


Abstract
Background: Antimicrobials are frequently prescribed to community-dwelling older adults. Our aim was to examine the prevalence, quantity and indications of antimicrobial prescriptions to older residents of Ontario.
Methods: We conducted a population-based analysis of outpatient antimicrobial prescriptions to residents of Ontario aged 65 years or more from 2006 to 2015. Antimicrobial prescriptions, infectious disease diagnoses and prescriber information were determined from linked health care databases. Our analyses were primarily focused on antibiotics, which account for most antimicrobial use.
Results: We identified 2 879 779 unique Ontario residents aged 65 years or more over our study period. On average, 40.7% (range 40.1%-41.5%) of older adult outpatients in any given year received 1 or more antibiotic prescriptions. Antibiotic use remained stable over the study period, averaging 25.1 (range 24.1-25.6) defined daily doses per 1000 person-days per year. Selection of antibiotics evolved, with increasing use of penicillins and decreasing use of fluoroquinolones and macrolides. For 65.7% of prescriptions, no infectious disease diagnoses were identified within 7 days of the prescription. Among prescriptions with an associated diagnosis, upper respiratory tract infection was most common (18.9%), followed by urinary tract infection (6.2%), skin/soft-tissue infection (4.3%), lower respiratory tract infection (4.2%) and other infection (1.2%). Most antibiotics were prescribed by family physicians.
Interpretation: Antibiotic use among older adult outpatients in Ontario remained stable between 2006 and 2015. Current methods of measuring use are not capable of accurately determining indication, and, thus, additional data sources to monitor the appropriateness of community antimicrobial use are needed.
Antimicrobials are among the most commonly prescribed medications in Canada. Most are dispensed in an outpatient setting, accounting for 93% of total use in 2014.1 Many prescriptions are unnecessary or inappropriate, with antibiotics given for viral illnesses and increasing use of broad-spectrum agents.2-7 The evaluation of outpatient antimicrobial use is of pressing importance, as misuse is the primary driver of antimicrobial resistance.8 Patients prescribed antibiotics in primary care are more likely to develop antibiotic-resistant infections,9 and higher outpatient antimicrobial use has been associated with increased resistance, in both community and health care settings.10-14 Overuse is also associated with greater health care costs and more adverse events.15-17 Furthermore, the correlation between in-hospital antimicrobial use and resistance has been found to be poor, which suggests that outpatient prescribing drives much of inpatient resistance.18,19
Judicious use of antimicrobials is particularly important for older adults, who are prescribed these medications more frequently than younger people.1,20-23 Antimicrobials are the fourth most common drug class prescribed among older adults in Ontario.24 Older adults are at greater risk for adverse drug events than younger people25,26 and have high rates of colonization with antimicrobial-resistant organisms.27-29
Several initiatives have raised awareness of inappropriate antimicrobial use and have promoted prudent prescribing.30,31 However, interventions for outpatient antimicrobial stewardship are challenging to implement,32 and surveillance of ambulatory prescribing in Canada has been limited despite calls to prioritize such efforts.33 The objective of our study was to describe patterns of outpatient antimicrobial prescribing in older residents of Ontario from 2006 to 2015.
Methods
We conducted a province-wide analysis of antimicrobial prescriptions to older adults (aged ≥ 65 yr) in Ontario from Jan. 1, 2006, to Dec. 31, 2015.
Data sourcesThis study used population-based administrative databases housed at the Institute for Clinical Evaluative Sciences. These databases are well validated and have been used in studies on antimicrobial prescribing.34-38 The Ontario Drug Benefit Program database, which contains all publicly funded medications prescribed to Ontario residents aged 65 years or more, was used for information on antimicrobial prescribing. This database exhibits greater than 99% accuracy when compared against pharmacy dispensing data.34 To identify older adults and determine infectious disease diagnoses, the following databases were linked to the Ontario Drug Benefit Program database at the patient level: the Registered Persons Database, which contains demographic information for Ontario residents with publicly funded health insurance (> 95% of residents); the Ontario Health Insurance Plan database, which contains all billing claims made by health care providers for services performed in Ontario; the Discharge Abstracts Database, which contains information on all admissions, discharges and same-day surgical procedures in Ontario hospitals; and the National Ambulatory Care Reporting System, which contains information on all emergency department visits in Ontario hospitals.
