


Abstract
Background Since 2010, tamper-resistant long-acting oxycodone has been available in both the United States and Canada; however, generic non–tamper-resistant brands of the drug have only been introduced in Canada. We aimed to determine whether the introduction of generic non-tamper-resistant oxycodone in Canada led to increased sales from Canadian pharmacies near the Canada–US border.
Methods We conducted a retrospective analysis of trends in dispensing of long-acting oxycodone from Canadian community pharmacies in geographic areas contiguous with the Canada–US border between Feb. 1, 2012, and Jan. 31, 2014. We reported the monthly dispensing rates of long-acting oxycodone by province and within each region near the Canada–US border.
Results During the study period, 8 507 882 long-acting oxycodone tablets were dispensed by Canadian pharmacies in regions near Canada–US border crossings. After the introduction of generic non–tamper-resistant formulations in December 2012, the dispensing rate declined in the border regions of Ontario, British Columbia and Quebec, and rose slightly in Manitoba (4.4%) and New Brunswick (3.6%). Dispensing rates rose by 45.5% in Alberta and 92.3% in Saskatchewan; however, only 3341 of the tablets dispensed were a generic non–tamper-resistant formulation. An examination of the dispensing patterns in 50 border areas after the marketing of non–tamper-resistant brands in Canada showed no patterns suggestive of trafficking.
Interpretation We found no large increases in the dispensing rates of generic non–tamper-resistant long-acting oxycodone in Canadian pharmacies near Canada–US border crossings such as were seen after the withdrawal of OxyContin in the United States in 2010. Despite our findings, Canadian clinicians and pharmacists should remain cautious in their prescribing and dispensing of non–tamper-resistant formulations of oxycodone because of their high potential for misuse and abuse.
Since its introduction in 1996, long-acting oxycodone has been the target of regulatory efforts to curb misuse, including changes in regulatory policy, product labelling and product formulation.1–7 The August 2010 introduction of a tamper-resistant formulation of long-acting oxycodone in the United States and the immediate removal of the original formulation (OxyContin) from the American market were seen as important steps in reducing the likelihood of misuse.8 The original form of OxyContin remained available in Canada until late 2011, and we reported that an excess of about 250 000 tablets were dispensed by retail pharmacies on the Canadian side of the Detroit–Windsor tunnel from August 2010 to October 2011.9 This was rapidly reversed after warnings were issued to prescribers and pharmacies.5
In August 2011, Purdue Pharma received a notice of compliance from Health Canada to market a tamper-resistant formulation of OxyContin in Canada, OxyNEO. In contrast to the US Food and Drug Administration (FDA),7 Health Canada authorized the marketing of generic non–tamper-resistant versions of long-acting oxycodone that are pharmacologically equivalent, and similar in appearance, to OxyContin in November 2012.7 This reintroduction of long-acting oxycodone products with no tamper-resistant properties reopened the potential for prescribing behaviour similar to that seen previously. 9
Given the potential for abuse, the differential availability of generic non–tamper-resistant formulations of long-acting oxycodone between the US and Canada has raised concerns of large-scale, organized, drug-seeking behaviour across the international border. We analyzed dispensing data from Canadian pharmacies near the Canada–US border to look for evidence of trafficking of these products.
Methods
We included all prescriptions for long-acting oxycodone dispensed by Canadian pharmacies located in areas adjacent to Canada–US border crossings (by land, bridge or ferry) between Feb. 1, 2012, and Jan. 31, 2014. This period includes the date of introduction of generic long-acting oxycodone to the Canadian market (Nov. 26, 2012). We studied dispensing close to 113 border crossings, excluding the 3 crossings between Yukon and Alaska because of incomplete dispensing records. Dispensing regions near border crossings were delineated by forward sortation areas, a well-established unit of aggregation for Canadian postal codes.10 In some cases, several border crossings lay within 1 dispensing region. In total, the 113 border crossings included in our analyses were mapped to 50 dispensing regions (Appendix 1, available at www.cmajopen.ca/content/3/2/E231/suppl/DC1). Only prescriptions from prescribers licensed to practise in Canada can be filled in Canadian pharmacies. We included all prescriptions for long-acting oxycodone dispensed by retail pharmacies within each forward sortation area in the study.
