


Abstract
Background: Screening colonoscopy for the detection of colorectal carcinoma is provided by several specialties. Few studies have assessed geographic variation in the delivery of this care. Our objective was to investigate how geographic and socioeconomic factors affect who provides screening colonoscopy in Canada.
Methods: This was a population-based cohort of all screening colonoscopy procedures performed at publicly funded Canadian health care facilities (excluding those in Quebec) between April 2008 and March 2015. The main outcome of interest was the proportion of colonoscopy procedures performed by surgeons versus gastroenterologists at the neighbourhood level. Predictors of interest included socioeconomic and geographic variables. We used spatial analysis to evaluate significant clustering of practitioner services and multinomial logistic regression to model predictors.
Results: We identified 658 113 screening colonoscopy procedures performed by 1886 providers (1169 surgeons and 717 gastroenterologists) over the study period, of which 353 165 (53.7%) were performed by surgeons. A total of 24.2% of neighbourhoods were located within clusters predominantly served by gastroenterologists, and 19.5% were within surgeon clusters; the remainder were in mixed clusters. Rural neighbourhoods had a significantly increased relative risk of being within a surgeon cluster (relative risk [RR] 5.38, 95% confidence interval [CI] 3.48-8.01) compared to mixed clusters and nearly 100 times higher relative risk of being in a surgeon cluster compared to gastroenterologist clusters (RR 98.95, 95% CI 15.3-427.2). Neighbourhoods with the highest socioeconomic status were 1.74 (95% CI 1.14-2.56) times likelier to be in gastroenterologist clusters than in mixed clusters.
Interpretation: Surgeons provide a large proportion of colonoscopy procedures in Canada and are essential for access to care, particularly in rural regions. Most Canadians are served relatively equally by surgeons and gastroenterologists. This emphasizes the importance of both specialties to the delivery of colonoscopy care across the country.
Colorectal cancer is the third most commonly diagnosed and fourth most common cause of cancer-related death in men and women, respectively, worldwide.1 In 2012, 1.4 million people received a diagnosis of colorectal cancer, and it was estimated that 700 000 of these people would die from the disease.1 High disease incidence and mortality have led to the development of multiple screening modalities, many of which detect and remove colonic polyps that are precursors to many colorectal cancers.2 Of these, colonoscopy is most sensitive test for detecting colorectal cancer and adenomas.3 As a common primary screening test, colonoscopy has been shown to decrease the incidence of colorectal cancer and associated mortality,4,5 and a recent meta-analysis suggested that it is a more effective screening tool than guaiac-based fecal occult blood testing or flexible sigmoidoscopy.6
There is conflicting evidence as to whether endoscopist specialty affects patient outcomes. Some studies have shown that, compared to patients treated by general surgeons or other specialists, patients who underwent colonoscopy performed by a gastroenterologist were significantly more likely to have polyps detected7-9 and removed10 and had lower rates of bowel perforation,11 and colorectal cancer was less likely to develop in these patients.12 However, other studies have revealed no significant difference in polyp detection13 or complication rates14 between gastroenterologists and surgeons, with at least 1 study showing that gastroenterologists have significantly higher total complication rates than surgeons.13 Despite these findings, little is known as to whether the populations these specialists serve are the same and how important either specialty is to the delivery of colonoscopy care, as provider delivery in urban and rural areas has been found to vary.15 In addition, residents of rural areas have been shown to have lower screening rates than urban residents16-18 and a higher proportion of their colonoscopy procedures done by general surgeons.15 Furthermore, the nature of the 2 professions differs and allows for varied roles in the delivery of endoscopy. Gastroenterologists can be more focused and may have a high-volume endoscopy practice, but their specialty may not be as suitable to rural areas. Few researchers have investigated geographic variations in the delivery of colonoscopy and what factors affect that variation. This information is vital to understanding and planning the delivery of colonoscopy care as well as contextualizing differences in outcomes. As such, the purpose of this study was to investigate variations in the delivery of screening colonoscopy by specialty across Canada.
