


Abstract
Introduction Recent epidemiologic studies have suggested that the incidence of noncervical cancers associated with human papillomavirus (HPV) is increasing. We assessed temporal, age-specific and sex-specific changes in the incidence of HPV-associated cancers in a population-based study.
Methods We used the Alberta Cancer Registry, a registry of all cancers diagnosed in the province of Alberta, Canada, to identify patients with cancers of the oropharynx, cervix, vulva, vagina, anus and penis (cancers associated with HPV) between Jan. 1, 1975, and Dec. 31, 2009. We estimated the age-standardized incidence of each cancer by sex- and age-specific group and assessed the annual percentage change using joinpoint regression.
Results The age-standardized incidence of oropharyngeal cancers increased for each 5-year interval of the study period among men (annual percentage change 3.4, p < 0.001) and women (annual percentage change 1.5, p = 0.009). For anal cancers, the age-standardized rates increased among women (annual percentage change 2.2, p < 0.001) and men (annual percentage change 1.8, p = 0.008). The age-standardized incidence of cervical cancer increased with age, reaching an annual percentage change of –3.5 among women aged 75–84 years (p = 0.04). The rates of other HPV-associated cancers (vulvar, vaginal and penile) showed little change.
Interpretation Our findings showed increases in the incidence of the HPV-associated cancers of the oropharynx and anus among men and women, and increases in cervical cancer among younger women. The incidence of HPV-related cancers in younger age groups should continue to be monitored. Programs to prevent HPV infection, such as vaccination, should be considered for males as well as females.
According to world-wide estimates, human papillomavirus (HPV) infection is responsible for 5.2% of all cancers.1,2 The association between HPV and cervical cancer has been well-known for many decades, but the link between HPV and cancers of the anus, penis, vagina, vulva and oropharynx has only recently been confirmed.3 Cervical cancer rates have been declining in Canada and the United States, consistent with the successful adoption of Papanicolaou smear screening programs,4,5 but the incidence of other HPV-related cancers has been increasing. The increasing incidence of these HPV-related cancers has been attributed to changes in lifestyle-related risk factors, most notably sexual behaviour.5 Analysis of trends in incidence and birth cohorts in both the US and the United Kingdom have shown an increased risk of HPV-related cancer in more recent birth cohorts and recent time periods,5,6 and these increases have been attributed to generational changes in sexual patterns and increased exposure to HPV.6
HPV vaccines are now broadly used in the prevention of cervical cancer. In Alberta, HPV vaccination programs were implemented in 2008 and, as in many other jurisdictions, have been funded only for females. Although HPV vaccination programs may reduce the incidence of HPV-related cancers other than cervical cancer,6 they remain the subject of much public policy debate in Canada.7 In this study, we sought to examine trends in noncervical HPV-related cancers over time and compare them with relative changes in cervical cancer and non–HPV-related cancers with similar risk factors.
Methods
Patient population
We defined HPV-associated cancers as those for which there is evidence to support their association with HPV.3 We identified cancers diagnosed between Jan. 1, 1975, and Dec. 31, 2009, from the Alberta Cancer Registry using the following International Classification of Diseases for Oncology, 3rd Revision (ICD-O-3) codes for the HPV-associated group: cancers of the anus (C20–C21), cervix (C53), oropharynx (C019, C024, C028, C090–C099, C102, C108, C140, C142 and C148), vulva (C51), vagina (C52) and penis (C60). The Alberta Cancer Registry is an accredited registry with population-based coverage since the 1950s. It currently covers a population of 3.6 million and has achieved the highest level for complete, accurate and timely incidence data as recognized by the North American Association of Central Cancer Registries.8 For a comparison of trends in incidence, we identified a group of non–HPV-associated, modifiable-risk cancers that were diagnosed over the same period from the Alberta Cancer Registry: cancers of the lip, oral cavity and pharynx (C00.0–C0.69, C07.9–C10.9), lung (C33, C34), endometrium (C54), ovary (C56) and colon (C18, C19).