Antimicrobial prescriptions
We used the Registered Persons Database to identify all Ontario residents aged 65 years or more as of Jan. 1 of each calendar year during our study period. Residents who had no contact with the health care system in the 7 years preceding assessment, or who died or moved out of province between calendar years were excluded. We then used the Ontario Drug Benefit Program database to determine the proportion of older adults who were prescribed an antimicrobial in each study year. Antimicrobials were classified into 1 of 4 categories: antibiotics, antivirals, antifungals and antiparasitics (Appendix 1, available at www.cmajopen.ca/content/5/4/E878/suppl/DC1).
Antibiotic prescriptions
Our subsequent analyses were focused on antibiotics, as this is the most frequently prescribed category of antimicrobials and because resistance to antibiotics is of greatest public health concern.8 Using the Ontario Drug Benefit Program database, we determined the quantity of each antibiotic class and antibiotic drug prescribed to older adults in each study year. Antibiotics were grouped into 14 classes, with antitubercular agents removed from the analyses (Appendix 2, available at www.cmajopen.ca/content/5/4/E878/suppl/DC1). Antibiotic use was measured in defined daily doses per 1000 person-days. Defined daily doses are a standardized metric of drug use based on an assumed average daily maintenance dosage.39 We calculated person-days as the total number of adults aged 65 years or more residing in Ontario in each study year multiplied by the number of days in that year.
Indications for antibiotic prescriptions: Each antibiotic prescription was subsequently linked to the physician claim, hospital discharge, same-day surgery and emergency department databases to identify any infectious disease diagnoses recorded within 7 days before or after the prescription. Diagnoses were grouped into the following categories: upper respiratory tract infection, lower respiratory tract infection, urinary tract infection, skin/soft-tissue infection, other infection and no recorded infection. We determined the proportion of use of each antibiotic class and antibiotic drug associated with each clinical indication.
Antibiotics prescribed for infectious disease diagnoses: We identified all infectious disease diagnoses recorded in the Ontario Health Insurance Plan database, Discharge Abstracts Database and National Ambulatory Care Reporting System for 2006 and 2015. These diagnoses were linked to the Ontario Drug Benefit Program database to examine whether a prescription for an antibiotic was filled in the 7 days before or after each diagnosis. We determined the overall numbers of antibiotic prescriptions as well as the 10 most commonly prescribed antibiotics for each diagnosis category.
Responsible prescribers
To determine the health care providers most responsible for outpatient antibiotic use among older adults, we determined the proportion of prescriptions, in individual claims and defined daily doses, attributable to family physicians and specialists. This analysis was conducted for 2006 and 2015.
Statistical analyses
Analyses were performed with SAS statistical software version 9.3 (SAS Institute Inc.) and R statistical software version 3.2.2 (R Foundation for Statistical Computing).
Ethics approval
Ethics approval was obtained from the Sunnybrook Health Sciences Centre Research Ethics Board.