Methods
Design and setting
This was a retrospective cohort study of all adult (age ≥ 18 yr) patients who underwent screening colonoscopy in a publicly funded facility between April 2008 and March 2015 in Canada (excluding Quebec). Screening colonoscopy guidelines are relatively similar across Canadian provinces, and major evidence for colorectal screening did not change during the study period, as the Canadian Task Force on Preventive Health Care updated their guidelines in 2016 from the 2001 guidelines.3,19
Data sources and definitions
We defined screening colonoscopy as a procedure aiming to detect and remove polyps and/or early-stage lesions.19 We derived patient, procedure, provider, distance and neighbourhood data from the Canadian Institute for Health Information Discharge Abstract Database and National Ambulatory Care Reporting System. We excluded Quebec as its data are not accessible directly from the Canadian Institute for Health Information but only through the Quebec Ministry of Health and Social Services. We identified screening colonoscopy by a colonoscopy procedure clarified by a screening diagnosis code. Both databases have been previously validated, and both showed high sensitivity for procedures.20-22 Other administrative databases have been validated for colonoscopy, with a 99% correlation with the correct procedure and a specificity of 76% in 1 study and over 95% in another study for the correct indication.23,24 We defined neighbourhoods as forward sortation areas, which are a unit of area used by the Canadian postal system denoted by the first 3 digits of the postal code. We derived geographic data for the forward sortation areas from the 2013 Canadian census files25 and obtained neighbourhood income data from Statistics Canada. Rurality was defined through the postal code.26,27 The median individual income for each neighbourhood was the specific income measure used and was derived from Statistics Canada data.27
Outcome measures and regression variables
The main outcome of interest in this study was the neighbourhood ratio of screening colonoscopy procedures done by surgeons versus gastroenterologists/internists. Colonoscopy procedures done by other providers accounted for less than 2% of all procedures and were excluded. The main geographic and socioeconomic factors of interest were distance to the colonoscopy facility, neighbourhood rurality and neighbourhood socioeconomic status.
Statistical analysis
We calculated the main outcome as the proportion of total colonoscopy procedures within a neighbourhood done by surgeons. To determine the spatial relation between neighbourhoods and specialty, we performed a geographic cluster analysis using the Getis-Ord Gi* statistic. This statistic determines whether the neighbourhood and all of its adjacent neighbours are significantly different from the overall mean. For this analysis, we defined neighbourhood connectivity as having an adjacent border. Neighbourhood clusters were then classified as a surgeon cluster, a gastroenterologist cluster high use or a mixed cluster. We carried out spatial analyses using the ArcGIS Desktop suite (ArcMap10.1, Environmental Systems Research Institute). We compared univariable comparisons of geographic and socioeconomic factors across surgical rate groups and clusters using analysis of variance or a χ2 test, as appropriate. To determine the effect of the neighbourhood and socioeconomic factors on neighbourhood cluster status, we used a multilevel multinomial logistic regression with the geographic and socioeconomic factors as fixed effects and the provinces as random effects. Importantly, this methodology allows for an unbiased evaluation of the effects by accounting for differences in use between provinces. Results are presented as surgeon and gastroenterologist neighbourhoods compared to mixed neighbourhoods, as well as surgeon neighbourhoods compared directly to gastroenterologist neighbourhoods. Owing to the use of multinomial regression, we report relative risk (RR) with 95% confidence intervals (CIs). Statistical significance was set at p < 0.05. We used Stata statistical software release 12.1 (StataCorp) and MLwiN version 2.26 (Centre for Multilevel Modelling, University of Bristol) for data analysis.
Ethics approval
This study was approved by the Hamilton Integrated Research Ethics Board.
Results
A total of 658 113 screening colonoscopy procedures were performed over the study period, 353 165 (53.7%) by surgeons (n = 1169) and 304 948 (46.3%) by gastroenterologists (n = 717). Surgeons performed 100 195 colonoscopy procedures (28.4% of their total colonoscopy procedures) in rural areas, compared to 37 893 procedures (12.4%) for gastroenterologists (p < 0.001) (Table 1). A third (32.9%) of procedures done by gastroenterologists were done in neighbourhoods with the highest socioeconomic status, compared to 17.7% for surgeons (p < 0.001). Patients of surgeons travelled farther than patients of gastroenterologists (mean 27.0 km v. 21.3 km, p < 0.001).