All tumours diagnosed since 2007 were coded according to the ICD-O-3; for those diagnosed in earlier years, we converted the codes to ICD-O-3 codes. Age at diagnosis was categorized by 10-year age group (< 35, 35–44, 45–54, 55–64, 65–74, 75–84), and year of diagnosis was assigned to a 5-year period (1975–1979, 1980–1984, 1985–1989, 1990–1994, 1995–1999, 2000–2004, 2005–2009). Because of the small number of cases of cancers of the anus, oropharynx and vagina among patients younger than 35 years, for these cancers, the youngest group was defined as age less than 45 years. Because of the small number of cancers of the lip, oral cavity and pharynx, trends for these were estimated over time for all ages. Patients aged 85 or older were excluded because of the small number of cases.
Statistical analysis
We calculated age-standardized and age-specific rates (per 100 000 population with 95% confidence intervals [CI]) by sex and cancer type for each 5-year period of diagnosis from 1975 to 2009. Rates were age-standardized to the 1991 Canadian cancer population. We identified trends in age-standardized and age-specific rates over time, and changes in these trends, using joinpoint regression. Joinpoint uses a regression model to describe trends by a sequence of trend lines, or annual percentage change, and to identify points where any significant changes in trends occur. We modelled trends using the Monte Carlo permutation method to select the optimum number of points at which incidence trends changed (either in direction or magnitude).9 The maximum number of joinpoints was limited to 5 as recommended.9 To assess trends by age group where incidence was low, we analyzed 5-year periods, thereby estimating the percentage change between periods. Findings were described as significant if the p value was less than 0.05. Analyses were conducted with SAS software (version 9.1; SAS Institute Inc.) and the Joinpoint Regression Program (version 4.0.4; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute).
