


Abstract
Background: Motivated by concerns of inadequate vaccination coverage and the potential for outbreaks of vaccine-preventable diseases, Canadian provinces have been discussing, implementing and tightening policies requiring documentation of vaccination for school enrolment. We sought to understand the acceptability of 14 potential vaccination policy levers among parents and other adults in British Columbia.
Methods: A representative online panel of 1308 adults in BC was surveyed in April 2017. Respondents were representative of the BC population by sex, age, geographic residence and percentage of household with children younger than 19 years. We used Poisson regression to estimate predictors of policy endorsement.
Results: Most respondents (> 80%) held positive attitudes toward vaccination. Policies such as mandatory documentation of vaccination at school entry were supported by more than 75% of all respondents. Punitive policies, such as denial of child tax benefits for nonvaccination, were supported by less than 40% of respondents. In multivariable regression, respondents with positive attitudes toward vaccination were significantly more likely to strongly support all potential policies. Additionally, female respondents and respondents with postsecondary education were significantly more likely to strongly support policies involving additional requirements for parents.
Interpretation: Most adults in BC held favourable attitudes toward vaccination, and strong support existed for policies designed to support vaccination. This study provides evidence that most adults in BC are supportive of vaccination and, when presented with a wide range of options, would likely be supportive of information and requirement policy options designed to increase vaccination uptake.
Canada has limited vaccination requirements for school entry. Only 2 of Canada’s 10 provinces — Ontario and New Brunswick — currently have laws requiring proof of vaccination, and both allow exemptions for medical reasons and for philosophical or religious beliefs.1,2 However, owing to increasing concern regarding outbreaks of vaccine-preventable diseases, school-based interventions to increase vaccination of children have received renewed attention.3 For example, in Ontario, the longstanding Immunization of School Pupils Act1 was amended such that, beginning in 2014, parents or guardians were required to provide proof of vaccination against 9 diseases or were required to file exemptions. In December 2015, Ontario launched multiple initiatives regarding communication, knowledge translation and strengthening the implementation of legislative mandates,4 and, in 2017, required that parents seeking nonmedical exemptions for their children complete an educational session on vaccine evidence.5 However, recent efforts to address decreasing vaccination coverage in some other provinces have encountered resistance. In 2017, the Alberta government declined to adopt a policy of mandatory vaccination for students,6 and in 2018, the Manitoba School Boards Association voted against a motion to lobby the provincial government to adopt stricter school-entry vaccination requirements.7,8
Currently, British Columbia does not require vaccination or even documentation of vaccination for school entry, although that may be changing.9 Vaccination records of school children are collected under a voluntary scheme at school entry, especially at kindergarten age, with more variability in such collection when children enter school at older ages. Public health staff members are authorized to request student records from the school under both the School Act10 and under the Independent School Regulation11 for the purpose of planning delivery of health services to students. As coverage rates in BC children are below national averages for many vaccines,12,13 a better understanding of the acceptability of potential policy levers could provide valuable assistance to policy-makers as they search for methods to increase vaccination rates. The objectives of this study were to assess the level of support in BC in the general population and in parents for a range of policy options designed to increase vaccination rates and to determine the characteristics associated with strong support.
Methods
Sample and procedures
An existing online panel of BC adults was surveyed Apr. 3–14, 2017. We recruited participants by email through the Sentis online consumer research panel. The sample was constructed to match the population distribution by age, sex and households with children younger than 19 years in each of the 5 regional health authorities. Because we were interested in the attitudes of parents of school-aged children, we also oversampled parents of children younger than 19 years to ensure adequate responses for parental questions.
Respondents received an email invitation with a survey link and provided informed consent before proceeding to the survey. A reminder email was sent 3 days after the initial email. Respondents earned points redeemable for retailer gift cards from the panel provider. The panel provider had no input on the study design, analysis or manuscript.
Survey design and development
Our online survey instrument consisted of 24 items pertaining to the topical domains described in the Measures section, as well as demographic questions. The instrument was pilot tested to ensure questions and response options were clear to respondents. A copy of the survey is available on request.