Figure 1 and Table 2 present the results of the cluster analysis. Of the 1114 neighbourhoods analyzed, 270 (24.2%) were within a cluster that had significantly higher rates of colonoscopy care provided by gastroenterologists, and 217 (19.5%) were within a cluster that had significantly higher rates of care provided by surgeons; the remainder were in mixed clusters. In gastroenterologist clusters, surgeons performed 22.7% of colonoscopy procedures, whereas in mixed clusters and surgeon clusters, they performed 53.5% and 83.0% of procedures, respectively. Only 2 (0.7%) of the gastroenterologist cluster neighbourhoods were rural areas, compared to 75 (34.6%) of the surgeon cluster neighbourhoods. In addition, 63.0% of gastroenterologist cluster neighbourhoods were in the 2 highest categories of economic status, compared to 31.8% of surgeon cluster neighbourhoods. Surgeon clusters were nearly 42 km farther from the colonoscopy facility than were gastroenterologist clusters (59.4 km v. 17.7 km). This clearly shows the rural predominance of surgeon clusters, whereas major urban areas tended to be served by gastroenterologists; in suburban areas and smaller cities, care delivery was generally mixed between surgeons and gastroenterologists.
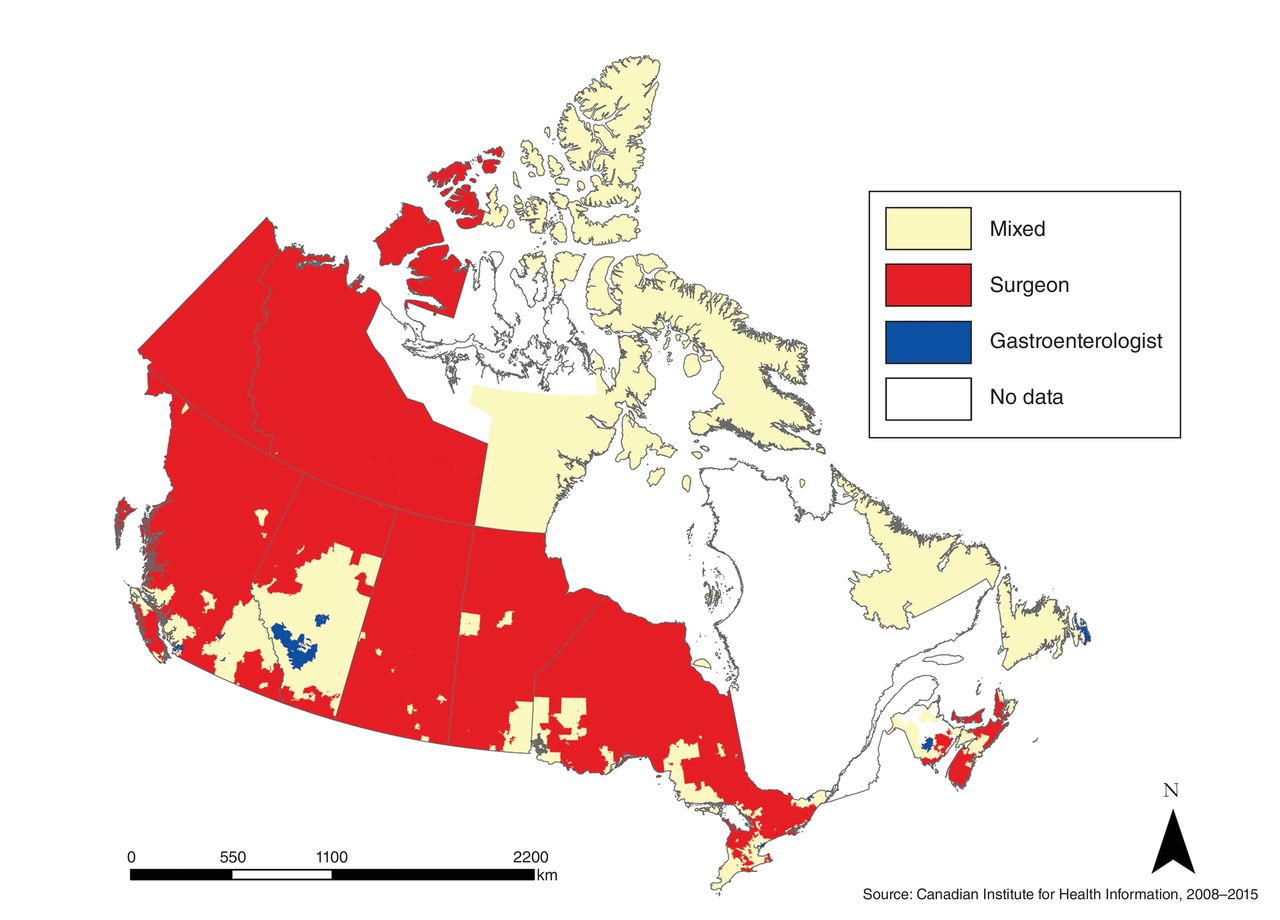
Neighbourhood clustering of screening colonoscopy providers in Canada, April 2008 to March 2015.
Compared to a mixed neighbourhood cluster, a rural neighbourhood was 0.12 (95% CI 0.01-0.35) times less likely to be in a gastroenterologist cluster and 5.38 (95% CI 3.48-8.01) times more likely to be in a surgeon cluster (Table 3). A neighbourhood in the highest socioeconomic quintile was 1.74 (95% CI 1.14-2.56) times more likely to be in a gastroenterologist cluster than in a mixed cluster and 0.60 (95% CI 0.33-1.00) times less likely to be in a surgeon cluster. Distance was significant only for gastroenterologist clustering: for every 50 km farther from the colonoscopy facility that a neighbourhood was, the relative risk of being a gastroenterology cluster neighbourhood compared to a mixed cluster neighbourhood was 0.76 times lower (95% CI 0.58-0.93).
A rural neighbourhood was 98.95 (95% CI 1.3-427.2) times more likely to be in a surgeon cluster than in a gastroenterologist cluster (Table 4). A neighbourhood in the highest socioeconomic quintile was 0.35 (95% CI 0.18-0.61) times less likely to be in a surgeon cluster than in a gastroenterologist cluster. Last, for each 50 km farther from the colonoscopy facility that a neighbourhood was, it was 1.37 (95% CI 1.10-1.77) times more likely to be in a surgeon cluster than in a gastroenterologist cluster.
Interpretation
We identified significant patterns in the geographic variation in the delivery of screening colonoscopy in Canada that were consistent across provinces. Overall, there was a clear rural-urban divide between surgeon- and gastroenterologist-delivered care. Surgeons performed 53.7% of all screening colonoscopy procedures and 73% of procedures in rural areas. Accordingly, rural neighbourhoods were nearly 100 times more likely to be in a surgeon cluster than a gastroenterology cluster and more than 5 times more likely to be in a surgeon cluster than a mixed cluster. In nonrural areas, surgeons provided 48.7% of the overall screening colonoscopy care, although this was spread around suburban areas and smaller cities, whereas gastroenterologist care was clustered within major cities such as Toronto, Vancouver, Edmonton, Calgary and Ottawa. This division of the delivery of care was also manifested in the fact that gastroenterologists tended to treat patients of the highest socioeconomic status as well as those who had to travel shorter distances to the health care facility.
Our results are consistent with the finding of Baxter and colleagues28 that surgeons performed 53% of colonoscopy procedures in Ontario. Schultz and colleagues29 also found that gastroenterologists and surgeons performed almost the same total number of procedures, although gastroenterologists tended to perform more procedures per physician. Variations in provider distribution between urban and rural areas have also been identified. Hilsden and colleagues15 reported that gastroenterologists provided colonoscopy care primarily in large urban areas, whereas surgeons tended to dominate provision of care in smaller urban and rural areas in Canada. However, they could look only at total numbers and were not able to determine whether significant clustering exists. Importantly, a recent systematic review identified a notable lack of studies assessing who provides colonoscopy care in rural areas.16 Lower rates of colorectal cancer screening in rural areas17,18 suggest a need for increased provision of colonoscopy care in these regions.