Results
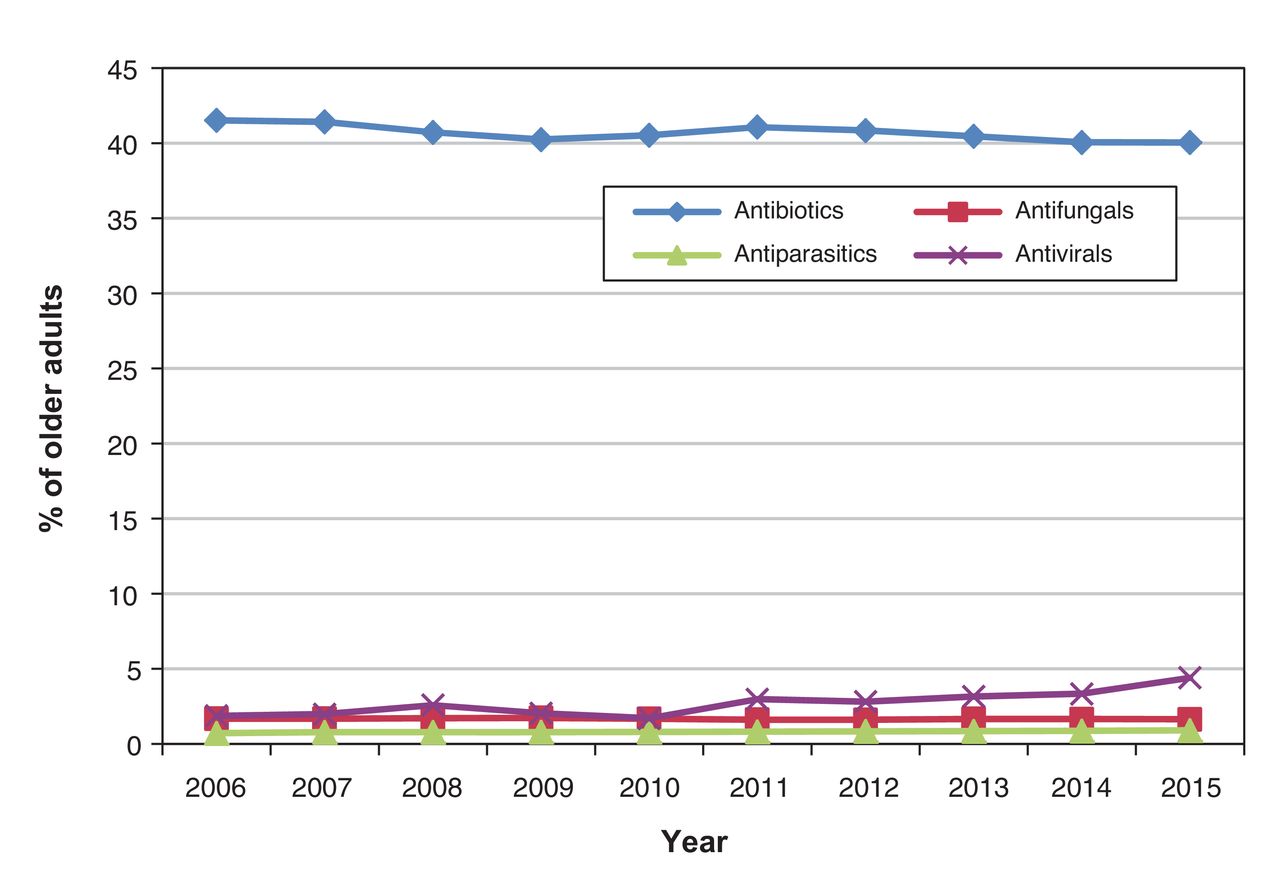
During the study period, 2 879 779 unique residents of Ontario aged 65 years or more were identified. The population of older adults increased from 1 646 909 in 2006 to 2 176 736 in 2015. On average, 40.7% (range 40.1%-41.5%) of older adult outpatients received an antibiotic prescription in any study year, and 2.7%, 1.7% and 0.8% were prescribed an antiviral, antifungal and antiparasitic, respectively. The proportion of older adults prescribed an antiviral increased from 1.9% in 2006 to 4.4% in 2015 (p < 0.001); antimicrobial use was otherwise stable across the 10 study years (Figure 1). Prescriptions for antibiotics, antifungals and antivirals increased with increasing age. In 2015, 142 569 residents (49.2%) aged 85 years or more were prescribed an antibiotic, compared to 242 555 (34.2%) of those aged 65-69 (p < 0.001). Similar increases between the 2 age strata were seen for antivirals (42 511 [14.7%] v. 12 487 [1.8%], p < 0.001) and antifungals (6354 [2.2%] v. 8886 [1.3%], p < 0.001).