Measures
Support for vaccination policy levers was measured with 14 items assessing support for national and international laws and public proposals14–16 that had been validated in a previous study.16 We classified the policy options into 4 categories (Box 1). The 4-point response scale for these items ranged from 1 (strongly agree) to 4 (strongly disagree), which we recoded in reverse direction to reflect stronger endorsement in our models.
Categorization of policy options Information or service provision
The government should invest more money in research to ensure that vaccines are safe.
Parents need access to more information about childhood vaccinations.
School vaccination rates should be made public.
More child vaccination-related services should exist.
Requirements
At school entry, all parents should be required to provide records showing whether their child has been vaccinated.
Parents who refuse vaccinations for their children should be required to sign a vaccine refusal form.
Parents who refuse vaccinations for their children should be required to attend an education session.
Children should not be allowed to attend public schools without all age-recommended vaccinations without a documented medical reason for not being vaccinated.
Penalties
Parents should be denied their monthly Canada child tax benefit until their children receive all age-recommended vaccinations.
Parents who lose their jobs should be denied unemployment benefits until their children receive all age-recommended vaccinations.
Parents should be required to pay a special tax or fine if their children have not received all age-recommended vaccinations.
Doctors should be allowed to refuse to see families who choose not to vaccinate their children.
Rewards
Parents should receive a financial reward if their children have received all age-recommended vaccinations.
Parents should receive a special tax break or credit if their children have received all age-recommended vaccinations.
Demographic characteristics included sex, age, number of children younger than 19 years in the household, foreign born (v. Canadian born), education level and household income.
Vaccination-related practices consisted of 3 binary (yes/no) items asking respondents whether they had ever delayed or ever refused a vaccine for their child (asked of parents), and ever refused a vaccine for themselves (asked of parents and nonparents).
Normative influences consisted of 2 items assessing whether the respondent had received negative information about vaccines from a) family members and b) friends.17,18
Attitudes toward vaccines consisted of 5 items based on the theory of planned behaviour that assessed the respondents’ attitudes toward vaccines.17–19 Each item was coded on a 4-point scale ranging from 1 (strongly agree) to 4 (strongly disagree).
Statistical analysis
The total sample was weighted for households with children younger than 19 years because we oversampled parents of children younger than 19 years of age using the 2016 Canadian Census. SAS version 9.2 was used for all analyses. We present descriptive data via weighted percentages for the total sample.
Our analyses consisted of 2 steps. First, we computed descriptive statistics for the study variables across 2 groups: total respondents and parents with children younger than 19 years. Second, we used Poisson regression with robust variance20 to estimate predictors of policy endorsement for those who strongly agreed with policies (v. all other responses). We selected this cut-off because it represented the highest degree of endorsement. The demographic, behavioural, normative and attitudinal characteristics described above were examined to determine whether specific policies were more or less likely to appeal to specific population groups. For these models, the 5 questions about vaccine attitude had high internal consistency (Cronbach α = 0.93) and thus were combined into a mean composite measure for vaccine attitudes and reverse coded for ease of understanding (ranging from 1 [strongly disagree] to 4 [strongly agree]). The variables of vaccination-related practices pertaining to whether respondents had every delayed or refused vaccines for their child were combined into one variable with 3 levels: 1) parents who had delayed or refused; 2) parents who had not delayed or refused; and 3) nonparents. Any characteristic with a prevalence ratio above 1 and a p value of 0.05 or less in the multivariable model indicated the characteristic was associated with strong support for the policy, with the prevalence ratio indicating the percent increase (if > 1) or decease (if < 1) in the probability of support for the policy for a characteristic of interest compared with its referent or each unit change in the vaccine attitude scale.
Ethics approval
The University of British Columbia provided research ethics approval.
Results
A total of 1352 invitations were sent, and 1002 adults (aged ≥ 19 yr) responded (74% response rate), with an additional 306 parents enrolled for a total sample size of 1308. Demographic characteristics of the respondents are shown in Table 1. In both the total and the subset of parents with young children, just over half were female (55.2% and 56.6%, respectively), 79.2% were born in Canada and 76.0% had education beyond secondary school. A total of 41.5% (weighted) had no children. Parent respondents were younger and had slightly higher household incomes than total respondents.