There is evidence that colonoscopy procedures performed by surgeons have similar morbidity and mortality rates as those performed by gastroenterologists.14,30,31 In a study of Ontario residents, Rabeneck and colleagues12 found that patients who underwent colonoscopy performed by a nongastroenterologist were at significantly increased risk for later development of colorectal cancer. In addition, Ko and colleagues7 reported that gastroenterologists were significantly more likely than other specialists to detect and remove polyps during outpatient colonoscopy. However, Kozbial and colleagues13 found no significant differences in the rate of polyp or carcinoma detection between general surgeons and internists. However, Baxter and colleagues28 did not find a significant association between endoscopist volume and important outcomes such as later development of colorectal cancer.
Our findings clearly show the importance of both gastroenterologists and surgeons in delivering colonoscopy care in Canada. In most neighbourhoods in Canada, the delivery of care is split evenly between the specialties. In addition, their roles seem complementary, as they allow each to provide colonoscopy care in areas where the other would not be able to. Specifically, in rural areas, surgeons fill the gaps in care owing to their ubiquity and ability to supplement their endoscopy practice with a surgical practice. In high-density urban areas, gastroenterologists can fill gaps in coverage where surgeons would likely not be able to meet demand. Recognizing this phenomenon may be a key for provincial health care systems to ensure access to colonoscopy for all patients.32,33 This finding also emphasizes the need for endoscopy training for both specialties during residency. This is a specific highlight for surgical programs, in which endoscopy accounts for only part of procedure volume. This training and credentialing during residency is even more important for surgeons planning to practise in rural areas.
The observed division of care also helps to contextualize findings related to practitioner volumes, as it may not be possible for rural surgeons to have high-volume endoscopy practices. Therefore, in an effort to provide access to colonoscopy care, it may be necessary to recognize this fact when creating credentialing guidelines with regard to yearly endoscopy volumes. Guidelines based on the practice of high-volume urban practitioners may have the effect of limiting access to colonoscopy care for patients. Therefore, ensuring access to quality colonoscopy care in rural areas will be an ongoing challenge for the health care system.
Limitations
This study has several limitations. It covered only colonoscopy procedures that were done in publicly funded health care facilities. The proportion of procedures performed in private endoscopy centres across Canada is largely unknown.34 Previous studies showed that, between 1993 and 2005, 84.4% of colonoscopy procedures performed in Ontario were done in hospitals, 11.4% were performed in nonhospital settings, and 4.1% were not classifiable.35 Considering that most private endoscopy centres are in urban centres and are run by high-volume endoscopists, it is unlikely that including them would have changed the overall message of this study. In addition, we did not cover all colonoscopy care but, rather, focused on screening. The purpose of including only screening colonoscopy was to encompass an overlapping area of practice for surgeons and gastroenterologists, as many other indications for colonoscopy would not overlap as evenly. There is a lack of data on potential provider-level confounders such as years in practice, and this may have influenced the validity of our findings. Last, the authors of the study who are practising physicians are all urban general surgeons and provide colonoscopy care to the community.
Conclusion
This study clearly shows the division in delivery of screening colonoscopy between rural and urban areas. In rural areas, surgeons were the predominant specialty providing colonoscopy care, whereas gastroenterologists accounted for a larger burden of care in high-density urban areas. This finding underscores the importance of both specialties in achieving access to colonoscopy care for all Canadians. It also highlights the importance of endoscopy in surgical training, especially for those not planning to practise in urban areas. Future research should focus on how this spatial pattern of practice affects outcomes.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/6/1/E126/suppl/DC1.
Footnotes
Competing interests: None declared.
Contributors: Aristithes Doumouras, Sama Anvari and Dennis Hong designed the study, acquired and analyzed the data and drafted the manuscript. Margherita Cadeddu, Mehran Anvari and Dennis Hong critically revised the manuscript for important intellectual content. All of the authors made substantial contributions to the study conception and the interpretation of the data, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
References
- Copyright 2018, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools