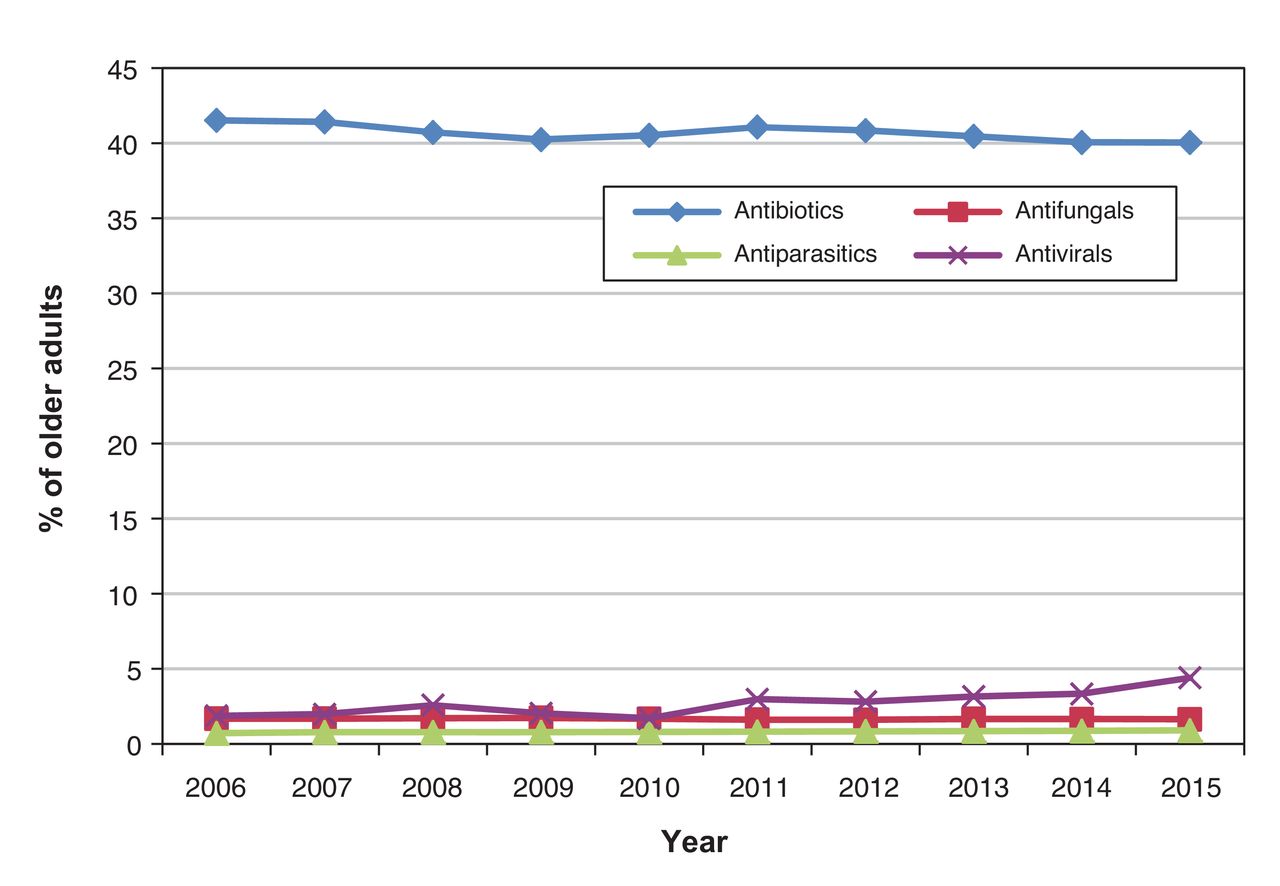
Proportion of Ontario residents aged 65 years or more who received at least 1 outpatient antimicrobial prescription, 2006-2015, by antimicrobial class.
Antibiotic prescriptions
The average quantity of antibiotics prescribed per year was 25.1 (range 24.1-25.6) defined daily doses per 1000 person-days. Antibiotic use remained relatively stable between 2006 and 2015, decreasing slightly from 25.6 to 24.1 defined daily doses per 1000 person-days.