Characteristics of 1308 adults in British Columbia surveyed in April 2017 to assess support for potential vaccination policy levers
Vaccination practices, normative influences and attitudes
Vaccination practices and normative influences (friends and family) are shown in Table 1. Comparing parents of children younger than 19 years of age (henceforth termed “parents of young children”) with parents of older children or respondents without children, more parents of young children reported knowing friends or family members who had refused vaccines. Vaccine attitudes among the total participants and parents of young children are shown in Figure 1 (the full survey results are available in Appendix 1, www.cmajopen.ca/content/7/2/E264/suppl/DC1). The mean of the vaccine-attitudes composite measure on a 4.0 scale was 3.37 (standard deviation [SD] 0.61) for the total sample and 3.30 (SD 0.62) for parents of young children.
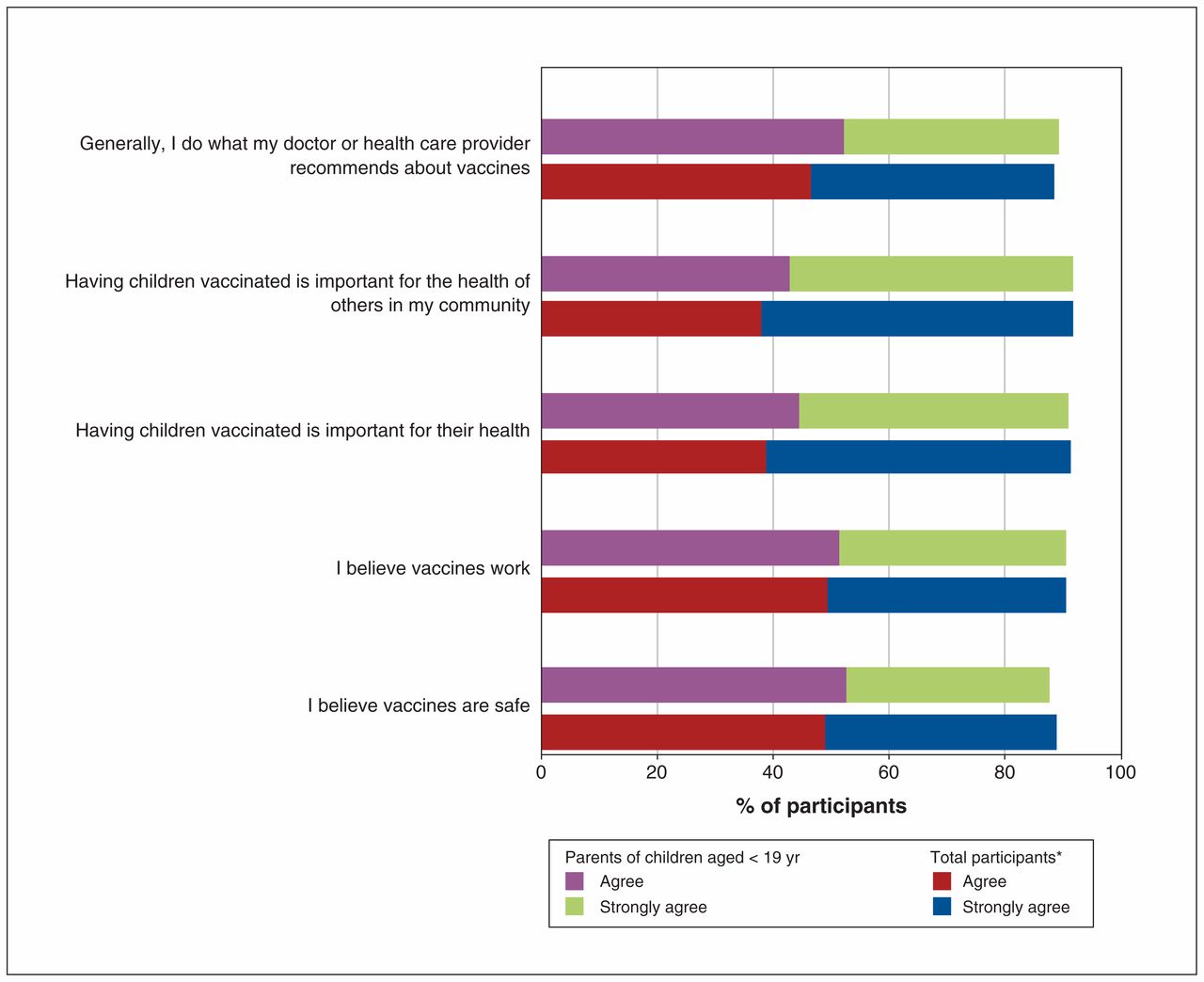
Proportion of respondents who agreed with positive vaccine statements. *Population percentages for the total are weighted for households with children younger than 19 years.
