


Abstract
Background: Bed rest is prescribed by most maternity health care professionals for high-risk pregnancy complications, but the impact of bed rest at home and in hospital has not been explored. Our aim was to quantify the influence of bed rest on maternal/fetal health outcomes in developed and developing regions.
Methods: We conducted a systematic review and meta-analysis of randomized controlled trials. We conducted a structured search through MEDLINE, Embase, CINAHL, Web of Science and the Cochrane Library through Mar. 7, 2019. Trials comparing standard care to standard care plus bed rest after 20 weeks’ gestation were assessed. Outcomes included infant birth weight, being small for gestational age, gestational age, premature or very premature birth, perinatal death, admission to the neonatal intensive care unit, preterm rupture of membranes, hypertensive disorders of pregnancy, preeclampsia and gestational diabetes mellitus.
Results: We identified 1191 publications, of which 43 were assessed for eligibility. Sixteen publications reporting on 14 unique studies (2608 women, 3328 infants) were included in the analysis. Overall, maternal/newborn outcomes were similar between women on bed rest and those not on bed rest. In subgroup analyses of developed and developing regions, length of gestation was shorter with bed rest (weighted mean difference −0.77 wk, 95% confidence interval [CI] −1.26 to −0.27, I2 = 0%), and the risk of a very premature birth was increased (risk ratio 2.07, 95% CI 1.15 to 3.73, I2 = 0%) in developed countries.
Interpretation: In developed regions, treatment of complicated pregnancies with more than 1 week of bed rest results in worse newborn outcomes. Additional studies are required to determine whether bed rest or hospital admission improves outcomes in developing regions. PROSPERO Trial registration number: CRD42018099237.
Bed rest and activity restriction is prescribed to about 20% of pregnant women with the intent of improving maternal/fetal health outcomes of high-risk pregnancies complicated by preterm labour, intrauterine growth restriction and hypertensive disorders of pregnancy.1–3 Bed rest as a treatment is associated with an economic cost of up to US$7 billion per year in the United States alone (including hospital admission, lost wages and lost domestic productivity). 1,4 Previous meta-analyses focused on multiple or singleton pregnancy suggested there is little evidence to support a policy of routine hospital admission for bed rest.5,6 However, high heterogeneity was highlighted as an issue for several outcomes. Despite the lack of evidence, bed rest continues to be prescribed by up to 95% of clinicians.1,7 This has resulted in an urgent call for additional research to elucidate the potential benefits (or harms) of bed rest for the woman and her fetus by the World Health Organization and the American College of Obstetricians and Gynecologists.7–9
Previous meta-analyses are current to 20175,6,10,11 but do not include all available trials. There appears to be a dichotomy between studies on bed rest conducted in developing countries versus developed countries. Bed rest studies conducted in developing countries may be significantly confounded by hospital admission, which may provide patients with increased access to nutritious food and clean water and increased vigilance by medical personnel; this may have substantially less impact on health outcomes in the developed world. However, the influence of the study location’s developmental status on the impact of bed rest at home and in hospital has not been explored. Therefore, we conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) that contrasted the effect on maternal/fetal health outcomes of bed rest or activity restriction in conjunction with standard care versus standard care alone (no bed rest) in pregnant women at 20 weeks’ gestation or more.
Methods
Eligibility criteria
We used the PICO (population, intervention, comparison, outcome[s]) framework to guide this review (Box 1).
PICO framework
Population: The population of interest was pregnant women.
Intervention: The intervention was standard care (including tocolytics and antihypertensive medications) plus bed rest (including activity restriction, in hospital or at home). Bed rest was defined as a prescribed restriction of activity encompassing the majority of waking hours for 1 week or more.12
Comparison: The eligible comparator was standard care without activity restriction (no bed rest).
Outcomes:
Fetal: birth weight, small at birth (birth weight < 1500 g and < 2500 g) or small for gestational age (< 10th percentile for gestational age and sex), gestational age, premature delivery (< 37 wk), very premature delivery (< 35 wk, < 34 wk or < 32 wk, as defined by the author), perinatal death and admission to the neonatal intensive care unit.
Maternal: preterm rupture of membranes, hypertensive disorders of pregnancy, preeclampsia and gestational diabetes mellitus.
Search strategy and study inclusion
We conducted this systematic review and meta-analysis in accordance with the Cochrane Handbook for Systematic Reviews of Interventions.13 We conducted a structured search through MEDLINE (1946 to Mar. 7, 2019), Embase (1974 to Mar. 7, 2019), CINAHL (1937 to Mar. 7, 2019), Scopus (inception to Mar. 7, 2019), Web of Science (1899 to Mar. 7, 2019) and the Cochrane Library (inception to Mar. 7, 2019). The complete search strategy is given in Appendix 1 (available at www.cmajopen.ca/content/7/3/E435/suppl/DC1). We searched for RCTs investigating the impact of bed rest versus standard care without activity restriction in pregnancy using controlled vocabulary (when available) and text words representing pregnancy/maternal/fetal outcomes or complications combined with terms representing bed rest. We modified the Cochrane RCT filter to exclude the drug therapy floating subheading and to include the term intervention*, and applied it to the searches with the exception of the Cochrane Library.13 Studies were not excluded because of language of publication or publication format (e.g., abstracts only). The structured search was created by L.S. and reviewed by a second librarian with systematic review experience. Records identified by the search strategy were independently assessed in duplicate for inclusion by B.M. or C.C., and M.H.D., with N.G.B. acting as arbitrator in the event of disagreement.
Data extraction
Studies were extracted independently and in duplicate by 2 researchers (B.M. and M.H.D.) using a standardized data collection form including indication for bed rest, duration of bed rest, location of bed rest (e.g., hospital v. home), and any cointerventions used, as well as fetal outcomes of interest (birth weight, being small at birth [birth weight < 1500 g and < 2500 g] or small for gestational age [< 10th percentile for gestational age and sex], gestational age, premature delivery [< 37 wk], very premature delivery [< 35 wk, < 34 wk or < 32 wk, as defined by the author], perinatal death and admission to the neonatal intensive care unit) and maternal outcomes of interest (preterm rupture of membranes, hypertensive disorders of pregnancy, preeclampsia and gestational diabetes mellitus). When multiple publications from the same trial were identified, data were extracted from all available articles.
Quality measures and risk of bias
The risk of bias in RCTs was assessed independently and in duplicate by C.C. and M.H.D. following the Cochrane Handbook for Systematic Reviews of Interventions.13 All studies were screened for potential sources of bias including selection bias, reporting bias, performance bias, detection bias, attrition bias and “other” sources of bias. The risk of bias across studies was rated as “serious” when studies having the greatest influence on the pooled result (assessed by means of weight [percent] given in forest plots) presented “high” risk of bias.14 The quality of the evidence was assessed by C.C. and M.H.D. using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.14 Evidence from RCTs was rated as high quality by default and then downgraded based on prespecified criteria, including study limitations (weight of studies showed serious risk of bias), inconsistency (heterogeneity was high [I2 ≥ 50%] or only 1 study was assessed), indirectness (bed-rest–only interventions and bed rest plus cointerventions were combined for analysis), imprecision (95% confidence interval [CI] crossed the line of no effect and was wide) and publication bias (substantial evidence of small-study effects).
Statistical analysis
We conducted statistical analyses using Review Manager v5.2. (Cochrane Collaboration). For continuous outcomes, we examined mean differences between bed-rest and no–bed-rest groups. For binary outcomes, we calculated risk ratios (RRs). We applied inverse-variance weighting to obtain pooled weighted mean differences (WMDs) and RRs using a random effect model. We performed a sensitivity analysis to evaluate whether the effects were different when examining relations between the different indications for bed rest and maternal/infant outcomes. We conducted the following subgroup analyses, determined a priori: 1) developmental status of the region in the year the study took place based on the World Bank country definition15 and 2) single-versus multiple-gestation pregnancies. We used χ2 tests to estimate heterogeneity between trials. The percent of total variability attributable to heterogeneity (i.e., not due to chance) was expressed as the I2. We explored the source of heterogeneity when intersubgroup heterogeneity was significant (p < 0.05). We estimated missing standard deviations (SDs) for outcomes from reported p values and sample sizes,16 according to procedures in the Cochrane Handbook for Systematic Reviews of Interventions (section 7.7.3.3).13 We used GRADEpro GDT (McMaster University and Evidence Prime) to evaluate and tabulate quality of evidence and strength of recommendations.17
Ethics approval
Ethics approval was not required for this systematic review and meta-analysis.
Results
Study selection
The literature search identified 1191 potentially relevant studies, 43 of which were assessed for eligibility. Sixteen articles from 14 individual RCTs met our inclusion criteria and were included in the review (Figure 1).