Ethics approval
This retrospective study was reviewed and approved by the Alberta Cancer Research Ethics Committee, Alberta Health Services.
Results
Between 1975 and 2009, 8120 HPV-associated cancers were diagnosed in Alberta. Most were cervical cancer (56.1%) and oropharyngeal cancer (17.9%) (Table 1). The HPV-related cancers were generally diagnosed at a younger age than the non–HPV-associated cancers (lung, endometrium, ovary and colon) (Table 2). Cervical cancer was diagnosed at the youngest age (mean 47.0 years, 95% CI 46.5–47.5), followed by oropharyngeal (mean 60.1 years, 95% CI 59.4–60.6), ovarian (mean 60.3 years, 95% CI 58.5–61.4) and anal cancer (mean 62 years, 95% CI 61.2–63.3).
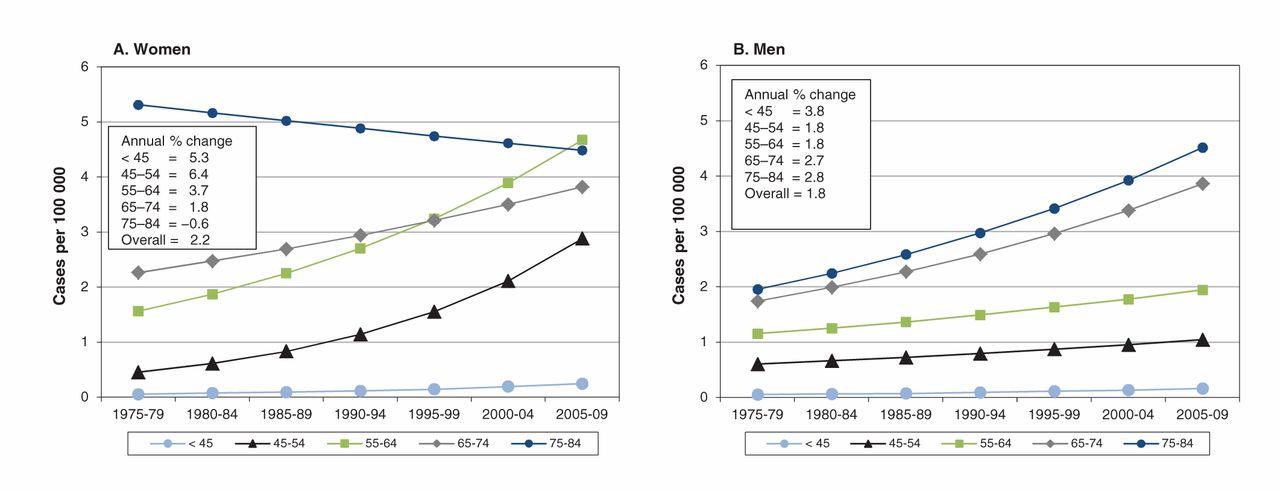
Significant increases in the incidence of HPV-associated cancers of the anus, oropharynx and vulva, and of non–HPV-associated cancer of the lung among women, were noted between 1975 and 2009. The age-standardized incidence of anal cancer among women doubled between 1975 and 2009, from 0.7 (95% CI 0.5–0.9) per 100 000 to 1.5 (95% CI 1.1–1.9) per 100 000; the annual percentage change was 2.2 (p < 0.001) (Appendix 1e). The increase in incidence per 5-year interval of anal cancers among women was highest among those less than 45 years (annual percentage change 5.3, p = 0.014) and those 45–54 years (annual percentage change 6.4, p = 0.011) and decreased with advancing age (Figure 1A). The age-standardized incidence of anal cancer among men increased from 0.5 (95% CI 0.4–0.6) per 100 000 in 1975 to 0.9 (95% CI 0.8–1.0) per 100 000 in 2009, with an annual percentage change of 1.8 (p = 0.008) (Appendix 1e). Among men, the incidence per 5-year interval increased in all age groups, with the annual percentage change ranging from 1.8 in the 45–54 and 55–64 age groups to 3.8 among those less than 45 at diagnosis (Figure 1B).
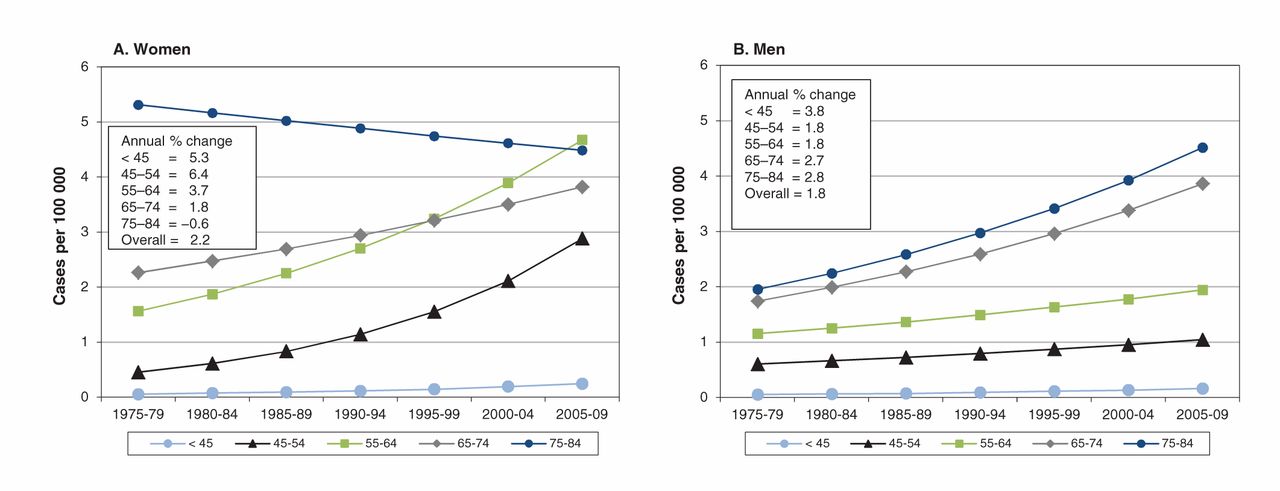
Age-specific trends in incidence of anal cancers in Alberta, Canada, 1975–2009, among women (A) and men (B).
