


Abstract
Background Despite their favourable toxicology profile, benzodiazepines and the related Z-drugs (zopiclone, zolpidem and zaleplon) have been associated with physiological tolerance, dependence and addiction. Evidence of harm (e.g., falls, motor vehicle collisions and cognitive disturbances) has been reported in older populations. The aim of this study was to determine the relation between users’ characteristics and the use of benzodiazepines and Z-drugs in Manitoba over a 16-year period.
Methods This time-series analysis was based on prescription data from Apr. 1, 1996, to Mar. 31, 2012, obtained from the Drug Product Information Network database of Manitoba. We obtained sociodemographic information on benzodiazepine and Z-drug users from the Population Registry and determined changes in utilization rates over time using generalized estimating equations.
Results Overall, the prevalence of benzodiazepine use remained stable at about 61.0 per 1000 population between 1996/97 and 2011/12; however, the prevalence of Z-drug use increased steadily from 10.9 to 37.0 per 1000 over the same period. In older people (≥ 65 years), the incidence of benzodiazepine use decreased from 55.5 to 30.3 users per 1000, whereas the incidence of Z-drug use increased from 7.3 to 20.3 users per 1000 over the study period. Among those 18–64 years of age, the incidence of benzodiazepine use decreased from 30.1 to 27.6 users per 1000, but the increase in incidence of Z-drug use was more than 2-fold. The youngest population (≤ 17 years) showed the lowest rates of use of these drugs. The highest rates of use were observed among older women and the low-income population.
Interpretation Over the study period, benzodiazepines have been prescribed less frequently to older patients in Manitoba; however, zopiclone prescribing has continued to increase for all age groups. The reasons for this increase remain to be determined.
Benzodiazepines have been used for decades as effective agents for the treatment of seizure and anxiety disorders and for the short-term control of insomnia. Although their toxicology profile is favourable compared with other hypnotic drugs and sedatives, such as barbiturates, their long-term use has been associated with physiological tolerance, dependence and addiction.1–3 Harm, supported by various levels of evidence, has been widely reported and includes higher risk of falls and fractures,4–6 motor vehicle collisions7 and cognitive disturbances particularly among older people.8 Newer non-benzodiazepine agents (i.e., zopiclone, zolpidem and zaleplon), commonly called Z-drugs, are indicated for sleep disorders. Although it has been suggested that Z-drugs have a lower potential for abuse and dependence,9 their use can also be problematic because of their effects on human performance and driving.10,11
Because of these potential adverse effects, clinical practice guidelines have advised against the use of benzodiazepines and Z-drugs for longer than 4 weeks, and health agencies worldwide have undertaken anti-benzodiazepine and anti-Z-drug campaigns, not without controversy.12–18 However, the dearth of published research studies on this subject suggests that such recommendations have not had a significant impact on the use of benzodiazepines and Z-drugs in various countries.19–22 The only population-based study conducted in Canada was based on data from British Columbia and examined a period of 10 years between 1996 and 2006.20 As there are long delays between the reporting of scientific knowledge and changes in clinical practice, changes in prescribing patterns may have occurred over the last 7 years. Thus, in this study, we describe the prescribing patterns for benzodiazepines and Z-drugs for the entire population of a Canadian province over 16 years by user characteristics.
Methods
Study population
All Manitoba residents registered with the provincial health care system who were prescribed a benzodiazepine or a Z-drug between 1996/97 and 2011/12 were included. No age restrictions were applied, but patients were stratified by sex and age (0–17, 18–64 and ≥ 65 yr). Location of residence (urban v. rural) and socioeconomic status were also assessed. According to validated definitions,23 incident (new) users were defined as people who had not received a prescription for any of the medications of interest in the year before receiving their first prescription, while prevalent users for each fiscal year were defined as people who had received at least 1 prescription for a medication of interest that year.
Data sources
Administrative data on the use of benzodiazepines and Z-drugs between Apr. 1, 1996, and Mar. 31, 2012, were obtained from the Manitoba Population Health Research Data Repository, housed at the Manitoba Centre for Health Policy. Patient records in the repository are de-identified using an encrypted personal health information number as a quasi-identifier to protect privacy. Databases used in this study include the Population Registry, which contains demographic information for all residents of Manitoba, and the Drug Product Information Network, which contains prescription data. The latter includes prescriptions dispensed in Manitoba regardless of the type of insurance coverage (government-sponsored, private or out-of-pocket) and, thus, provides a comprehensive description of non-hospital drug use. Medications administered in hospital and physician samples are not included. Prescriptions dispensed to First Nations patients served by northern nursing stations may by underestimated because of incomplete data entry during the early use of the system. However, the database has been determined to be over 90% accurate in terms of prescriptions dispensed in the community.24
Measures
All benzodiazepines available on the Canadian market during the study were included. Drug identification numbers were retrieved from Health Canada’s drug product database using the codes of the Anatomical Therapeutic Chemical classification system (Box 1). The Z-drugs included in the study were zopiclone and zaleplon; zolpidem was not included as it did not become available on the Canadian market until the end of 2011.