The 5 most frequently prescribed antibiotic classes were penicillins, fluoroquinolones, macrolides, cephalosporins and urinary anti-infectives. Trends in their use are shown in Figure 2. Prescriptions for penicillins increased from 6.1 to 7.8 defined daily doses per 1000 person-days between 2006 and 2015. Prescriptions for fluoroquinolones and macrolides decreased over the study period, whereas cephalosporin and urinary anti-infective use remained stable. The rise in penicillin prescriptions was driven by greater use of amoxicillin, from 4.7 to 5.7 defined daily doses per 1000 person-days, and of amoxicillin-clavulanic acid, from 0.68 to 1.8 defined daily doses per 1000 person-days (Appendix 3, available at www.cmajopen.ca/content/5/4/E878/suppl/DC1). Among fluoroquinolones, use of both ciprofloxacin and moxifloxacin declined; among macrolides, clarithromycin use decreased, whereas azithromycin use increased. Nitrofurantoin accounted for most urinary anti-infectives.

Total outpatient prescriptions, in defined daily doses per 1000 person-days, of the 5 most commonly prescribed antibiotic classes, 2006-2015.
Indications for antibiotic prescriptions
Over the study period, 65.7% of antibiotics prescribed to older adults did not have a corresponding infectious disease diagnosis detectable within 7 days of the prescription (Appendix 3, white bar segments). The most frequently identified diagnosis was upper respiratory tract infection, associated with 18.9% of prescriptions, followed by urinary tract infection (6.2%), skin/soft-tissue infection (4.3%), lower respiratory tract infection (4.2%) and other infection (1.2%). Upper respiratory tract infection was the most common diagnosis associated with penicillins and macrolides, and urinary tract infection was most common with nitrofurantoin and trimethoprim-sulfamethoxazole. Among fluoroquinolones, ciprofloxacin was associated with urinary tract infection, and moxifloxacin was associated with upper and lower respiratory tract infections. For cephalosporins, skin/soft-tissue infections were the most common diagnosis associated with cephalexin, and upper respiratory tract infection was most common with cefuroxime (Appendix 3).
Antibiotics prescribed for infectious disease diagnoses
Upper respiratory tract infection was the most common diagnosis associated with an antibiotic prescription. There were 184 667 upper respiratory tract infections associated with antibiotic prescriptions in 2006; this increased to 211 549 prescriptions in 2015. Increased use of amoxicillin (0.80 to 0.98 defined daily doses per 1000 person-days) and amoxicillin-clavulanic acid (0.10 to 0.29 defined daily doses per 1000 person-days), and decreased use of clarithromycin (1.10 to 0.53 defined daily doses per 1000 person-days), moxifloxacin (0.18 to 0.13 defined daily doses per 1000 person-days) and levofloxacin (0.16 to 0.13 defined daily doses per 1000 person-days) were observed over the study period (Figure 3, A).

Outpatient prescriptions, in defined daily doses per 1000 person-days, of the 10 antibiotics most commonly prescribed for (A) upper respiratory tract infections, (B) urinary tract infections, (C) lower respiratory tract infections and (D) skin/soft-tissue infections in 2006 and 2015. Note: TMP/SMX = trimethoprim-sulfamethoxazole, Amox/Clav = amoxicillin-clavulanic acid.
Urinary tract infections were the second most common indication for outpatient antibiotics: 75 645 antibiotic prescriptions for this diagnosis were identified in 2006, and 100 648 were identified in 2015. Use of nitrofurantoin increased from 0.27 to 0.34 defined daily doses per 1000 person-days between 2006 and 2015. Prescriptions for fluoroquinolones declined over the study period, driven largely by a decrease in norfloxacin use, from 0.21 to 0.07 defined daily doses per 1000 person-days; ciprofloxacin use increased slightly. Likewise, prescriptions for trimethoprim-sulfamethoxazole decreased, from 0.22 to 0.14 defined daily doses per 1000 person-days (Figure 3, B).
Lower respiratory tract infection was the third most common indication for outpatient antibiotic treatment in this population: 48 408 lower respiratory tract infections were associated with antibiotic prescriptions in 2006, and 66 273 in 2015. A substantial decrease in macrolide use was observed. Clarithromycin was the most frequently prescribed antibiotic in 2006, but use declined substantially in 2015 (0.29 to 0.15 defined daily doses per 1000 person-days). In contrast, prescriptions for amoxicillin (0.05 to 0.14 defined daily doses per 1000 person-days) and amoxicillin-clavulanic acid (0.03 to 0.13 defined daily doses per 1000 person-days) increased. There were small declines in prescriptions for fluoroquinolones, although levofloxacin was the most commonly prescribed antibiotic for this indication in 2015 (Figure 3, C).
