked participants to brainstorm responses to a single question: “When leaving the hospital for home, some thing(s) that affected the experience were: ____.” A total of 665 patients and caregivers responded to the question online, and another 71 via a facilitated group discussion. We analyzed the data for themes and found that patients and caregivers identified 6 key areas affecting their experience transitioning from hospital to home: home and community care, the discharge process, medical follow-up after discharge, medications, patient and caregiver education, and the kindness and caring of the health care team in hospital. The most common challenges were with the timeliness, sufficiency, reliability and consistency of publicly funded home care services. Understanding what matters to patients and caregivers helps us define what good care looks like and how we should focus efforts to improve our health care system.
Improving the transition from hospital to home is an important health care system priority. Much of the research about the transition from hospital focuses on reducing readmissions, partly as a strategy to reduce costs.1 But interventions to reduce readmissions have had mixed success,2,3 and there is debate about whether readmissions can be prevented through better care4,5 or whether readmission is an outcome important to patients.6 Focusing efforts on understanding and improving the patient experience may be a more fruitful approach to improving the quality of transition from hospital to home.
Engaging patients in health care design can improve service delivery and quality of care.7,8 Many organizations are trying to enhance patient engagement in direct care9,10 or have engaged patients to inform organizational-level interventions.
Our provincial quality agency was interested in engaging patients to inform a quality standard on the transition from hospital to home. We performed province-wide group concept mapping to understand patient and caregiver priorities in the transition. We began with province-wide brainstorming that sought to understand what affected the patient and caregiver experience in the transition from hospital to home.
Methods
Setting and context
The research was conducted in partnership between Ontario’s agency for health care quality at the time, Health Quality Ontario (now Ontario Health [Quality Business Unit]), and a team of researchers. Ontario is Canada’s most populous province, with about 14.1 million people in 2017.11 Physician and hospital services are fully insured under the provincial health insurance plan, which covers all permanent residents, but there are recognized gaps in coverage, including gaps in dental care, home and community care, and medications.12 Home and community care services are organized and delivered at the level of the health region (Local Health Integration Network).
Study design and participants
We used group concept mapping methods to engage people with lived experience as a patient or caregiver of a patient transitioning home from hospital. Group concept mapping is a participatory research method ideally suited to gather input from a large number of stakeholders to inform planning and evaluation.13–17 It involves participants in generating ideas, prioritizing emerging concepts and interpreting results (Appendix 1, available at www.cmajopen.ca/content/8/1/E121/suppl/DC1). Group concept mapping has been used to understand patient experience18 and what good care looks like,19,20 with the results informing the development of performance measures. It has also been used to engage patients in clinical quality improvement.21
We report on the first phase of concept mapping — brainstorming — which engages participants in generating ideas relevant to the research question. Research has shown that brainstorming in group concept mapping is highly effective and efficient at identifying outcomes important to patients compared to traditional qualitative methods.22
We engaged people who had lived experience as a patient or caregiver of a patient discharged home after being admitted overnight to an Ontario hospital in the previous 3 years. We defined “home” broadly to include community residences, such as an apartment or house, but also shelters, supportive housing, long-term care, rehabilitation and chronic care facilities. Caregivers could include family members or unpaid friends. Participants self-assessed whether they met the inclusion criteria. On the advice of patients and caregiver advisors, there were no age restrictions for participation.
Recruitment
In keeping with the mandate of Health Quality Ontario, recruitment was intentionally broad and inclusive. However, we also used strategies to reach participants from diverse backgrounds. We recruited participants over 10 weeks beginning Jan. 11, 2018 using the agency’s social media channels and network of partner organizations. We provided pertinent patient, community and health care organizations (e.g., Meals on Wheels, Multiple Sclerosis Society of Canada, Lived Experience & Recovery Network, Ontario Hospital Association, Association of Family Health Teams of Ontario) with materials to promote the survey (Appendix 2, available at www.cmajopen.ca/content/8/1/E121/suppl/DC1) and invited them to host a group discussion.