Benzodiazepines and related drugs available in Manitoba over the study period (1996–2012), listed by generic name and Anatomical Therapeutic Chemical code
Alprazolam N05BA12
Bromazepam N05BA08
Chlordiazepoxide N05BA02
Clobazam N05BA09
Clonazepam N03AE01
Diazepam N05BA01
Flurazepam N05BA17
Lorazepam N05BA06
Oxazepam N05BA04
Temazepam N05CD07
Triazolam N05CD05
Zopiclone N05CF01
Zaleplon N05CF03
Population sizes, ranging from 1 144 087 in 1996/97 to 1 261 373 in 2011/12, for use in calculating overall prevalence and incidence, were obtained from the Population Registry as Dec. 31 snapshots for each year. The 3 age groups ranged from 296 658 people in 1996/97 to 291 782 in 2011/12 for those 0–17 years of age, from 692 539 to 793 093 for those 18–64 years of age and from 154 890 to 176 498 for those 65 years of age and older.
Region of residence (rural v. urban) was determined by postal codes registered with Manitoba Health. Socioeconomic status was based on median neighbourhood income quintiles provided by Statistics Canada for the dissemination area in which patients resided: low income included the lowest and second-lowest quintiles, high income included the 3 highest quintiles. People to whom a neighbourhood income could not be assigned (i.e., residents of personal care homes, psychiatric facilities and prisons and wards of the public trustee and Child and Family Services) were grouped into a “not found” category.
Prescriber specialties were derived from the de-identified physician identification number reported on the prescription and classified as general practitioner, psychiatrist or other medical specialty.