Last, 45 453 antibiotic treatments were prescribed for skin/soft-tissue infections in 2006, and 64 882 in 2015. Cephalexin was the most commonly prescribed antibiotic in both years, increasing from 0.36 to 0.47 defined daily doses per 1000 person-days between 2006 and 2015. Cloxacillin, ciprofloxacin and clarithromycin were less commonly prescribed in 2015 than in 2006, whereas use of clindamycin and amoxicillin-clavulanic acid increased between the 2 years (Figure 3, D).
Responsible prescriber
Family physicians accounted for most antibiotic prescriptions to older adult outpatients (Table 1). Antibiotic prescriptions by both family physicians and specialists increased from 2006 to 2015, with proportionately more specialist prescriptions in 2015.
Interpretation
This study of 2 879 779 older residents of Ontario showed that ambulatory antimicrobial use remained stable from 2006 to 2015. Two-thirds of antibiotic prescriptions did not have a corresponding infectious disease diagnosis within 7 days of the prescription.
We observed increasing use of amoxicillin and amoxicillin-clavulanic acid, and decreasing use of fluoroquinolones and macrolides over our study period. These results diverge from the rise in use of broad-spectrum antibiotics reported in prior studies.2,5,20 This may represent a positive change, with physicians favouring narrow-spectrum agents where appropriate. However, overall outpatient antibiotic use was consistent over our study period, averaging 25.1 defined daily doses per 1000 person-days per year, with 40.7% of older adults receiving a prescription. A 2016 national report on antimicrobial use in Canada showed a similar rate of use in this population (23.0 defined daily doses per 1000 person-days per year) but a higher proportion receiving a prescription (86%).1 Our findings suggest that antibiotic prescribing has not been curtailed by existing interventions. Given that more than 90% of antimicrobials are prescribed in outpatient care, community-based efforts are urgently needed, particularly targeting upper respiratory tract and urinary tract infections, the most common diagnostic indications in our study. Interventions should be directed to family physicians, who accounted for more than 70% of antimicrobial prescriptions to older Ontario residents. However, prescriptions by specialists remain common and rose between 2006 and 2015, with dermatologists and internists previously identified as high-frequency prescribers.1
The antibiotics prescribed for upper respiratory tract infections changed over our study period. Fluoroquinolone and macrolide use declined, and penicillin use increased, which contrasts with previous analyses showing rising selection of the former classes.2-4,6,7 This is in keeping with guidelines recommending amoxicillin or amoxicillin-clavulanic acid as first-line therapy for bacterial upper respiratory tract infections.40-42 However, upper respiratory tract infections were the most common diagnoses associated with antibiotic prescriptions in our study, even though most cases are viral and guidelines discourage routine antibiotic therapy.40-43 Other jurisdictions have similarly found high rates of antibiotic use for upper respiratory tract infections.1,5,20 This highlights the potential impact a community-based antimicrobial stewardship program could have in reducing overall antibiotic use.