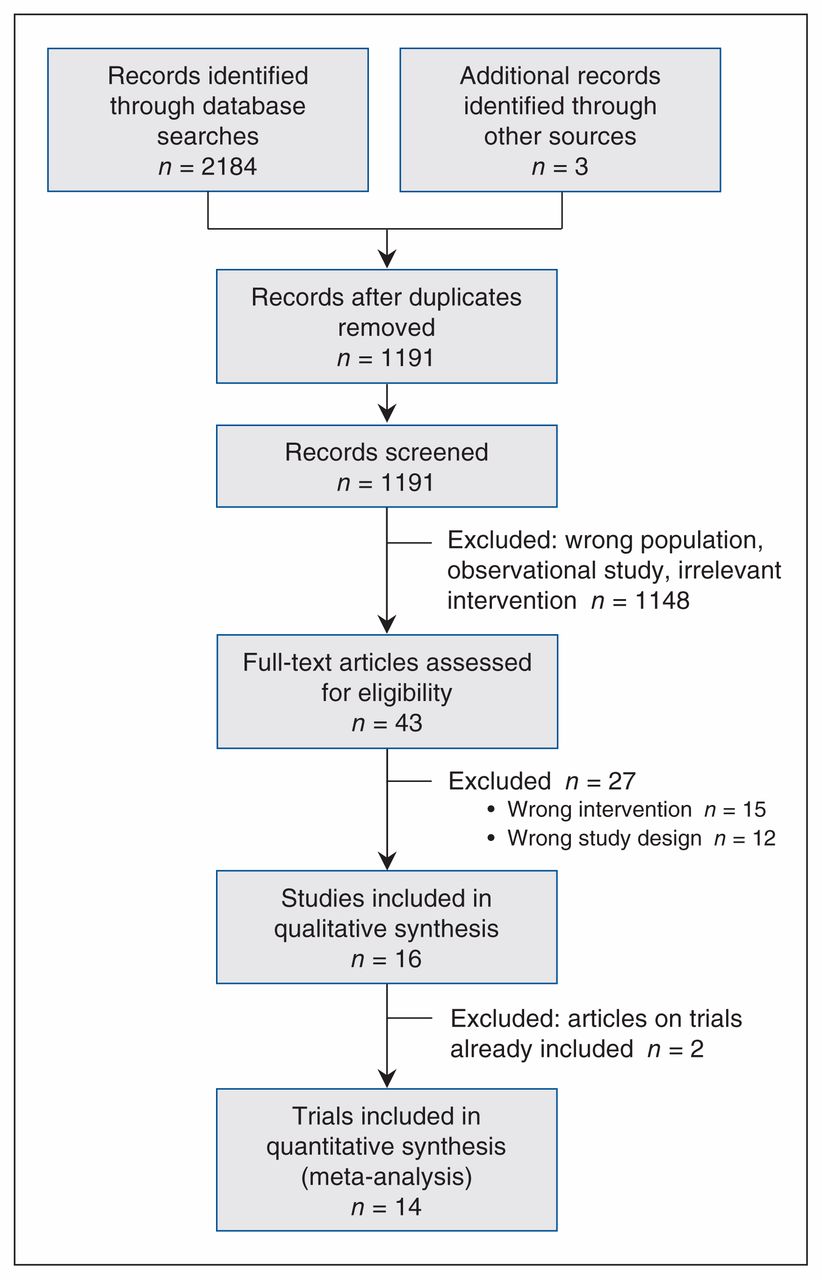
Flow diagram showing study selection.
Study characteristics
The 14 studies assessed in our analysis included 2608 pregnancies (3328 newborns). Nine studies were from developed regions, and 5 were from a developing region (Zimbabwe18–22). Indications for bed rest in the Zimbabwe studies included multiple-gestation pregnancy18–21 and hypertensive disorders of pregnancy.22 Studies evaluating pregnancies in developed regions examined multiple-gestation pregnancy, 23–25 hypertensive disorders of pregnancy,26,27 preterm labour,28,29 suspected intrauterine growth restriction,30 high risk of preterm birth28 and preterm rupture of membranes.31
The length of the prescribed bed rest ranged from 1.0 to 9.7 weeks.18–22,25,27,29,31 A summary of study characteristics is provided in Table 1.
Study characteristics
Quality of evidence
Overall, the quality of evidence ranged from low to high (Supplementary Table S1, Appendix 2, available at www.cmajopen.ca/content/7/3/E435/suppl/DC1). The most common reasons for downgrading the quality of evidence were serious risk of bias and serious imprecision of the interventions. Common sources of bias included selection bias owing to inadequate generation of a randomized sequence and reporting bias owing to selective outcome reporting.
Synthesis of results
Fetal outcomes
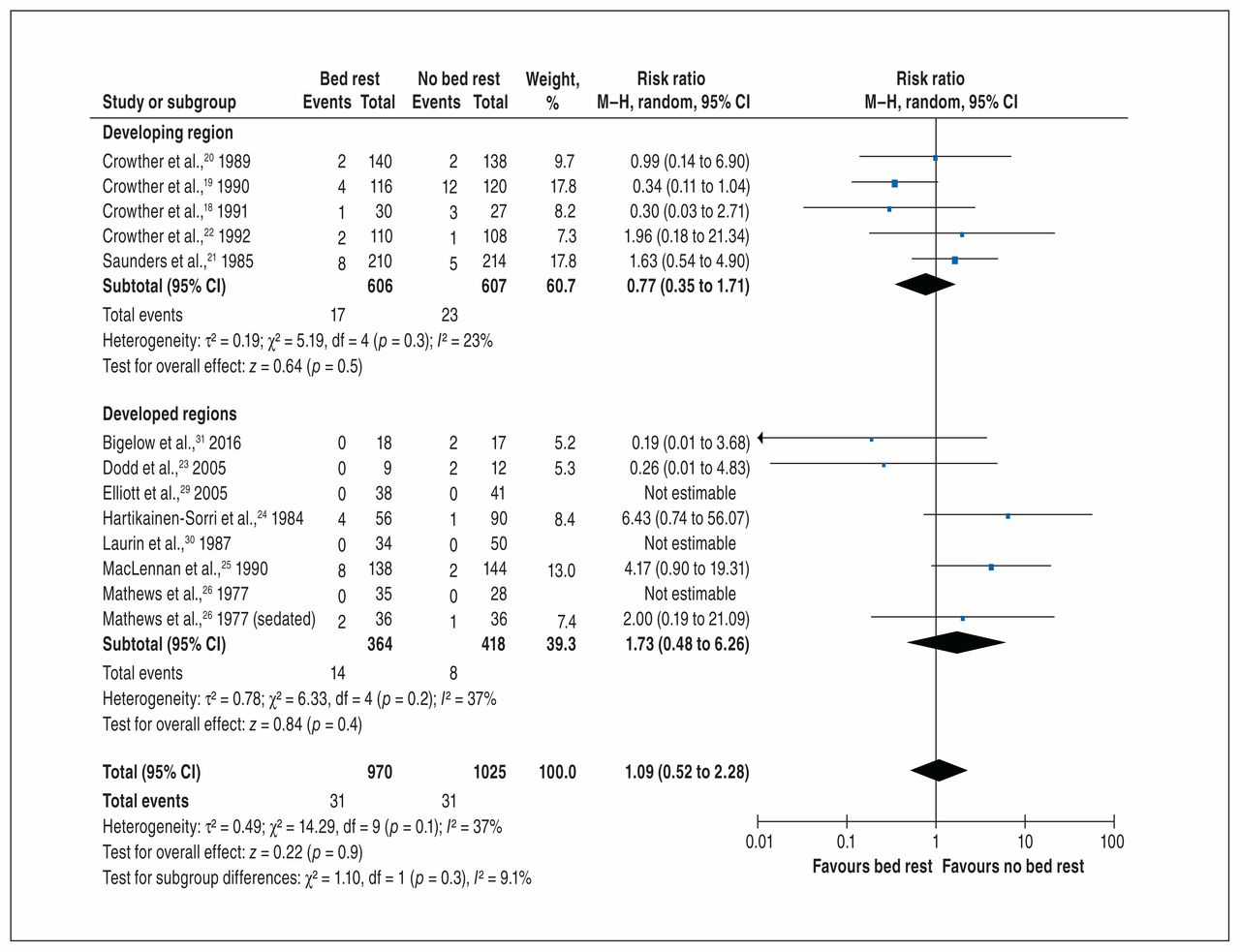
Bed rest did not decrease the risk of perinatal death overall (12 RCTs, 1995 births: 782 in developed regions and 1213 in Zimbabwe; RR 1.09, 95% CI 0.52 to 2.28, I2 = 37% (Figure 2) or when separated by developmental status of the country (p = 0.3 for subgroup differences).18–26,29–31
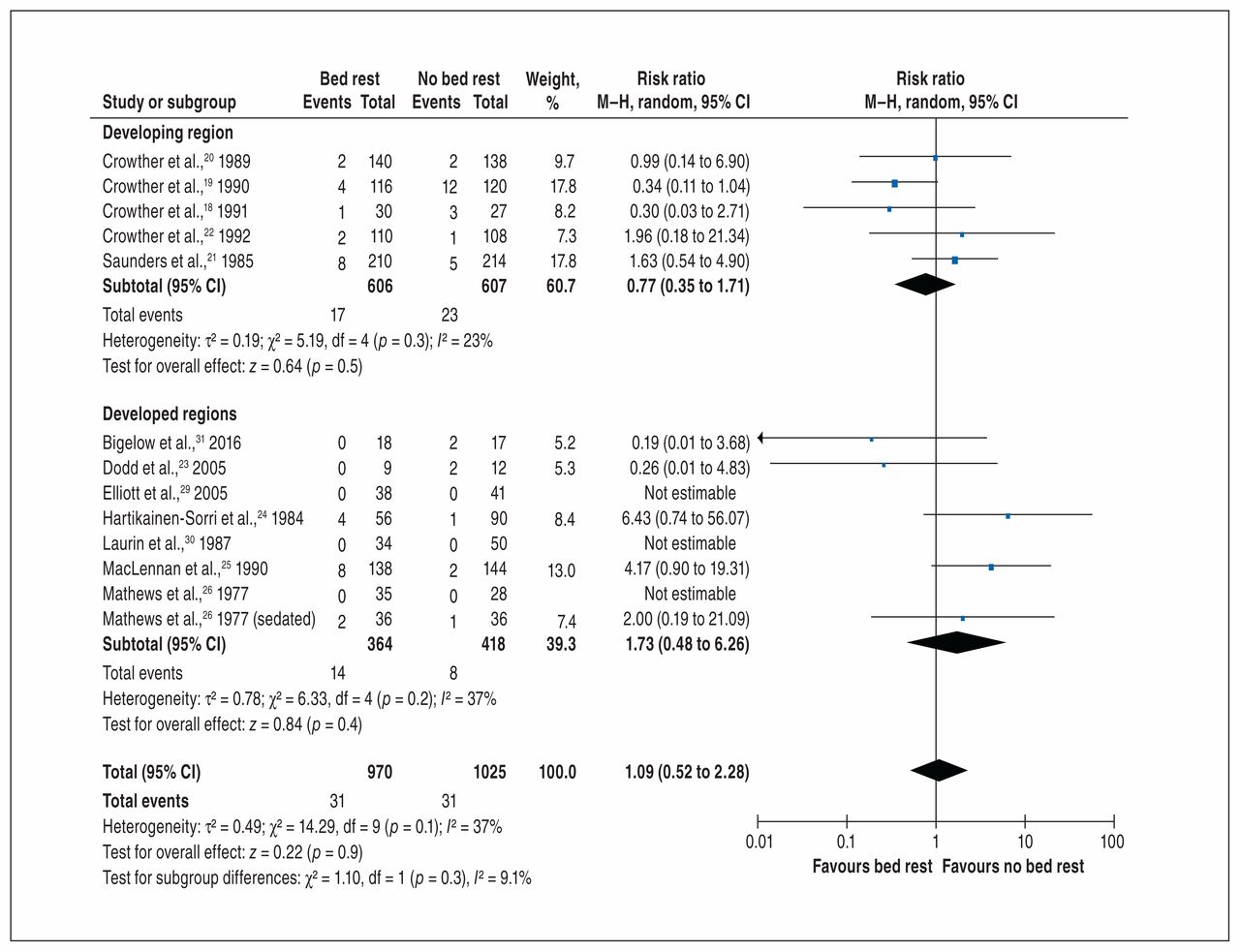
Effect of bed rest (experimental) versus no bed rest (control) on perinatal death. Note: CI = confidence interval, df = degrees of freedom, M–H = Mantel–Haenszel.
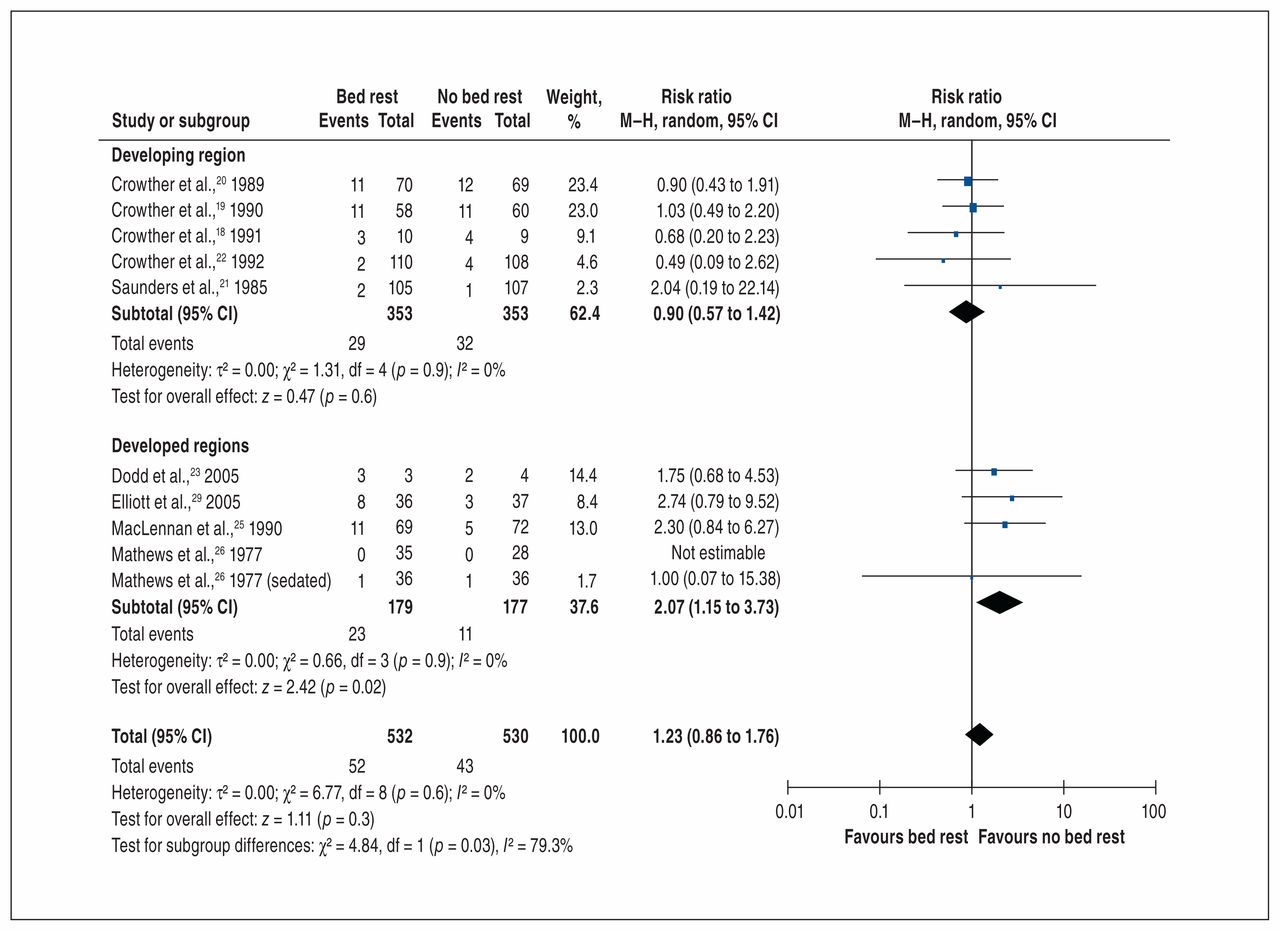
Preterm birth (< 37 wk) and very preterm birth are the leading causes of perinatal morbidity and mortality.32 In our meta-analysis, “very premature” was defined as less than 32 weeks in 2 studies,21,25 less than 34 weeks in 4 studies18–20,23 and less than 35 weeks in 2 studies.26,29 Our analysis of premature birth included 2511 women.18–29,31 No difference was found in rates of premature birth between women on bed rest and those not on bed rest (RR 0.98, 95% CI 0.91 to 1.06, I2 = 0%; low evidence), and subgroup analyses were not significant (Supplementary Figure S1, Appendix 2). High heterogeneity was interrogated in the meta-analysis of very premature birth owing to statistically significant heterogeneity in the developed regions subgroup, which led to the removal of 1 study with a 100% event rate in both study arms.31 Bed rest doubled the risk of having a very premature baby in developed regions (prevalence 6.2% v. 12.8%) (RR 2.07, 95% CI 1.15 to 3.73, I2 = 0%; moderate evidence) (Figure 3) but not the developing region. Subgroup differences were significant (p = 0.03).

Effect of bed rest (experimental) versus no bed rest (control) on very preterm birth. The study by Bigelow and colleagues31 was removed owing to its influence on heterogeneity (heterogeneity of developed regions subgroup p < 0.001; 100% event rate in both study arms). Note: CI = confidence interval, df = degrees of freedom, M–H = Mantel–Haenszel.
Subgroup differences were significant for birth weight (p = 0.02) and gestational age (p = 0.01). Overall, there was high-quality evidence that bed rest was not associated with a greater birth weight compared to no bed rest (1492 births; WMD 40 g, 95% CI −30 g to 110 g, I2 = 31%) (Supplementary Figure S2, Appendix 2).18–20,22,23,25–27,29–31 However, subgroup analysis identified that bed rest modestly increased birth weight in Zimbabwe (WMD 100 g, 95% CI 40 g to 170 g, I2 = 0%; p = 0.002 for subgroup differences; high evidence) but had no impact on birth weight in developed regions.
When gestational age at birth was considered as a continuous variable, women who were on bed rest delivered babies at an earlier gestational age in developed regions (WMD −0.77 wk, 95% CI −1.26 to −0.27, I2 = 0%; moderate evidence) (Figure 4) but not in the developing region (WMD −0.04 wk, 95% CI −0.35 to 0.26, I2 = 6%; high-quality evidence).18–25,29,30,31
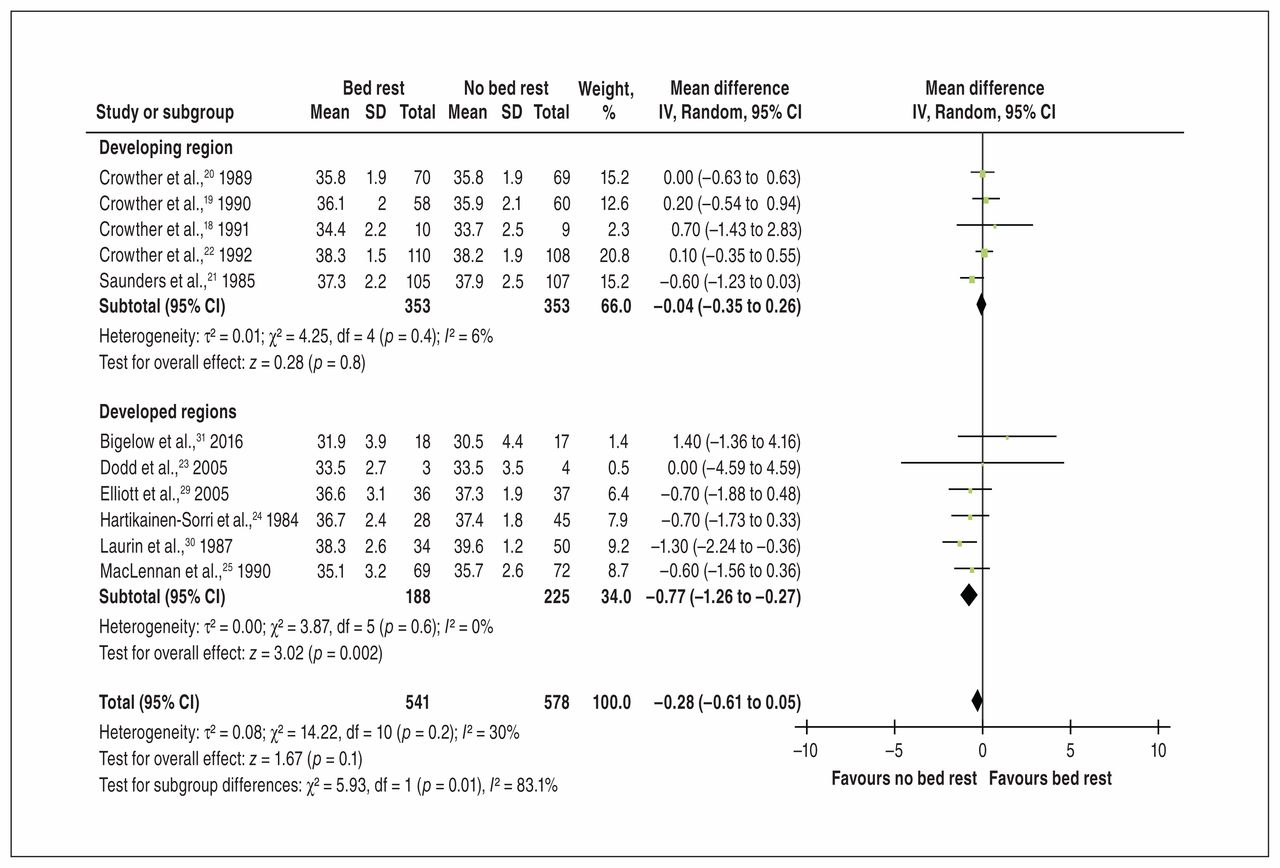
Effect of bed rest (experimental) versus no bed rest (control) on gestational age. Note: CI = confidence interval, df = degrees of freedom, IV = inverse variance, SD = standard deviation.
Overall, moderate-quality evidence indicated that bed rest did not decrease the risk of birth weight less than 2500 g (1837 births; RR 0.92, 95% CI 0.85 to 1.00, I2 = 0% [Supplementary Figure S3, Appendix 2]).18–25,27,29 Bed rest decreased the risk of delivering a baby weighing less than 2500 g in Zimbabwe (RR 0.89, 95% CI 0.81 to 0.98, I2 = 0%; high-quality evidence) but not in developed regions.
The risk of delivering a newborn weighing less than 1500 g (Supplementary Figure S4, Appendix 2),18–21,23–25,29 being small for gestational age (Supplementary Figure S5, Appendix 2)18–20,22,26,27 or being admitted to the neonatal intensive care unit (Supplementary Figure S6, Appendix 2)18–20,22,25,27,29,31 was similar between the bed-rest and no–bed-rest groups. Subgroup analyses were not statistically significant.
Maternal outcomes
Overall, there was low-quality evidence from 10 RCTs (963 women) regarding the association between bed rest and cesarean birth.18–20,22,23,25–27,30,31 The pooled estimate indicated that bed rest did not reduce the rate of cesarean delivery (RR 1.00, 95% CI 0.74 to 1.34, I2 = 31%) (Supplementary Figure S7, Appendix 2). Subgroup analyses were not statistically significant.
Six RCTs (559 women) with low-quality evidence indicated that bed rest did not reduce the risk of hypertensive disorders of pregnancy (RR 0.85, 95% CI 0.51 to 1.42, I2 = 25%) (Supplementary Figure S8, Appendix 2).18–20,23–26 Bed rest also did not reduce the rate of preeclampsia (RR 0.98, 95% CI 0.80 to 1.19) (Supplementary Figure S9, Appendix 2) or preterm rupture of membranes (438 women; RR 1.38, 95% CI 0.85 to 2.26, I2 = 0%) (Supplementary Figure S10, Appendix 2).18–20,25
One moderate-quality RCT25 (downgraded owing to serious inconsistency) (141 women) showed that bed rest did not reduce the rate of gestational diabetes (RR 1.04, 95% CI 0.22 to 4.99) (Supplementary Figure S11, Appendix 2). Funnel plots showed that the outcomes examined were not influenced by publication bias (Supplementary Figures S12 and S13, Appendix 2).
Sensitivity analyses
Eight of the 14 studies included multiple-gestation pregnancies. 18–21,23,25–27 When stratified for singleton or multiple gestation, perinatal death, premature birth at less than 37 weeks, gestational age, birth weight less than 1500 g, birth weight less than 2500 g, being small for gestational age, admission to neonatal intensive care unit, cesarean delivery, preterm rupture of membranes, gestational diabetes, pregnancy-induced hypertension and preeclampsia were all similar between the no–bed-rest and bed-rest groups (Supplementary Figures S14–S27, Appendix 2). Although RCTs examining bed rest for multiple births were more common in the developing region than in developed regions, stratification by singleton-versus multiple-gestation birth explained significantly less heterogeneity than stratification by developmental status of the region.