Statistical analyses
Separate analyses were conducted to evaluate prevalent and incident use of benzodiazepines and Z-drugs. Generalized estimating equations, which addressed the correlated structure of the data,25,26 were used to analyze incident and prevalent use over time as number of users per 1000 population and to determine the influence of sociodemographic characteristics (age, sex, region of residence and socioeconomic status) on prescribing over the entire study period. For analyses, we used SAS statistical software (v 9.2, SAS Institute, Cary, NC).
Ethics approval
The study was approved by the Health Research Ethics Board of the Faculty of Medicine, University of Manitoba (H2009–024). The study was conducted in full compliance with the Personal Health Information Act of Manitoba, and privacy/confidentiality consent was obtained from the Health Information Privacy Committee of the Government of Manitoba (#2008/2009–48).
Results
Incidence of benzodiazepine and Z-drug use
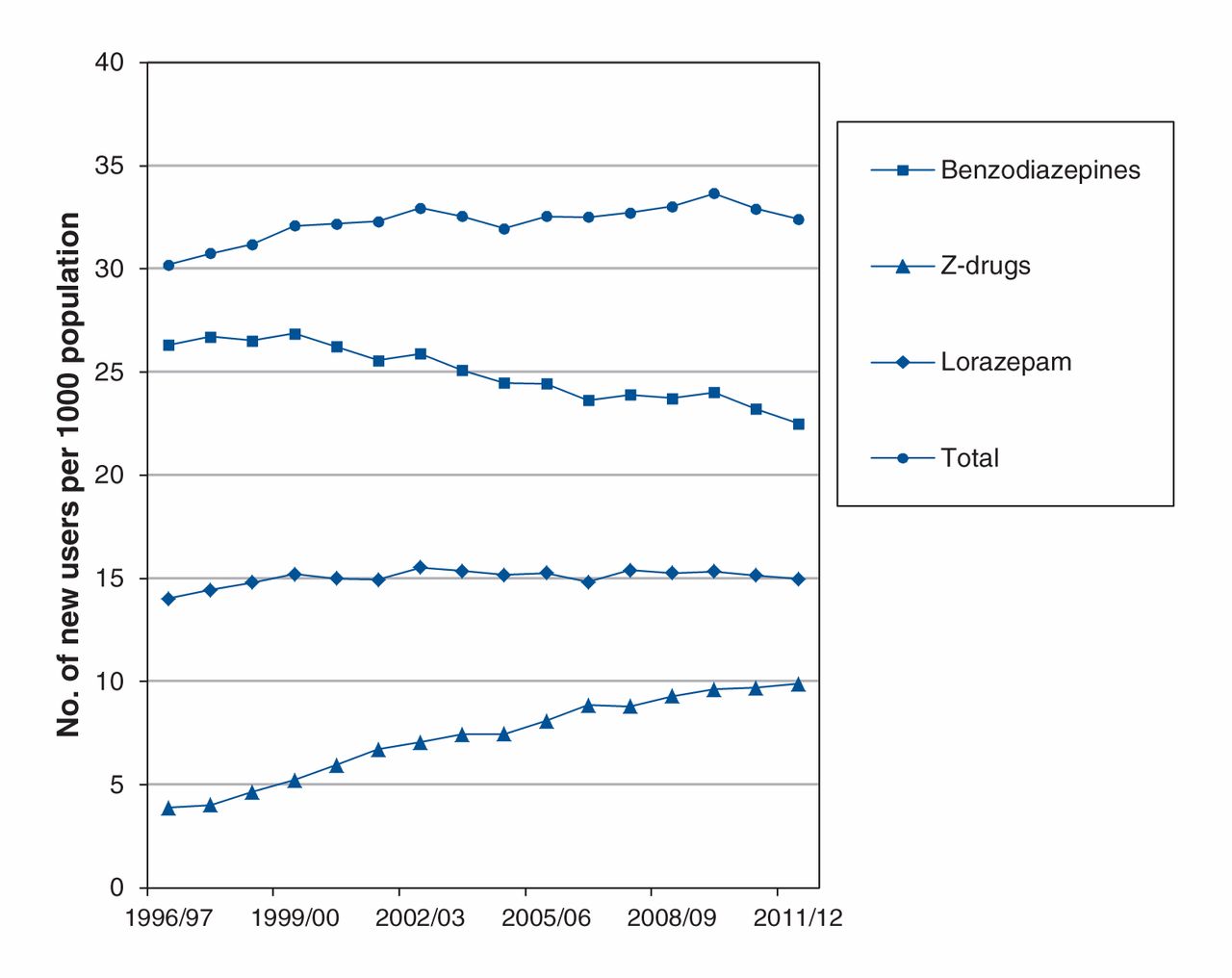
Lorazepam was the benzodiazepine most often prescribed during the study period, with the number of new users remaining fairly stable: from 14.0 per 1000 population in 1996/97 to 15.0 per 1000 in 20011/12 (Figure 1). The incidence of use of other benzodiazepines was lower. Clonazepam was the second-most prescribed benzodiazepine in recent years, with incidence of its use increasing from 1.3 per 1000 in 1996/97 to 2.7 per 1000 in 2011/12. The incidence of diazepam use decreased by more than half between 1996/97 and 2011/12 (from 3.0 to 1.3 per 1000). The incidence of alprazolam and temazepam prescribing also decreased over the same period: from 2.4 to 1.1 per 1000 and from 2.4 to 1.7 per 1000, respectively.

Incidence of benzodiazepine and Z-drug (zopiclone and zaleplon) use in Manitoba, 1996–2012.
The incidence of benzodiazepine use decreased significantly among older adults (≥ 65 yr) from 55.5 per 1000 population in 1996/97 to 30.3 per 1000 in 2011/2012, but use of Z-drugs by this population increased consistently from 7.3 to 20.3 per 1000 over the same period (Figure 2). During the study period, the number of new users of zopiclone in this age group increased by 37 691.
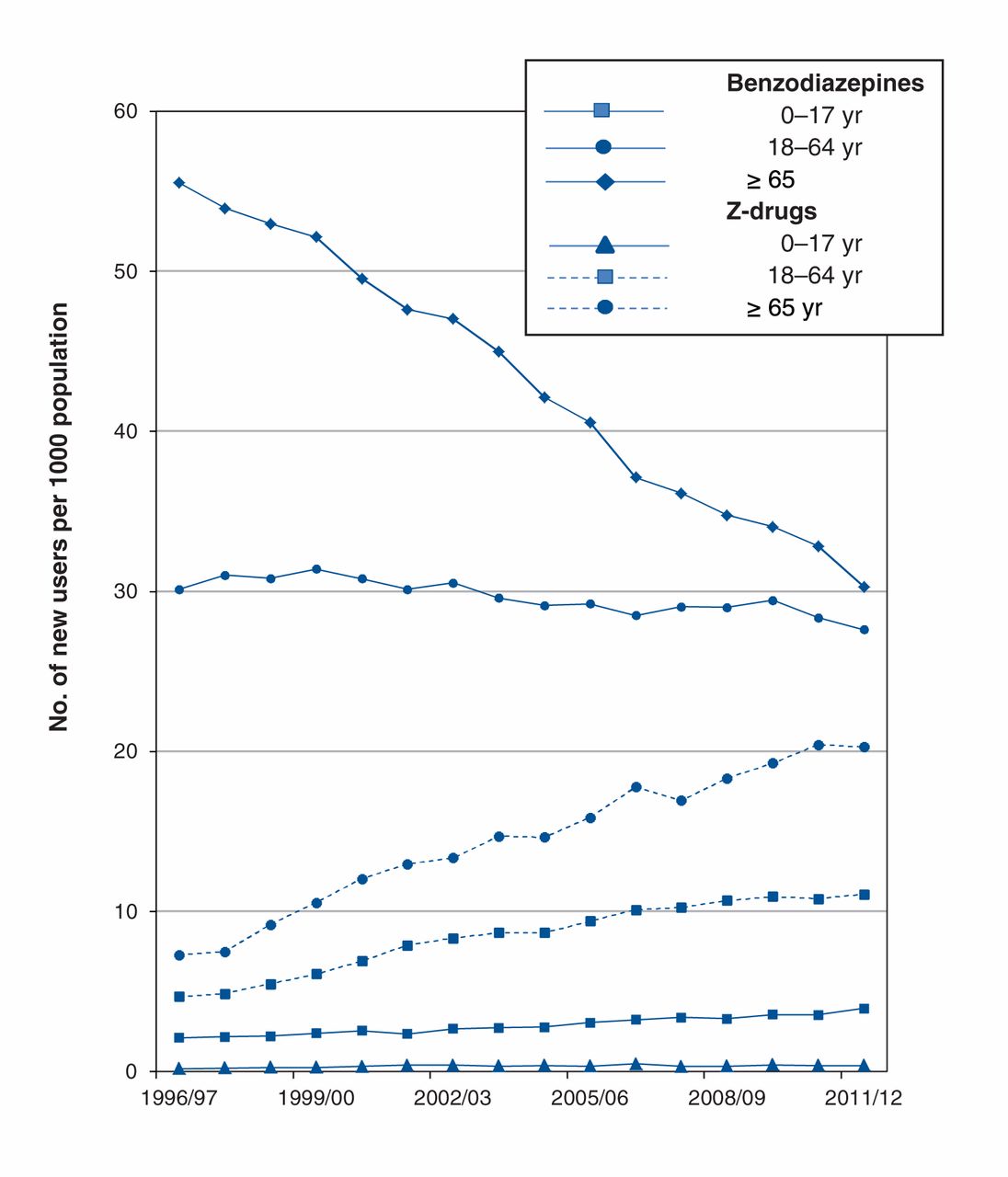
Incidence of benzodiazepine and Z-drug (zopiclone and zaleplon) use by age group in Manitoba, 1996–2012.
The adult population between 18 and 64 years of age showed a slight decrease in incidence of benzodiazepine use, from 30.1 to 27.6 per 1000 population, but the increase in incidence of Z-drug use was more than 2-fold: from 4.7 per 1000 in 1996/97 to 11.1 per 1000 in 2011/12 (Figure 2). The number of new users of zopiclone and zaleplon in the 18–64 age group increased by 99 361 over the study period.
The youngest segment of the population (0–17 yr) showed the lowest overall incidence of benzodiazepine and Z-drug use, with only 1589 new users over the study period; however, among this population, the incidence of use of both classes of drugs increased significantly: from 2.20 per 1000 in 1996/97 to 3.95 per 1000 in 2011/12 for benzodiazepines; and from 0.19 to 0.39 per 1000 for Z-drugs over the same time period (Figure 2).
Prevalence of benzodiazepine and Z-drug use
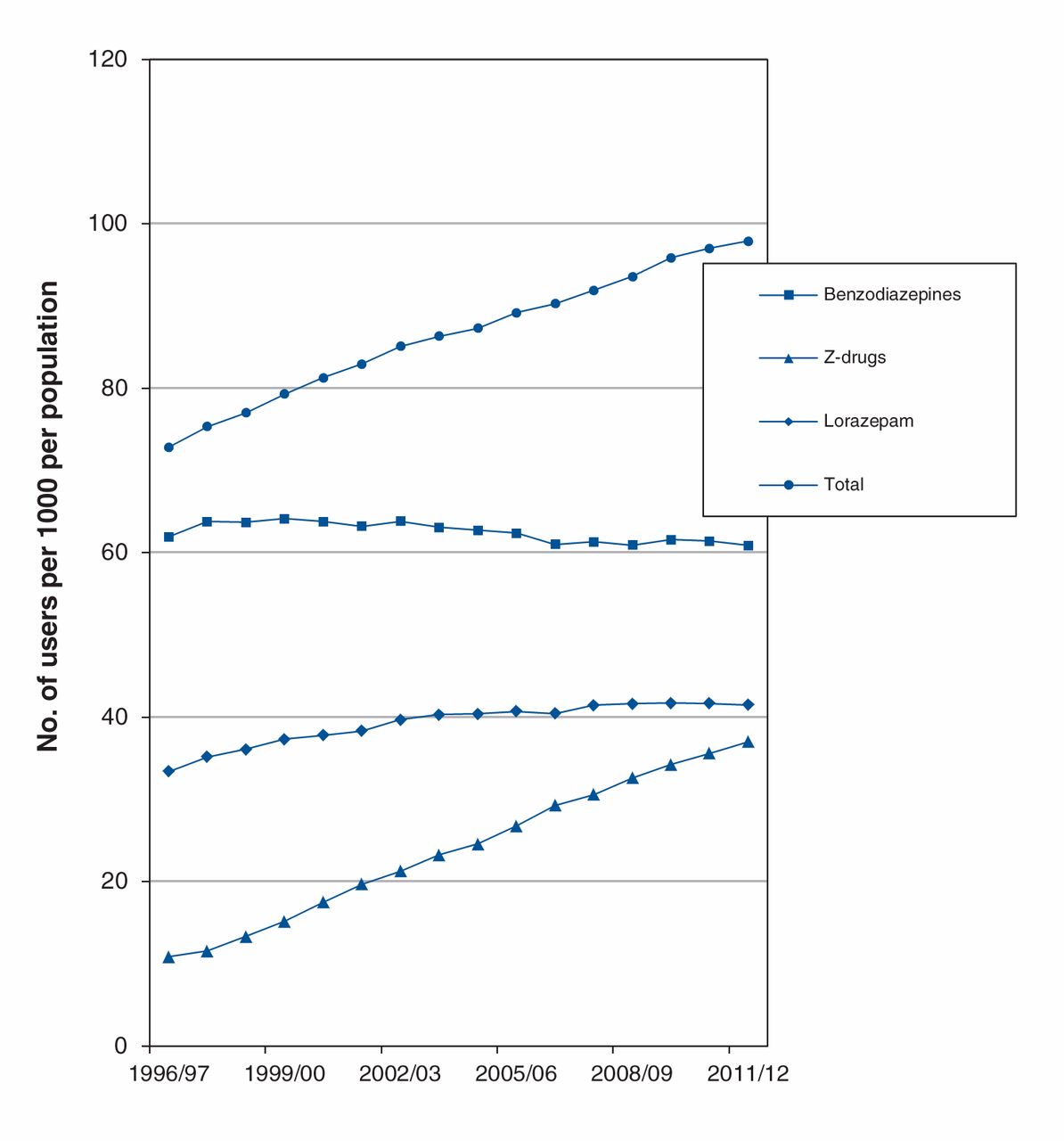
Over the study period, the prevalence of lorazepam use increased from 33.4 to 41.5 per 1000 population (Figure 3). For clonazepam, prevalence increased from 5.6 per 1000 population in 1996/97 to 15.8 per 1000 in 2011/12 The prevalence of temazepam use also increased from 8.1 per 1000 in 1996/97 to 12.0 per 1000 in 2011/12. In contrast, the prevalence of diazepam use showed a significant decrease from 10.5 to 5.8 per 1000 over the study period. Alprazolam prevalence remained stable at approximately 7.0 per 1000.
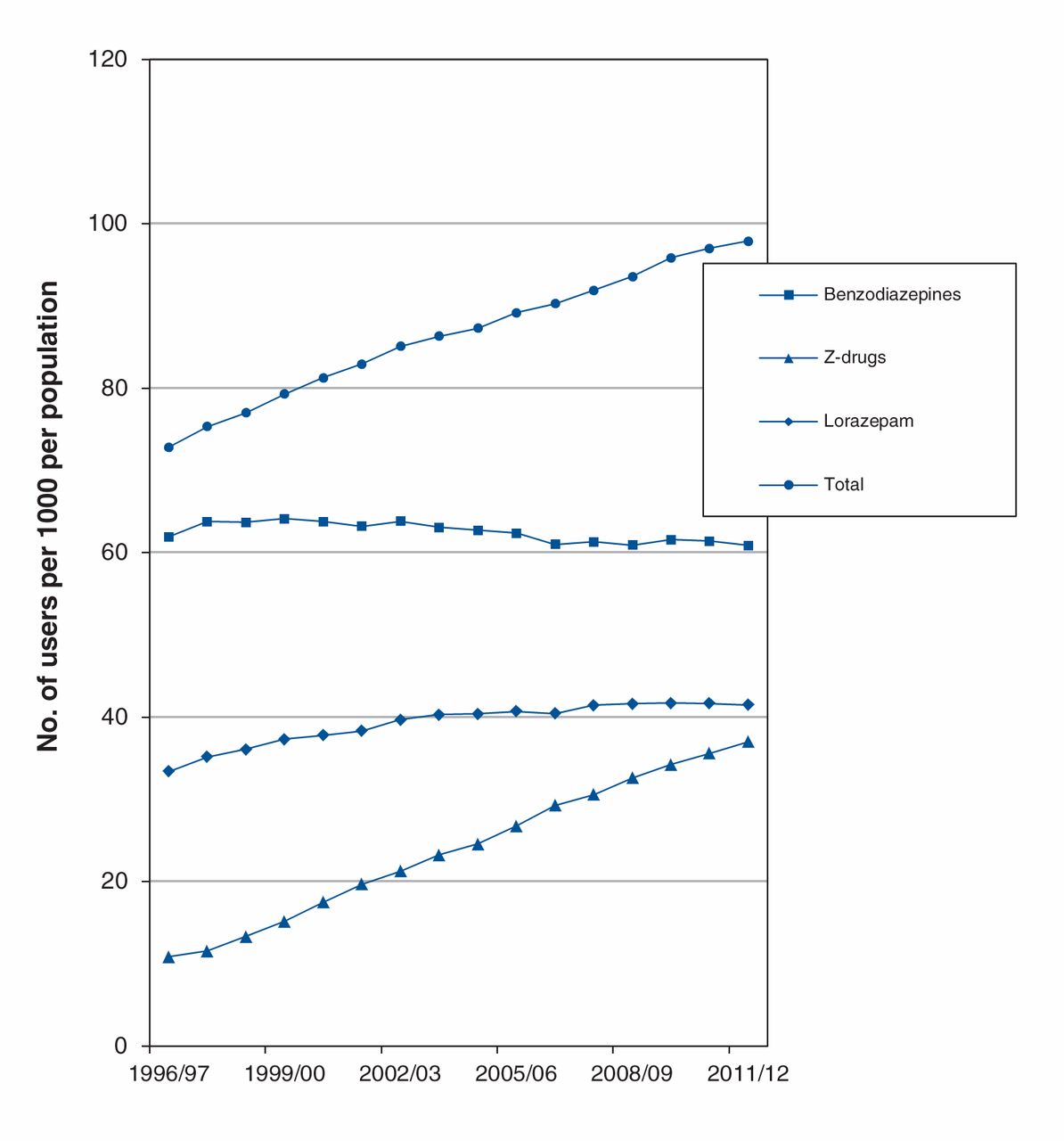
Prevalence of benzodiazepine and Z-drug (zopiclone and zaleplon) use in Manitoba, 1996–2012.
Stratification by age group (Figure 4) showed that, since 2005/06, the prevalence of both benzodiazepine and Z-drug use was highest among the oldest population group: benzodiazepine prevalence among this group decreased from 174.7 to 120.6 per 1000 over the study period, but Z-drug use increased steadily from 25.2 to 93.9 per 1000 in the same period.
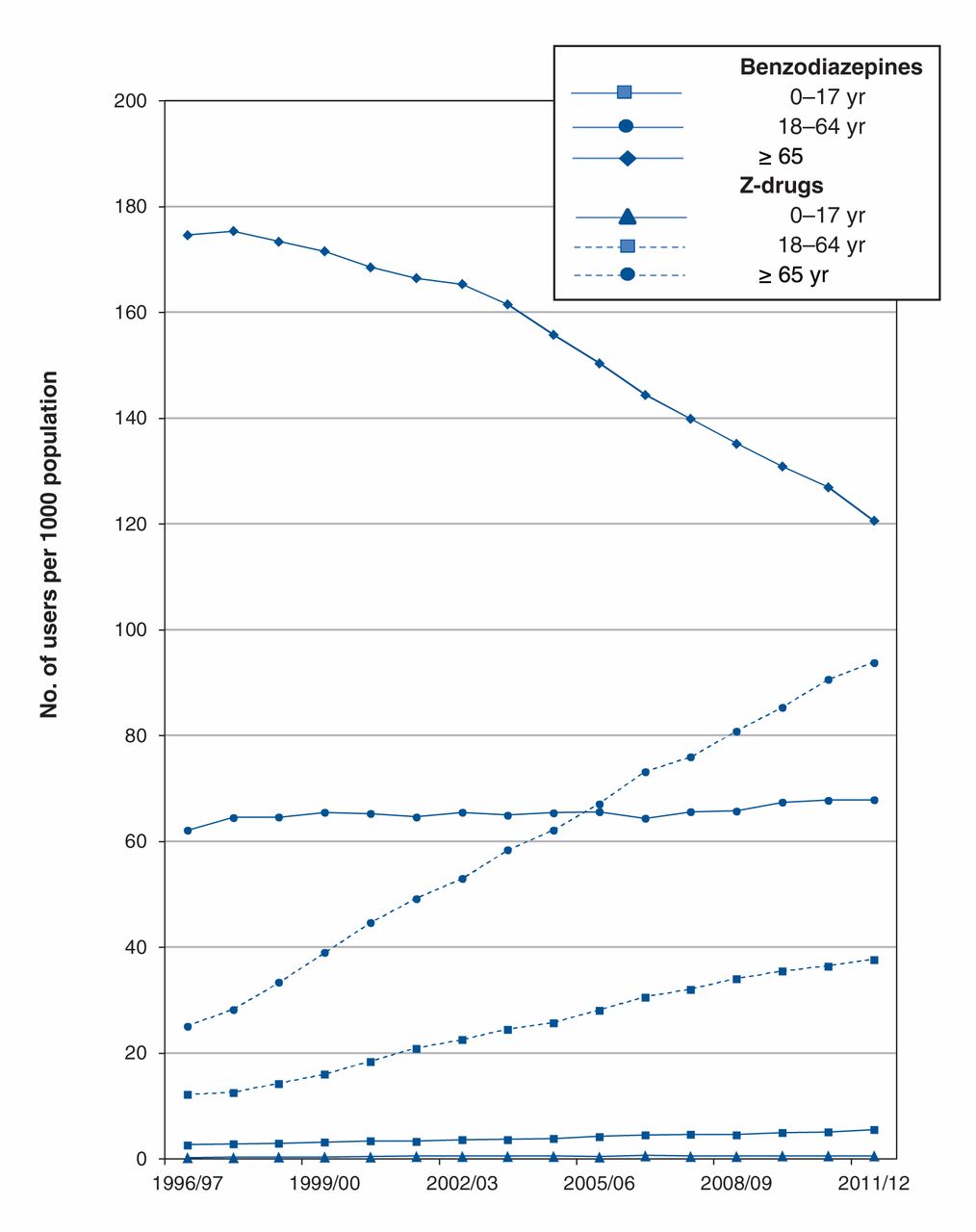
Prevalence of benzodiazepine and Z-drug (zopiclone and zaleplon) use by age group in Manitoba, 1996–2012.
In the other 2 age groups, prevalence of benzodiazepine use increased from 62.1 to 67.9 per 1000 among the 18–64 year olds and from 2.7 to 5.6 per 1000 among the 0–17 year olds. For the Z-drugs, prevalence increased from 12.2 to 37.8 per 1000 and from 0.29 to 0.62 per 1000 among the 18–64 and the 0–17 age groups, respectively (Figure 4).
Effects of sex, place of residence and socioeconomic status
Stratification by sex showed that the incidence of both benzodiazepine and Z-drug use was higher among females than males over the study period. The incidence of benzodiazepine use decreased slightly among females from 33.2 to 28.3 per 1000, compared with a decrease from 19.2 to 17.3 per 1000 among males. The incidence of Z-drug use among females increased from 4.6 to 11.8 per 1000; among males, the increase was from 3.2 to 8.0 per 1000. These changes were significant (Table 1).
Region of residence did not have a significant effect on incidence of use. High socioeconomic status was associated with a higher incidence of Z-drug use.
The prevalence of benzodiazepine use among males was 42.7 per 1000 in 1996/97 and 44.4 per 1000 in 2011/12; among females, the prevalence was 80.1 per 1000 in 1996/97 and 77.0 in 2011/12. The prevalence of Z-drug use increased significantly from 13.4 to 47.4 per 1000 among females and from 8.3 to 26.4 per 1000 among males (Table 2).
Urban place of residence was associated with a higher prevalence of benzodiazepine use. High socioeconomic status was associated with a higher prevalence of Z-drug use, but a lower prevalence of benzodiazepine use (Table 2).
Prescriptions
In 2011/12, more than 1 million prescriptions for benzodiazepines and Z-drugs were dispensed in Manitoba. In 1996/97, a total of 379 259 prescriptions were for benzodiazepines alone and 44 020 were for Z-drugs. By 2011/12, the number of prescriptions for benzodiazepines and Z-drugs had increased to 726 409 and 277 811, respectively. Lorazepam was the benzodiazepine most often prescribed; it accounted for more than a third of all benzodiazepine prescriptions. Each year, general practitioners wrote more than 80% of all prescriptions for these drugs and psychiatrists wrote approximately 15%; the remainder were written by physicians of other medical specialties.
Interpretation
Substantial changes in prescription patterns were observed in Manitoba over the study period. Over time, fewer patients were started on a benzodiazepine, although the prevalence of use was not significantly affected but remained relatively stable in the adult population (18–64 yr). This suggests that patients were probably staying on medications longer than recommended.
Our analyses differentiated between benzodiazepines and the Z-drugs, zopiclone and zaleplon, which are not chemically related to benzodiazepines but share similar pharmacologic activity with respect to the γ-aminobutyric acid (GABA) type A receptor. Z-drugs have been marketed as hypnotic medications superior to benzodiazepines mainly because of their favourable pharmacokinetic and safety profiles despite the lack of evidence of substantial clinical advantages over appropriate doses of shorter-acting benzodiazepines.27
Other international studies have shown an increase in Z-drug use over time while benzodiazepine use decreased, especially among people over 65 years of age.28–31 In Canada, prescribing of benzodiazepines and Z-drugs in British Columbia decreased slightly from 1996 to 2006 in older people, but increased in younger segments of the population (females and people with low income).20 To set our results in the context of other reports and to assess use of these drugs in the oldest and youngest groups, we stratified our population into 3 age groups.
We observed sex differences in our study: both prevalence and incidence of benzodiazepine and Z-drug use were consistently higher among women, especially older women. Although this finding is not unique to the Canadian context, studies in other countries, where insurance coverage of short-acting benzodiazepines and Z-drugs is restricted, have reported that male patients were more likely to receive benzodiazepines than female patients.30 Place of residence did not seem to have a substantial effect on incidence, but low income was associated with greater use of benzodiazepines than Z-drugs. The higher rates of mental disorders among women and lower socioeconomic status groups may explain this finding.32 Government-sponsored drug programs have covered these drugs as unrestricted benefits; therefore, no segment of the population could have experienced access limitations.
Limitations
Our study has some recognized limitations. Administrative data do not provide information on clinical benefits. Medication use in hospitals is not captured, although information on nonhospital use is comprehensive. The prescription database does not include information on diagnoses and comorbidities; however, Z-drugs are indicated specifically for the treatment of insomnia, and it has been suggested that some physicians still perceive that they are safer and more effective than benzodiazepines for this condition.33 Therefore, it could be inferred that insomnia might be the most prevalent diagnosis affected by a switch from a benzodiazepine to a Z-drug. It is important to note that zaleplon was discontinued in 2007 and that its use in Manitoba has been generally low: prevalence was below 1.0 per 1000 between 2001/02 and 2007/08, and incidence approached 0.1 per 1000 in 2005/06. Thus, zopiclone alone accounts for the rapid increase in the use of Z-drugs. As we collected no information on daily doses, duration of use or co-medications, no conclusions on appropriateness of prescribing can be derived from this study. Finally, prescription databases are only records of dispensations and not of medication consumption.
Our study was not designed to assess the impact of specific warnings or interventions aimed at improving prescribing habits; however, it appears that physicians in Manitoba have been concerned about the potential harm of prescribing benzodiazepines to their older patients, as has been the case for other psychotropic medications,34 and have responded by starting fewer and fewer older people on a benzodiazepine. The rise in zopiclone prescribing, however, remains a reason for concern.
Patients of all ages seem to remain on a benzodiazepine or zopiclone for extended periods and might experience difficulties in discontinuing treatment. It is important to explore interventions35,36 that can help patients discontinue use of benzodiazepines and Z-drugs when they are no longer needed.
Conclusion
Although it appears that, over time, benzodiazepines have been prescribed less frequently to older patients in Manitoba, zopiclone prescribing has continued to rise among all age groups. It remains to be investigated whether the decline in benzodiazepine use is limited to the diagnosis of insomnia or whether other medications have replaced benzodiazepine for conditions such as anxiety.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/2/4/E208/suppl/DC1
Acknowledgements
: The authors acknowledge the Manitoba Centre for Health Policy, University of Manitoba, for use of data contained in the Population Health Research Data Repository under project #2009-020, and derived from data provided by Manitoba Health. The results and conclusions are those of the authors and no official endorsement by Manitoba Health, the Manitoba Centre for Health Policy or other data providers is intended or should be inferred.
Footnotes
-
Competing interests: None declared.
-
Contributors: Silvia Alessi-Severini and James M. Bolton contributed equally to this project. All authors contributed to the design and interpretation of the study. Silvia Alessi-Severini wrote the paper, Matthew Dahl conducted the analyses. All authors contributed to the writing and approved the final version. All of the authors agree to act as guarantors for this work.
-
Funding: Preparation of this article was supported by an operating grant from the Health Sciences Centre Foundation (James Bolton and Silvia Alessi-Severini). Additional investigator support includes the following salary awards: a Manitoba Health Research Council Establishment Award (James Bolton), a Manitoba Health Research Council Chair Award (Jitender Sareen) and a Canadian Institutes of Health Research New Investigator Award (#152348, Jitender Sareen).
References
- © 2014 Canadian Medical Association or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