To obtain estimates of both publicly and privately funded prescriptions for long-acting oxycodone, we used the IMS Brogan Geographic Prescription Monitor database to quantify retail prescription volumes for all long-acting oxycodone products for our study period. This database captures data from a representative sample of 5700 retail pharmacies across Canada, which provides monthly estimates by geographic area at the product form and strength levels. These projections used methods that incorporate factors including the number of pharmacies in a given region, the distance between IMS-captured and uncaptured pharmacies and the sizes of the pharmacies.11 IMS Brogan continuously monitors all data received from the retail pharmacies to ensure that they are within the standards set for quality control, and the resulting product-level projected volumes are representative of all pharmacies in Canada. These data have been used extensively in research on drug use and are viewed as the best source for providing representative data on prescribing trends in Canada.9,12,13 During our 2-year study period, we obtained the monthly prescription volumes (numbers of tablets dispensed) for all long-acting oxycodone products for each of the 50 dispensing regions, stratified by formulation type (brand name v. generic). Tablet numbers are presented at the levels of province and dispensing region, and are expressed as dispensing rates (number of tablets dispensed per 1000 population) using the relevant Statistics Canada census population estimates as the denominator.
Because several forward sortation areas are rural, sparsely populated and less likely to be sources of trafficked drugs, we conducted additional analyses of long-acting oxycodone prescription volumes in more populated areas close to (but not contiguous with) the Canada–US border. In each province, we identified 2 cities with populations greater than 10 000 that were within 150 km (93 miles) of a border crossing (Appendix 1). We excluded Ontario, the most populous province, from this exercise because we included highly populated Ontario centres in proximity to the Canada–US border in the primary analysis. We defined dispensing regions in these cities using forward sortation areas, and we evaluated long-acting oxycodone volumes in the same way as in the primary analysis. We visually inspected the graphs showing prescribing rates over time, because we were unable to obtain sufficient historical data to enable formal time series analyses.
Results
We identified between 1 and 8 border crossings within each of the 50 dispensing regions. The population density of the dispensing regions varied substantially, from 0.14 residents/km2 (near the Rainy River International Bridge between Ontario and Minnesota) to 4796 residents/km2 (near the Victoria–Port Angeles ferry crossing between British Columbia and Washington). During the study period, 8 507 882 long-acting oxycodone tablets were dispensed by pharmacies in these regions. Between the first full month of availability of generic long-acting oxycodone (December 2012) and the end of the study period, generic formulations comprised 11.6% of the total number of dispensed tablets, although this proportion varied considerably by province (from 0.1% in Saskatchewan to 29.3% in Quebec, Appendix 1).
Dispensing volumes did not change dramatically at the provincial level during the study period (Figure 1). Reductions were seen in overall dispensing of long-acting oxycodone in the border regions of Ontario, British Columbia, Quebec and New Brunswick. Volumes remained consistent in Manitoba and Saskatchewan. There was an overall increase in the dispensing rate in Alberta, but this was driven by the new tamper-resistant formulation.