With the help of a community advisory group (Appendix 3, available at www.cmajopen.ca/content/8/1/E121/suppl/DC1), we undertook targeted outreach to patient groups that we hypothesized a priori as having unique perspectives but suspected were difficult to reach. Target populations included children, long-term care residents, rural residents, those with mental health issues, newcomers, people who did not speak English, people who were homeless or experiencing housing instability, and members of the LGBTQ2S community. Members of community advisory groups supported their community groups to engage in group discussions or online (e.g., by providing language interpretation as needed).
We monitored participant demographic characteristics and intensified recruitment strategies for target populations accordingly. There was no monetary incentive to participate. Health Quality Ontario committed to sharing the results with participants.
Data collection
Participants could engage in brainstorming in 1 of 2 ways: via on online survey hosted on Health Quality Ontario’s webpage or via a facilitated group discussion. In both cases, participants were asked to provide responses to a single focal prompt: “When leaving the hospital for home, some thing(s) that affected the experience were: ____.” Instructions clarified that participants could report both positive and negative experiences, and could provide multiple responses. We tested and refined the focal prompt based on feedback and pilot testing from Health Quality Ontario’s Patient, Family and Public Advisors Council, and Patient Advisors Network. Participants were asked to complete demographic questions after answering the focal prompt online. Online responses were anonymous and were exported into Microsoft Excel for analysis.
Facilitated group discussions were hosted by interested patient, community and health care organizations. We included this participation option to maximize the diversity of respondents and to support participation for people with lower language and electronic literacy. Members of the study team and of Health Quality Ontario produced a facilitation guide (Appendix 4, available at www.cmajopen.ca/content/8/1/E121/suppl/DC1), facilitation slides (Appendix 5, available at www.cmajopen.ca/content/8/1/E121/suppl/DC1) and live webinars to support organizations to host a group session.
All sessions were cofacilitated or guided by a member of the agency’s Patient and Public Partnering team. Sessions lasted 30–60 minutes and were not audio-recorded. The host organization was responsible for documenting responses to the focal prompt and collecting demographic information of participants, and forwarding these to Health Quality Ontario. The agency received group responses without any participant identifiers and entered these manually into Excel.
Data analysis
We analyzed all responses to the focal prompt from the online survey and group discussion together using thematic analysis.23,24 We included responses even if demographic information was incomplete. Eight members of the research team (T.K., D.W., K.O., C.K., K.D., G.M., L.P., P.O.) read and coded the data as follows. First, they individually selected 200 items at random and thematically coded them, keeping and coding items that were responsive to the focal prompt, and eliminating items that were off topic or duplicates. The team members then met and discussed their codes and agreed on a single set of 6 codes that applied to the 200 items. Subsequently, the remaining items were assigned to team members to eliminate items that were not relevant, to apply the initial set of thematic codes and to flag any items that were responsive to the focal question but did not fall into the initial thematic codes. There was overlap in assignment of items to team members to support consistent coding. Discrepancies and uncertainty were resolved via email and face-to-face meetings.
The team reviewed responses from participants whose transition was to a long-term care home, rehabilitation centre or chronic care hospital separately to determine whether additional codes were needed; ultimately, the 6 existing thematic codes were applied to all the items, with no new thematic codes emerging.
Once all items were eliminated or coded, 2 team members each worked with items within a single thematic code. The team members then identified 5–15 statements (concepts) to represent that code. Given that some categories had dozens of items, this required a second round of thematic coding within these large initial groupings. This helped to ensure that key themes within the initial categories were represented in the final statements.
After the second round of thematic coding, the team reviewed the coded items and together developed the final statements. The team tried to have each statement reflect the language used by participants in their responses. The team aimed to identify up to 50 unique statements, a manageable number for use in the sorting and rating phase of concept mapping.13,25 As a final check, the principal investigator (T.K.) re-reviewed all coded items and modified or confirmed the final statements.
We summarized participants’ demographic characteristics using simple proportions.
All analyses were conducted in Excel, which offered sufficient functionality for thematic coding given the relatively short responses to the focal prompt.
Patient engagement
Members of Health Quality Ontario’s Patient, Family and Public Advisors Council identified that improving transition from hospital to home was a priority and were involved in the initial study design. They informed the engagement approach, participant inclusion criteria and brainstorming question.
We formed a community advisory group composed of patients, caregivers, and representatives from selected community and health care organizations to help with targeted engagement (Appendix 3). The community advisory group also informed study design and helped with interpretation of results.
Health Quality Ontario’s Patient Advisors Network — over 500 patients, families and members of the public from across the province — helped to recruit survey participants.
Finally, we reviewed the study design, proposed outreach and preliminary results with the Transitions Between Hospital and Home Quality Standard Advisory Committee. The committee includes people with lived experience as well as clinicians, administrators and policy experts who advise Ontario Health (Quality Business Unit) on the development of the quality standard.
A brief summary of preliminary results from the brainstorming were shared with all participating organizations and posted on the agency website. No individual patient partners met the criteria for study authorship.
Ethics approval
The protocol was reviewed and discussed with the St. Michael’s Hospital Research Ethics Board and deemed not to constitute research under Article 2.5 of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans and to not require informed consent from participants.
Results
In all, 665 people (263 patients [39.5%], 352 caregivers [52.9%] and 50 people who were both patient and caregiver [7.5%]) responded to the focal prompt online, and 71 people participated in 1 of 8 group discussions. An additional 287 people began the online survey but did not respond to the focal prompt.
Group discussions were facilitated in 5 health regions and were organized by Local Health Integration Networks, primary care centres, hospitals and patient advocacy organizations (Table 1). We did not consistently receive demographic information about participants in the facilitated group discussion; self-reported demographic characteristics of participants who responded to the online survey are presented in Table 2. The majority (635 [95.5%]) of online participants reported that the patient was discharged to an apartment, house or other community residence; 30 (4.5%) went to a long-term care home; and 54 (8.1%) went to a rehabilitation facility, chronic care hospital or other destination (numbers total < 665 as some participants specified more than 1 destination if they were responding as both a patient and a caregiver). Participants came from different communities spanning Ontario’s geography (Figure 1).
Facilitated group sessions regarding the transition from hospital to home conducted across Ontario
Self-reported demographic characteristics of online participants