We also found increased penicillin use and decreased macrolide use for lower respiratory tract infections. Although macrolides are recommended as first-line therapy for outpatient community-acquired pneumonia,44 resistance rates in Streptococcus pneumoniae have approached 25% in Canada.1,45,46 Thus, macrolides should not be used as monotherapy in this context. The need for "atypical" coverage in treating community-acquired pneumonia has also been questioned.47 Within the macrolide class, growing preference for azithromycin over clarithromycin was observed. This finding may be explained by ease of administration, with single daily versus twice-daily dosing, as well as studies showing equivalency between 3-day courses of azithromycin and longer courses of clarithromycin.48,49 Another reason for the preference for azithromycin over clarithromycin may be greater awareness of drug interactions involving cytochrome P450, with CYP3A4 being inhibited by clarithromycin but not azithromycin.50
For urinary tract infections, use of nitrofurantoin increased. This is in accordance with guidelines recommending this agent as first-line therapy for urinary tract infections owing to high susceptibility rates and low risk to host flora.51 In contrast, use of trimethoprim-sulfamethoxazole declined. This may reflect increasing recognition of its adverse effects,52 particularly among older patients coprescribed common cardiovascular and renal medications.37,53,54 Prescriptions for ciprofloxacin decreased as well, which may be owing to rising awareness of the risks associated with fluoroquinolones.55-58
Cephalexin was consistently the most commonly prescribed antibiotic for skin/soft-tissue infections. Use of clindamycin and amoxicillin-clavulanic acid increased over the study period, which may reflect a change in practice to cover anaerobic organisms as well as methicillin-resistant Staphylococcus aureus in the case of clindamycin. However, clindamycin is associated with the highest risk of Clostridium difficile infection among antibiotics.59,60
The fact that two-thirds of antibiotics prescribed were not associated with a recorded infectious disease diagnosis suggests that our databases were unable to capture most antibiotic indications, even in the context of a universal single-payer health care system, access to linkable physician claim, hospital discharge, same-day surgery and emergency department databases, and the use of a broad 7-day window around prescriptions to identify diagnoses. Effective surveillance of community antibiotic use will require more comprehensive methods of capturing antibiotic indication, such as linkage to electronic medical records and mandatory reporting of diagnosis with each prescription.
Limitations
Antibiotic prescriptions and infectious disease diagnoses were linked through their presence within 7 days of one another. Although these antibiotic-diagnosis associations are likely accurate given their temporal proximity, we could not ascertain causation. We identified diagnoses using infectious-disease-specific diagnostic codes; broader systems-based codes may have improved our linkage rates. For inpatient diagnoses, captured in the Discharge Abstracts Database, date of admission was taken as the date of diagnosis. Diagnoses around outpatient antibiotic prescriptions, and vice versa, may consequently have been missed, particularly in cases long hospital stays and infections fully treated in hospital. Furthermore, the Ontario Health Insurance Plan database allows for only a single diagnosis to be recorded in each claim; infectious disease diagnoses may have been unrecorded in visits involving multiple diagnoses. Another limitation is our categorization of diagnoses. Disease-specific diagnoses, such as acute bronchitis and acute rhinosinusitis, would have allowed us to better assess antimicrobial appropriateness. Last, defined daily dose may be an inaccurate measure of drug use in patients with renal impairment, a common comorbidity in older populations.
Conclusion
In our analysis of outpatient antimicrobial use among older adults in Ontario, we observed a trend toward greater selection of narrow-spectrum antibiotics. However, total use was stable from 2006 to 2015, and antibiotics were frequently prescribed for upper respiratory tract infections. This emphasizes that misuse and overuse of antibiotics remain a problem. Interventions to improve antibiotic prescribing in ambulatory care are therefore warranted. In addition, two-thirds of antibiotic prescriptions were not associated with an infectious disease diagnosis, which shows that existing methods of surveillance in Ontario are not capable of determining antibiotic indication. Given the lack of information on outpatient antibiotic use in Canada, efforts to monitor the quantity, composition and appropriateness of community use need to be strengthened. Our results can be used to guide such efforts and to benchmark antimicrobial stewardship interventions among outpatients.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/5/4/E878/suppl/DC1.
Footnotes
Competing interests: None declared.
Contributors: Nick Daneman, Hong Lu and Erin Graves conceptualized and designed the study, and developed the statistical analysis plan. Nick Daneman and Charlie Tan analyzed and interpreted the data and drafted the manuscript. Hong Lu, Anna Chen and Shudong Li contributed to data acquisition and analysis. Kevin Schwartz contributed to data interpretation and manuscript revision. All of the authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was supported by a Canadian Institutes of Health Research Clinician Scientist Salary Award to Nick Daneman and an Applied Health Research Question fund via the Institute for Clinical Evaluative Sciences.
Disclaimer: This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by the ICES or the Ontario MOHLTC is intended or should be inferred.
References
- Copyright 2017, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools