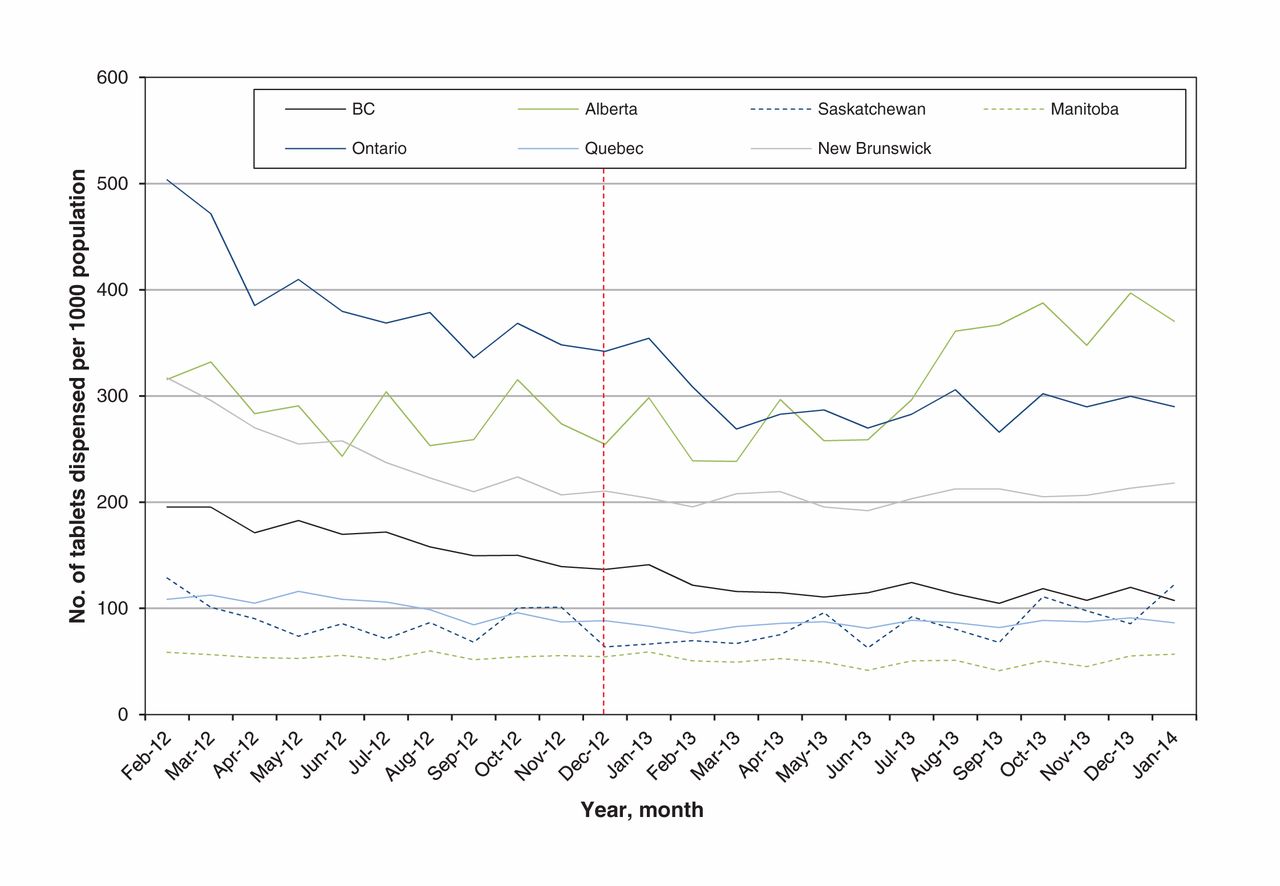
Rate of long-acting oxycodone tablet dispensing (per 1000 population) in regions near Canada–United States border crossings, by province, February 2012 to January 2014. Vertical dashed line indicates point at which generic formulations of the drug became available in Canada.
Between the introduction of the generic formulations in December 2012 and the end of the study period (January 2014), the monthly dispensing rate of long-acting oxycodone near the Canada–US border decreased in British Columbia (21.4%, from 136.7 to 107.4 tablets per 1000 population), Ontario (15.2%, from 342.0 to 289.9 tablets per 1000 population) and Quebec (2.3%, from 88.4 to 86.3 tablets per 1000 population) (Figure 1). In Manitoba and New Brunswick, there were slight increases in the rate of long-acting oxycodone dispensed near the border during this time (4.4% in Manitoba, from 54.5 to 56.8 tablets per 1000 population; 3.6% in New Brunswick, from 210.5 to 218.0 tablets per 1000 population). Both Alberta and Saskatchewan showed substantial relative increases in the rate of long-acting oxycodone dispensed near the border between December 2012 and January 2014 (45.5% increase in Alberta, from 254.5 to 370.4 tablets per 1000 population per month; 92.3% increase in Saskatchewan, from 63.7 to 122.5 tablets per 1000 population per month). However, only 3216 and 125 tablets of non–tamper-deterrent oxycodone were dispensed in the border prescribing regions of Alberta and Saskatchewan, respectively, during this time.
We looked at prescribing patterns for the 50 individual dispensing regions adjacent to the Canada–US border for the type of signal previously seen at pharmacies adjacent to the Detroit–Windsor tunnel,9 and we did not see any substantial fluctuations in the dispensing volume of long-acting oxycodone (Appendix 1). In 10 of the border crossing regions in Ontario, we saw a reduction in the dispensing rate of long-acting oxycodone between December 2012 and January 2014 (range 6.7%–50.0% reduction) (Figure 2). In the Ontario–Ohio (Pelee Island ferry) and the Ontario–Minnesota (Rainy River) border crossing regions, we saw small increases (8.6% and 6.8%, respectively) in the rate of dispensing. The rate in the Ontario–New York (Buffalo Queenston) prescribing region increased by 31.3%, and the rate in the Ontario–Michigan (Detroit–Windsor tunnel) region increased by 48.0%. However, these increases did not occur until July 2013 and October 2013, respectively, and were associated with a small increase in the absolute number of tablets dispensed (monthly mean number of excess tablets was 3135 for Ontario–New York and 3278 for Ontario–Michigan). We detected no substantial fluctuations in monthly prescribing volumes in our analysis of dispensing volumes in larger cities near the Canada–US border (Figure 3). Finally, we found no consistent difference in prescribing trends based on whether the prescribing region bordered an American city identified as a high-intensity drug-trafficking area.14

Rate of long-acting oxycodone tablet dispensing (per 1000 population) in regions near Canada–United States border crossings in Ontario, February 2012 to January 2014. Vertical dashed line indicates point at which generic formulations of the drug became available in Canada. See Appendix 1 (available at www.cmajopen.ca/content/3/2/E231/suppl/DC1) for description of all border crossings contained within each dispensing region

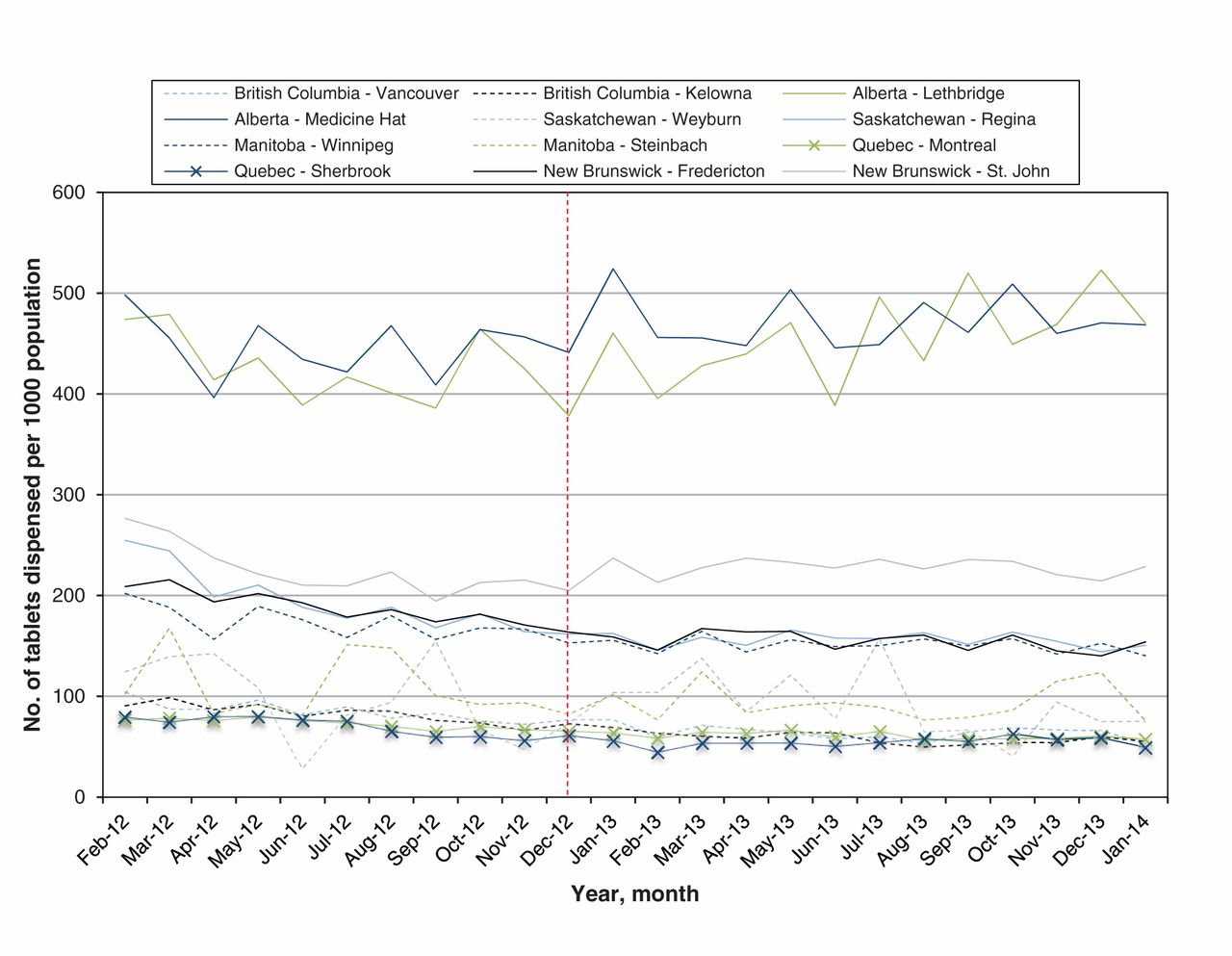
Rate of long-acting oxycodone tablet dispensing (per 1000 population) in cities within 150 km of Canada–US border crossings, February 2012 to January 2014. Vertical dashed line indicates point at which generic formulations of the drug became available in Canada.
Interpretation
In this population-based study involving Canadian retail pharmacies located near the Canada–US border, we found no indication that increased volumes of long-acting oxycodone were dispensed after the introduction of generic non–tamper-resistant formulations in Canada. Our results suggest that, despite the differential availability of these formulations high-volume diversion of these drugs from Canadian retail pharmacies into the US, such as we saw at the Detroit–Windsor tunnel in 2010 and 2011, has not occurred.9 This is likely a reflection of the highly regionalized nature of our past finding, which was quickly rectified after warnings were issued to pharmacists and prescribers. Furthermore, we likely saw no additional increase near the Detroit–Windsor tunnel because the people involved in past trafficking are now aware that their activities are being monitored.
Our findings may be influenced by the slow adoption of generic formulations of long-acting oxycodone in most regions of Canada. Indeed, Quebec is the only province bordering the US in which generic formulations represented a substantial proportion of the long-acting oxycodone market (29%). This high rate of uptake is driven by a public drug plan policy in Quebec that only reimburses patients for the lowest cost generic equivalent of brand name agents when generic versions are available.15 This policy likely encourages patients in Quebec to receive generic long-acting oxycodone owing to the large cost difference between the generic and brand name formulations of the drug. Despite this high rate of dispensing in Quebec, the volume of long-acting oxycodone dispensed near the Quebec–US border crossings did not increase after the introduction of the generic non–tamper-resistant formulations.
Limitations
The methods we employed are likely to detect only geographically concentrated, high-volume diversion of drugs dispensed from Canadian retail pharmacies near Canada–US border crossings. Although this method previously detected such patterns,9 the diversion of small volumes would not be captured. Although the consistency of the findings reinforces the suggestion that large-scale diversion from Canada to the US is not occurring, it does not preclude the possibility of increased dispensing of long-acting oxycodone in localized regions that were not included in our analysis.
We were unable to perform interventional time series analysis because of limitations of data availability before the intervention of interest. In addition, we are unable to obtain data on stolen oxycodone tablets; therefore, this analysis is restricted to describing volumes of long-acting oxycodone legally obtained from Canadian retail pharmacies. Finally, it is possible that the most common drugs of abuse have shifted in the US following the changes in opioid availability. If patients moved to using heroin instead of prescription opioids, the demand for illicitly obtained oxycodone in the US might be affected.
Conclusion
Our population-based analysis of all long-acting oxycodone dispensed in Canadian pharmacies near the Canada–US border found no evidence of behaviour suggestive of large-scale trafficking of generic non–tamper-resistant formulations after their introduction in Canada. However, despite these findings, Canadian clinicians and pharmacists should remain cautious in their prescribing and dispensing of non–tamper-resistant formulations of oxycodone because of the high potential for misuse and abuse of this medication. Furthermore, because high doses of all opioid formulations have been associated with increased fatality rates during regular clinical practice, continued efforts to exercise caution when prescribing these agents should be maintained.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/3/2/E231/suppl/DCI.
Acknowledgments
The authors thank Peter Gozdyra for support in obtaining geographic information for the descriptive analysis and Karen Cauch-Dudek for help identifying the dispensing regions. The statements, findings, conclusions, views and opinions contained and expressed in this publication are based in part on data obtained under licence from IMS Health Canada Inc. concerning the following information service: IMS Brogan Geographic Prescription Monitor database, data period February 2012 to January 2014. All rights reserved. The statements, findings, conclusions, views, and opinions contained and expressed herein are not necessarily those of IMS Health Canada Inc. or any of its affiliated or subsidiary entities. Data sharing: Data are not available for sharing.
Footnotes
Competing interests: Michael Paterson received grants from the Canadian Institutes of Health Research during the conduct of this study. Dr. Gomes reports grants from Ontario Ministry of Health and Long-Term Care, outside the submitted work. No other competing interests were declared.
Contributors: Tara Gomes was involved in the study conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript and final approval of the submitted manuscript. J. Michael Paterson and David Henry were involved in the study conception and design, acquisition and interpretation of data and critical revision of the. Mariam Mukati was involved in study design, analysis of data and critical revision of the manuscript. All of the authors approved the final version to be published and agree to act as guarantors of the work. CNODES investigators: Samy Suissa (principal investigator); Colin Dormuth (British Columbia); Brenda Hemmelgarn (Alberta); Gary Teare (Saskatchewan); Dan Chateau and Patricia Caetano (Manitoba); David Henry and Michael Paterson (Ontario); Jacques LeLorier (Québec); Adrian Levy (Nova Scotia); Pierre Ernst (UK Clinical Practice Research Datalink); Robert Platt (methods); and Ingrid Sketris (knowledge translation).
Funding: This study was supported by the Canadian Network for Observational Drug Effect Studies (CNODES), a collaborating centre of the Drug Safety and Effectiveness Network (DSEN), funded by the Canadian Institutes of Health Research (grant no. DSE-111845).
References
- © 2015, 8872147 Canada Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.