For oropharyngeal cancer, the increase in incidence per 5-year interval among men (annual percentage change 3.4, p < 0.001) was double that among women (annual percentage change 1.5, p = 0.009) between 1975 and 2009 (Appendix 1f). The age-standardized incidence of oropharyngeal cancer increased from 1.2 (95% CI 1.1–1.3) to 3.7 (95% CI 3.5–3.9) per 100 000 among men, as compared with an increase from 0.6 (95% CI 0.5–0.7) to 1.0 (95% CI 0.9–1.1) per 100 000 among women. For women, the incidence increased with advancing age, from 0.01 (95% CI 0.0–0.1) per 100 000 among those less than 45 years to 3.3 (95% CI 2.9–3.7) per 100 000 among those aged 65–74 years and 2.6 (95% CI 2.3–2.9) per 100 000 among those aged 75–84. The same was true for the rise in incidence per 5-year interval (annual percentage change −1.7 among those < 45 yr to 1.9 among those 75–85 yr; test for increase in age, p = 0.11), although this was not significant (Figure 2A). The incidence per 5-year interval for oropharyngeal cancer among men decreased with advancing age (annual percentage change 6.9 among those 35–44 yr to 1.5 among those 75–84 yr); this was also not statistically significant (p = 0.23) (Figure 2B).
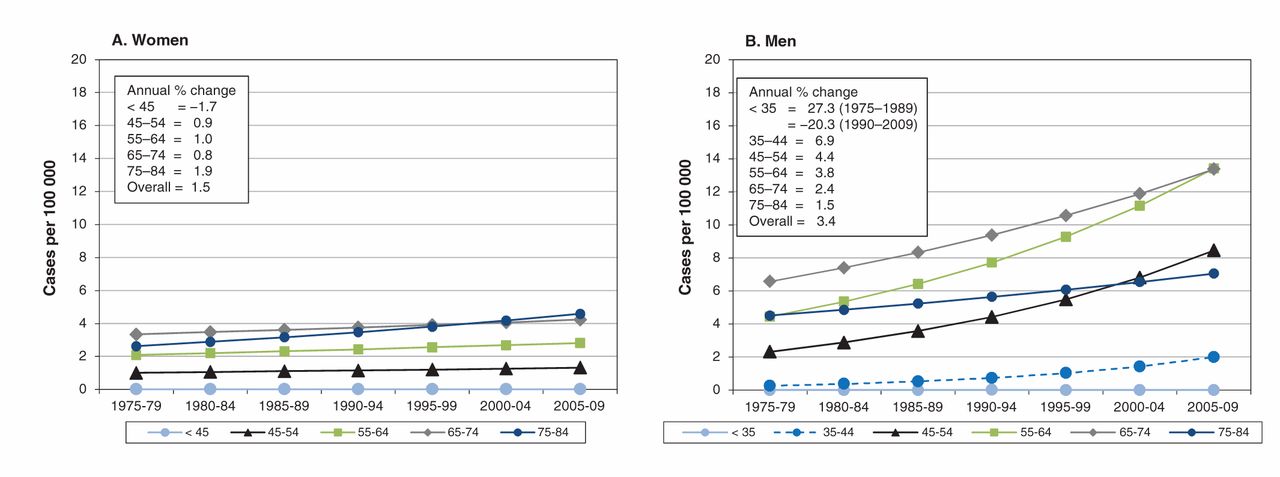
Age-specific trends in incidence of oropharyngeal cancers in Alberta, Canada, 1975–2009, among women (A) and men (B).