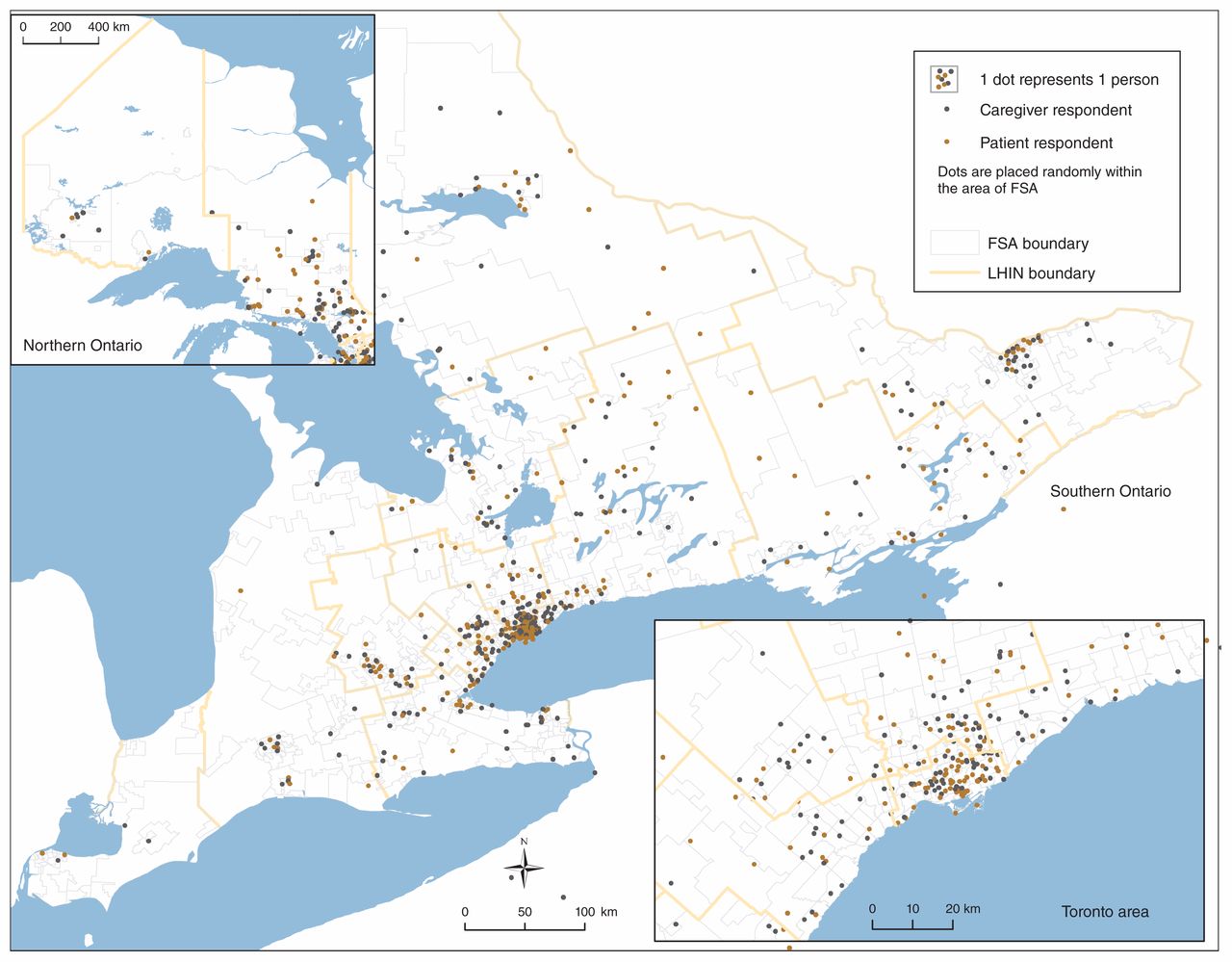
Geographic distribution of patients and caregivers who responded to the focal prompt online and provided the first 3 digits of their postal code. Caregivers reported postal codes of the person(s) they were caring for. Note: FSA = forward sortation area, LHIN = Local Health Integration Network.
Participants collectively submitted 2704 responses to the focal prompt. Most responses (about 85%) described negative experiences. We identified 6 overarching themes — home and community care and supports, medical follow-up after discharge, discharge process, patient education, medications, and kind and caring health care team in hospital — and 52 related statements (concepts). Themes and example quotes were shared with people with lived experience who were on our advisory groups or participated in this or later engagements; themes resonated as reflective of their experience.
Home and community care and supports
The largest number of participant responses were related to home and community care, and most described negative experiences (Table 3). Many participants commented about the poor quality of home care, including the timeliness and sufficiency of services, and the consistency and reliability of home care staff. Many reported that home care was not in place for days or weeks once the patient was home, sometimes contrary to what they had been told in hospital. Home care staff changed frequently and often cancelled with short notice or no notice. Many participants described not having enough care, particularly for bathing and dressing, and some specifically noted that patients and caregivers needed to advocate to get the care they needed. Some mentioned challenges with coordination and staffing when patients moved between 2 Local Health Integration Networks.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: home and community care supports
Participants reported challenges accessing a range of community supports, including outpatient mental health support. Experiences with home palliative care were mixed. Participants expressed that there was often a long wait for publicly funded physiotherapy and rehabilitation supports, and that the publicly funded care eventually provided was insufficient to meet their need. Participants also noted that housecleaning, laundry and other support services were not covered by the home care agency and that arranging these was challenging.
Many patients described the important role their family and friends played in supporting their recovery at home, whereas others described difficulties in living alone after discharge with no family support. Some participants commented on the minimal respite services for caregivers.
Medical follow-up after discharge
Participants reported both positive and negative experiences accessing their family doctor or specialist in a timely way after discharge (Table 4). Some appreciated having a trusted family doctor, whereas others noted they had no family doctor and were not given help to find one. Some participants left hospital with specialist appointments clearly arranged, but others expressed frustration at having to arrange these themselves, in some cases without clear direction. Participants noted whether their family physician or health care staff at their long-term care home or rehabilitation centre had information about the admission. Participants also recounted difficulties getting to follow-up appointments because of challenges with mobility, distance, and related transportation or cost, with some wishing their doctor made house calls.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: medical follow-up after discharge
Discharge process
Several participants described negative experiences related to the timing of discharge (Table 5). Many felt that they or their loved one were discharged too early, before recovery, with some thinking this contributed to a subsequent hospital visit. Some described the discharge process as rushed, in some cases because someone else was waiting for the bed. In contrast, other participants said there were unnecessary delays in the expected discharge due to paperwork.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: discharge process
Experiences relating to communication and shared-decision making were mixed. Some participants described being involved as a patient or caregiver in the discharge process, whereas others, particularly caregivers, discussed being left out of planning although they would be caring for the patient at home.
Participants described not being given enough notice about the discharge time; in some cases, this resulted in logistical difficulties for caregivers. Participants specifically commented on not being able to see the doctor at the time of discharge. Some also expressed challenges with transportation home.
Patient education
There were mixed experiences with receiving a written discharge summary that included instructions (Table 6). Many participants mentioned they were uncertain who to call if there was a problem after discharge, although some were given the number of a doctor or staff member. Some participants noted receiving clear information about self-care and recovery once home, whereas others described not having information on how to care for themselves or use new equipment.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: patient education
Medications
Some participants had medication effects, adverse effects and schedules explained clearly to them before discharge, whereas others did not (Table 7). Several described challenges managing complex new medication regimens at home and not having sufficient instruction or support to do so. Some participants mentioned the high out-of-pocket costs for medication. A few noted difficulty filling their prescription in a timely way after discharge.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: medications
Kind and caring health care team in hospital
Many participants recounted how doctors, nurses and other hospital staff were kind and caring (Table 8). Some described staff as being rude or inattentive. Many noted whether their doctor or nurse took time to listen and answer their questions. A few participants described not having accommodations for people with specific physical needs (e.g., visual or hearing impairment) or not having language or cultural needs met. Many felt that how they were treated in hospital directly affected their recovery at home.
Patient and caregiver views on factors affecting the experience of transitioning from hospital to home: kindness and caring of health care team in hospital
Interpretation
In this patient-oriented study, in which we consulted with a large, diverse group of patients and caregivers across a vast geographic area who had lived experience of transitioning from hospital to home, patients and caregivers highlighted several areas that affected their experience in the transition from hospital to home. The most commonly reported challenges related to home and community care, with many participants reporting that publicly funded home care services were not timely, sufficient, reliable or consistent. Many relied on family, friends, private services or charities to fill the gap. The second most notable theme related to the discharge process, including timing, communication, and involvement of patients and caregivers in the planning process. The largest proportion of positive experiences related to kindness and caring of individual physicians, nurses and hospital staff.
The gaps we found in the availability and quality of home care echo concerns raised in the 2015 final report from Ontario’s Expert Group on Home and Community care.26 In 2017, home care delivery in Ontario underwent substantial reforms, with responsibility transferring from regional agencies to the Local Health Integration Network itself.27 A year after these reforms, patients and caregivers in our study continued to report numerous challenges with home care services. Implementing recommendations from a recent expert panel to ensure a consistent and transparent level of service may address some of these concerns.28
Our findings also underscore the importance of shared decision-making and clear communication during the transition from hospital to home. Patients and their caregivers wanted to be involved in discharge planning, have their questions answered, understand their medications and know how to perform self-care once home. Lack of patient and caregiver involvement in discharge planning is a known gap.29–31 Other studies have shown that patients attribute readmissions to being discharged too early and not having their concerns addressed.32,33 Informational continuity among hospital, patients and families, and outpatient settings is another known challenge34–36 that was echoed in our findings and is the subject of interventions under evaluation. 37 Like us, others have noted how kindness and caring by the care team in hospital can affect the transition from hospital to home.38
Our study highlights the limits of the coverage of Ontario’s public health insurance and how these conflict with patient and caregiver expectations. Policy experts have long noted that Canada has deep public coverage for a narrow basket of services, specifically hospital, diagnostic and physician services.39 Our study revealed challenges even within this narrow basket, including lack of a family doctor and pressure on hospital beds, leading to people feeling pushed out. Bigger challenges related to out-of-pocket costs for medications, equipment, transportation and home support services, such as meal preparation and housecleaning. People noted limited coverage for services such as physiotherapy and home care; some could afford to pay privately for these services, but others could not.
Limitations
Study participants came from varied geographic, medical and social backgrounds, but we had limited success recruiting newcomers and people who did not speak English or French. Our initiative was not designed specifically to understand or address the unique needs of Ontario’s Indigenous communities; Indigenous health experts we spoke with recommended that the Ontario Health (Quality Business Unit) partner with Indigenous communities separately to focus on the impact of transitions in care on Indigenous health.
Group concept mapping methods made it feasible for us to gather open-ended responses from a large number of participants but also meant our responses were not as rich as qualitative data from semistructured interviews or focus groups. However, other research suggests that the brainstorming method identifies a higher proportion of outcomes important to patients compared to qualitative interviews.22 We did not use techniques to limit the same person from responding more than once. However, this limitation had minimal impact on our results, as the survey encouraged participants to provide as many responses to the focal question as desired.
Our recruitment was intentionally broad and inclusive; however, the fact that participants self-selected may have introduced bias into our results. Furthermore, the majority of responses about the transition experience were negative, and it is unclear to what degree this reflects a response bias toward those with more negative experiences. Regardless, these are areas for health system improvement.
Lessons learned from patient engagement
Patient involvement in the research improved the study design, including the focal prompt, study inclusion criteria, target population and recruitment strategies. Patient and community groups enabled us to effectively recruit study participants who represented a broad cross-section of Ontarians, including patients living in rural communities and those traditionally underserved. Discussing our early results with patients helped us validate our findings and interpretation. It was clear throughout the process that patients and caregivers identified improving the transition from hospital to home as an important health system priority.
Conclusion
Our consultation with more than 700 patients and caregivers from diverse communities across the province highlighted 6 key areas affecting their experience of transition from hospital to home: home and community care, the discharge process, medical follow-up after discharge, medications, patient and caregiver education, and the kindness and caring of the health care team in hospital. Most notable were challenges with the timeliness, sufficiency, reliability and consistency of publicly funded home care services. The second phase of our group concept mapping will engage patients and caregivers to prioritize areas for health system improvement. Our work will inform a provincial quality standard on transitions from hospital to home that will be used as a foundation for quality improvement.
Acknowledgements
The authors thank their community advisory group for their guidance on study design, support with participant recruitment and assistance with interpreting the data; Health Quality Ontario’s Patient, Family and Public Advisors Council for their early input on study design and participation in the study; and Health Quality Ontario’s Transitions Between Hospital and Home Quality Standard Advisory Committee for their feedback on study design, recruitment and data interpretation. They thank Health Quality Ontario’s Patient and Public Partnering team and Communications team for their work supporting patient and caregiver outreach, and the senior leadership team for their support through the project and helpful comments on the manuscript.
Footnotes
Competing interests: At the time of writing, David Wells, Carol Kennedy, Gracia Mabaya, Lacey Phillips and Amy Lang were employees of and Tara Kiran was an embedded clinician researcher at Health Quality Ontario. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Tara Kiran conceived the study, and Tara Kiran, David Wells, Amy Lang and Pat O’Campo designed it. Tara Kiran, David Wells and Amy Lang recruited participants and supported data collection. Tara Kiran, David Wells, Karen Okrainec, Carol Kennedy, Kimberly Devotta, Gracia Mabaya, Lacey Phillips and Pat O’Campo analyzed and interpreted the data. Tara Kiran drafted the manuscript. All of the authors revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: Tara Kiran is supported as a Clinician Scientist by the Department of Family and Community Medicine at the University of Toronto and at St. Michael’s Hospital. She is also supported by Ontario Health (Quality Business Unit) and the Canadian Institutes of Health Research as an Embedded Clinician Researcher. She is the Fidani Chair in Improvement and Innovation at the University of Toronto.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/1/E121/suppl/DC1.
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.