Support for vaccination policies
Figure 2 shows the proportion of respondents who either agreed or strongly agreed with 14 specific vaccination policies (the full survey results are available in Appendix 2, www.cmajopen.ca/content/7/2/E264/suppl/DC1). Policies pertaining to information and services received the highest level of agreement from all respondents as well as parents of young children. Policies that establish additional requirements for parents received agreement from most survey respondents, including both parents and nonparents. Rewards, or policies that provided incentives to vaccinating parents, were supported by more than half of parents of young children but received less support among total respondents (p < 0.005). Finally, penalties were supported by a minority of respondents, regardless of parental status, with particularly low support for the denial of unemployment benefits to nonvaccinating parents.
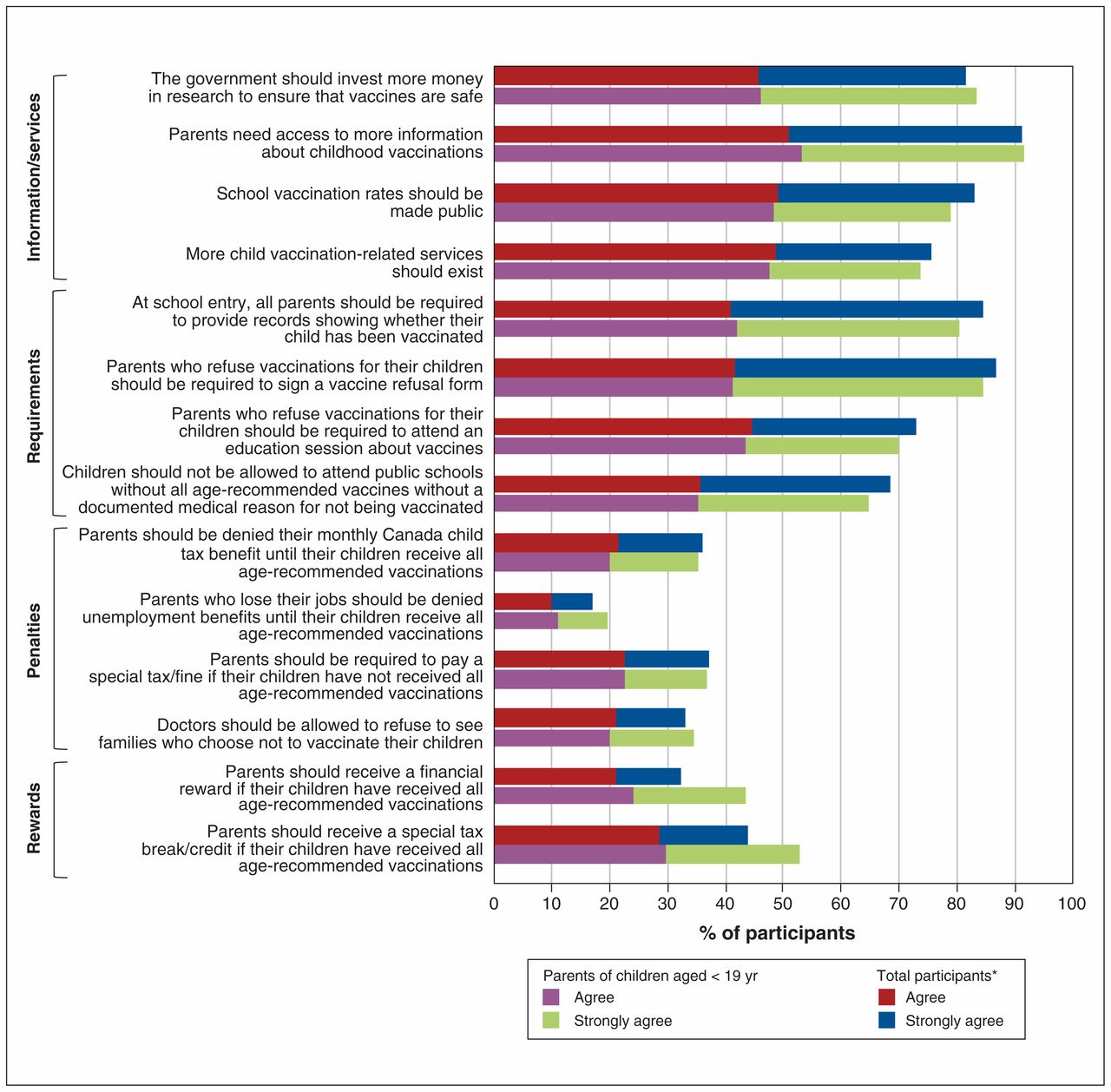
Proportion of respondents who agreed with 14 vaccination policies. *Population percentages for the total are weighted for households with children younger than 19 years.
Multivariable analyses of vaccination-policy support
Tables 2 and 3 show the adjusted prevalence ratios obtained from multivariable models regressing the demographic, behavioural, normative and attitudinal characteristics on strong support for each policy.
Multivariable prevalence ratios for strongly agreeing with specific vaccination policies pertaining to information and services, and requirements*
Multivariable prevalence ratios for strongly agreeing with specific vaccination policies pertaining to penalties and rewards*