Interpretation
Overall, maternal and fetal outcomes were similar between women on bed rest and those not on bed rest. However, stratification by the developmental status of the region explained a significant amount of heterogeneity; this has been noted in previous meta-analyses on this topic.5,10,11 Stratification identified a divergent impact of bed rest between groups such that bed rest in developed regions decreased gestational age by 5.4 days and increased the risk of delivering a very premature baby. In contrast, bed rest in the developing region increased birth weight by 100 g and decreased the risk of delivering a baby weighing less than 2500 g.
Six Cochrane reviews have previously examined the impact of bed rest on maternal and fetal outcomes including the prevention of preeclampsia (2 studies, n = 106),33 improving outcomes of pregnancies complicated by hypertension (4 studies, n = 449),10 the prevention of preterm birth (1 study, n =1266),3 impaired fetal growth (1 study, n =107)34 and multiple gestation (7 studies combining complicated and uncomplicated pregnancies, n = 713;5 6 studies including strict or partial bed rest, n = 636).11 In all cases, the investigators concluded that there was insufficient evidence for or against the use of bed rest to improve maternal/fetal health outcomes as a result of small samples and high heterogeneity. In nonpregnant populations, the physiological effects of bed rest are not altered by the indication for bed rest;35 thus, we combined all indications for bed rest during pregnancy. Stratification by developmental status of the region resulted in subgroup heterogeneity of 40% or less for all but 1 subgroup analysis (55%). Hospital admission may explain some of the differences observed between the influence of bed rest in developed versus developing regions. Although bed rest has been shown to decrease maternal weight gain in developed countries,36 admission to hospital in developing countries may afford access to proper nutrition, sanitation, clean water and medical professionals. These factors may overcome some of the negative physiological effects of bed rest in selected populations.
It is beyond the scope of this review to determine whether bed rest or hospital admission itself improved birth weight in studies in Zimbabwe. Additional work is required to dissect the influence of hospital admission versus bed rest in developing regions. Bed rest is likely to drive inflammation, which may increase the risk of preterm birth, necessitating further research on the levels of inflammatory cytokines in pregnant women on bed rest. Although there is a reduction in blood pressure during bed rest,37 other mechanisms of harm such as endothelial dysfunction may lead to further negative effects in pregnancies complicated by hypertension or preeclampsia. As a result, further research may be required in developed regions on the influence of bed rest on pregnancies complicated by hypertension.
Limitations
All trials of bed rest in developing regions were conducted in Zimbabwe. As the rates of maternal and fetal morbidity and mortality in Zimbabwe are among the highest in the world,38,39 our findings from this country may not be generalizable to other developing regions. Furthermore, as all the Zimbabwe studies were conducted between 1984 and 1992, this may limit the applicability of the results for developing countries, as obstetrical practice will have changed over time. In the Zimbabwe studies, bed rest was conducted in hospital, and no bed rest was conducted at home. In developing countries, low birth weight is associated with hypertensive disorders of pregnancy, preeclampsia, nutritional status of the woman, anemia and access to health care.40 Hospital admission may afford improved access to skilled health care workers, sanitation and nutritional status monitoring, thereby reducing the risk of low birth weight.40
Conclusion
Our analyses showed that, in developed regions, 1 additional baby was born very premature for every 15.1 women treated with bed rest. In conjunction with the overwhelming evidence of negative maternal health consequences of prenatal bed rest, our results suggest that bed rest increases the risk of serious negative consequences for newborns in developed regions. In developing regions, bed rest appears to have a minimal positive effect on birth weight, but this finding may be confounded by the effects of hospital admission.
Acknowledgement
The authors thank Sandy Campbell from the John W. Scott Health Sciences Library for peer reviewing the database searches.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Margie Davenport led the review. Rshmi Khurana conceived the project. Margie Davenport, Normand Boulé and Linda Slater designed the search strategy. Margie Davenport, Brittany Matenchuk and Chenxi Cai performed the review. Margie Davenport and Brittany Matenchuk analyzed and interpreted the data. Brittany Matenchuk drafted the manuscript, and Margie Davenport, Rshmi Khurana, Chenxi Cai and Normand Boulé critically revised it for important intellectual content. All of the authors approved the version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding for this project was made possible by the Advancing Women’s Heart Health Initiative National and by an Alberta New Investigator Award to Margie Davenport supported by Health Canada and the Heart and Stroke Foundation of Canada. This research was also funded by generous supporters of the Lois Hole Hospital for Women through the Women and Children’s Health Research Institute.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/7/3/E435/suppl/DC1.
References
- Copyright 2019, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