Demographic factors, in general, showed inconsistent associations across policies. However, some patterns existed. Women were significantly more likely to endorse support for information and services, and requirement policies (e.g., vaccine record provision [prevalence ratio 1.21], signed refusal [prevalence ratio 1.23] and education sessions [prevalence ratio 1.24]). Younger participants were significantly more likely to support some penalties (denying unemployment benefits [prevalence ratio 2.81 for the age group 18–24 yr, and 2.03 for the age group 25–34 yr], and applying taxes or fines [prevalence ratio 1.83 for the age group 25–34 yr, and 1.63 for the age group 35–44 yr) and reward policies, and parents of young children were significantly more likely to support reward policies. Lower income was associated with support for information and services (e.g., research funding [prevalence ratio 1.43] and more vaccination services [prevalence ratio 1.40]), and participants with higher education (e.g., beyond secondary) had a significantly higher likelihood of supporting policies of school vaccination rates being made public (prevalence ratio 1.42), parents being required to provide vaccination records (prevalence ratio 1.25) and signed refusals (prevalence ratio 1.23), doctors’ refusing unvaccinated patients (prevalence ratio 1.66), school bans of unvaccinated students (prevalence ratio 1.22) and denial of child tax benefits (prevalence ratio 2.00).
Regarding vaccination practices, normative influences and vaccine attitudes, having positive vaccine attitudes was the only covariate predictive of support for 13 out of 14 policies. No behavioural or normative influence was consistently associated with policy support (or nonsupport). However, having normative influences that delayed or refused vaccines, or having been provided negative information about vaccines, did predict greater support for policies pertaining to information and services. Parents who had delayed or refused vaccines for their child did not support requiring signed vaccine refusal forms (prevalence ratio 0.78).
In terms of the predictors associated with the different policy categories, policies pertaining to information and services varied in terms of predictors associated with strong support, with positive vaccination attitudes being the only common covariate associated with strong support across all but 1 of these policies. This category of policy was the only one to receive strong support from respondents who had delayed or refused vaccines for their children (prevalence ratio 1.24 for more government-funded research, and 1.33 for more information access). In general, requirement policies were more strongly supported by women, participants with postsecondary education and participants with positive attitudes toward vaccination. Penalty policies were strongly supported by participants with positive vaccination attitudes, men, participants with higher incomes and those in younger age groups. Importantly, several population groups, such as women and immigrants, were significantly less likely to support penalty policies. Finally, rewards were most strongly supported by those in younger age groups (i.e., of child-bearing age) and those with young children.
Interpretation
This study examines the support for a variety of vaccination policy options and identifies the factors associated with this support. Overall, these findings indicate that vaccination is a strongly supported social norm among our sample of BC adults, and that several nonpunitive policies might be well accepted. British Columbians expect parents to vaccinate their children, and for most policies, support is similar among parents and the general public — with the exception of greater support among parents for policies that directly benefit these parents (i.e., financial rewards or tax breaks). Depending on the policy, successful implementation may require special attention (e.g., communication and logistical assistance) be paid to specific populations to facilitate acceptance. Some populations, such as those who do not support vaccination or who do not have strong attitudes in support of vaccines, may be unlikely to agree with any measures directly affecting them.
Public support is important for the success of vaccination policy to minimize risks of unintended consequences from population backlash. Moreover, public attitudes toward such policies can vary substantially depending on context. For example, whereas California’s recent revision of their school vaccination law (allowing only medical exemptions in public schools) appears to have been well-received by the majority, Italy has experienced substantial backlash to recent tightening of childhood vaccine policy (requiring more vaccines and imposing financial penalties).21,22 In our study, policies involving additional requirements for parents garnered support from most respondents, which was similar to the support seen in California, where 67% of adults and 65% of parents of public school children felt that children who have not been vaccinated should not be allowed to attend school.23 By contrast, more punitive policies, such as denial of child tax benefits or other government benefits or services — similar to the “no jab, no pay” policy14,24,25 in Australia — were not viewed favourably in our study. Less than 15% of respondents indicated strong support, and important population groups, such as women and immigrants, indicated strong disagreement. Implementation of an unpopular policy could potentially undermine attempts to increase vaccine coverage, as has been seen in Italy and other jurisdictions.22,26
Limitations
These findings need to be considered with respect to some limitations. First, our data are from a nonprobability online panel. Using a volunteer sample may introduce selection bias, as those who participate may be different from nonparticipants. Nevertheless, our sample was representative of the BC population by geography, sex, age and proportion of households with children. The proportion in our survey who delayed or refused vaccines (26%) for their child was similar to population rates at 30% of 7-year-old children in BC.12
Conclusion
This study provides evidence that most BC adults are supportive of vaccination and would likely be supportive of nonpunitive policy options designed to increase uptake of vaccines. Similar context-specific research conducted in other jurisdictions in Canada, the United States and beyond would benefit public discourse and government decision-making. This is especially true in locations where vaccination policy is hotly debated. Often in such settings, debate is fueled by anecdote in media stories or, at best, public surveys containing 1 or 2 items about vaccinations that offer limited information for such a nuanced issue. Furthermore, governments would benefit from future research focusing on the extent to which such policy attitudes might remain stable over time, including before and after introduction of a particular policy, and even compared and contrasted with attitudes in other provinces or jurisdictions.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Julie Bettinger, Devon Greyson and Richard Carpiano contributed substantially to the conception and design, acquisition of data, and analysis and interpretation of data. Pamela de Bruin, Issy Aguiar, Monika Naus and Brett Hodson contributed substantially to the conception and design. Julie Bettinger wrote the manuscript, which the other authors revised critically for important intellectual content. All authors gave final approval of the version to be published and agreed to act as guarantors of the work.
Funding: This study was funded by the British Columbia Immunization Committee, a subcommittee of the Communicable Disease Policy Committee.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/7/2/E264/suppl/DC1.
References
- Copyright 2019, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.