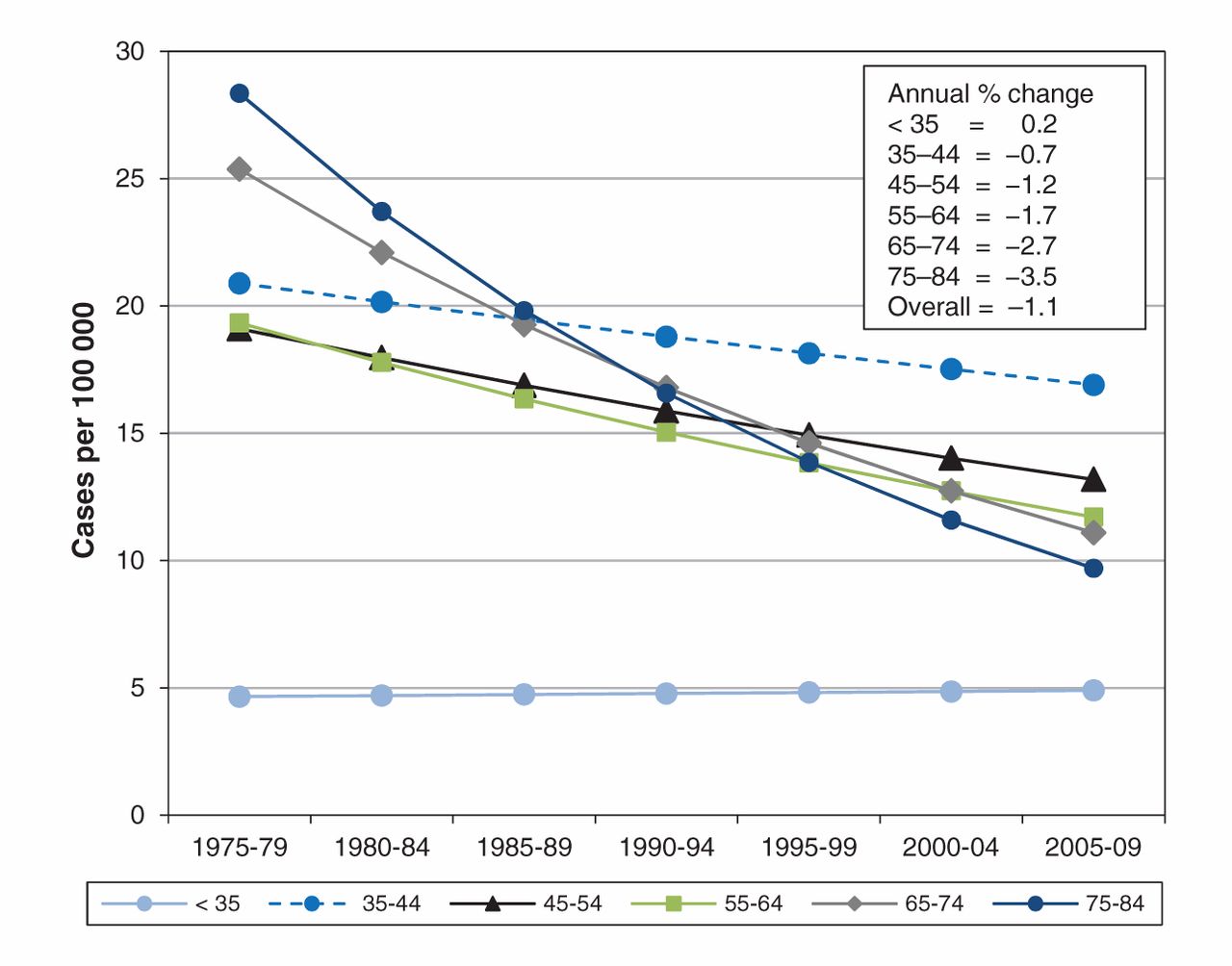
There was little change in the incidence over time of HPV-associated cancers of the vulva, vagina and penis (Appendix 1a). The increase in age-standardized incidence of vulvar cancer was small (annual percentage change 0.07, p = 0.043) (Appendix 1a). In comparison, the age-standardized incidence of cervical cancer declined over this period (annual percentage change –1.1, p < 0.001) (Appendix 1g). The decline in cervical cancer incidence increased with age, reaching an annual percentage change of –3.5 among women aged 75–84 (test for trend: p < 0.001) (Figure 3).

Age-specific trends in incidence of cervical cancers in Alberta, Canada, 1975–2009.
In comparison, among non–HPV-related cancers, the age-standardized incidence of cancers of the lip and oral cavity was stable among men and women (Appendix 1h). The age-standardized incidence of lung cancer among men decreased after 1987 (annual percentage change –1.5, p < 0.001), but among women, it continued to increase, from 13.4 (95% CI 13.2–13.6) per 100 000 in 1975 to 47.3 (95% CI 46.6–48.0) per 100 000 in 2009 (Appendix 1b). There was little change in the age-standardized incidence of endometrial cancer since 1980 (annual percentage change 0.2, p = 0.40). The incidence of ovarian cancer was stable until 1994 (annual percentage change 0.4, p = 0.43), after which it decreased (annual percentage change –3.5, p = 0.04) (Appendix 1c). The age-standardized incidence of colon cancer among women consistently decreased, from 30 (95% CI 29.5–30.5) per 100 000 to 26 (95% CI 25.5–26.5) per 100 000 (p < 0.001). Among men, the incidence of colon cancer increased between 1975 and 1997 (annual percentage change 1.0, p < 0.001) and was stable between 1997 and 2008 (annual percentage change –0.8, p = 0.54) (Appendix 1d).
For numbers of cases by cancer type, 5-year period, age group and sex, see Appendix 2.
Interpretation
We observed an increase in the incidence of noncervical, HPV-related cancers in Alberta from 1975 to 2009, specifically cancers of the anus and oropharynx. Although not statistically significant, the greater increases in oropharyngeal cancer among younger men and in anal cancer among younger women warrant monitoring or further investigation to determine whether these trends continue or increase. There was little change in incidence over time for other HPV-associated cancers (vulvar, vaginal and penile). In comparison, the age-standardized incidence of cervical cancer declined over the study period, as anticipated because of established screening programs. The incidence of non–HPV-related cancers (lung, endometrial, ovarian and colon) decreased in the latter years of the study, except for lung cancer among women, which continued to increase, reflecting historic smoking patterns.
Similar trends in the incidence of HPV-associated cancers have been reported elsewhere in Canada and other regions in the world. Recent studies evaluating oropharyngeal cancer have suggested that, in contrast to head and neck cancers, which are associated with tobacco and alcohol use, the incidence of HPV-associated cancers is on the rise,10–14 although incidence varies by country, ethnicity or race, and sex.14,15 Data from the Canadian Cancer Registry show that the age-standardized incidence of HPV-associated oropharyngeal cancer increased from 1.6 per 100 000 in 1992 to 2.6 per 100 000 in 2009.16 A recent study from British Columbia mirrors the overall Canadian trends.17 We observed that the increase in incidence of oropharyngeal cancer among men was twice that among women (annual percentage change 3.4 v. 1.5) between 1975 and 2009. Similarly, both Canadian16 and US18 data show that the increased incidence of HPV-associated head and neck cancers was greater among men, most notably the younger groups. In 2 previously reported Canadian studies,16,17 ethnic minorities appeared to be at higher risk than the general population of both oropharyngeal cancer and oral cavity cancers. In the US, non-Hispanic white and Hispanic populations experienced greater increases in the incidence of HPV-associated head and neck cancers than other groups.18 It is unclear whether racial and ethnic variations reflect differences in oncogenic HPV infection or other risk factors. Because ethnicity was not consistently available in our registry data, we were unable to determine whether there were any potential differences in HPV-related cancer incidence by ethnic group in Alberta.
For anal cancer, studies from the US,19 Australia20 and several European countries12,21–23 have reported an increase in incidence over time. As was also observed in our study, the incidence of anal cancer in most countries is higher among women than among men. Among the other HPV-related cancers we examined (vulvar, vaginal and penile), we noted a significant increase only in the incidence of vulvar cancer, but the change was small. We observed little change in the incidence over time of vaginal and penile cancers, although the rarity of these tumours limits the ability to distinguish small differences. Reports of increasing incidence of vulvar, vaginal and penile cancers have been observed in some parts of the world. In both Denmark24 and the Netherlands,25 the incidence of penile squamous cell carcinomas has been increasing. Similarly, in the US, the incidence of invasive vulvar carcinoma increased 1.0% per year between 1973 and 2004.26 As with other HPV-associated cancers, the rates of invasive vaginal, vulvar, penile and anal carcinomas have all been reported to vary by race and ethnicity.27–29
Strengths and limitations
Strengths of this study include the evaluation of all known HPV-associated cancers in a comparative analysis of data from a single centralized cancer registry over 4 decades. The quality of the Alberta Cancer Registry data is known to be high but may be affected by incorrect or incomplete data or changes in identification because of the use of new diagnostic techniques over time. In addition, data were collected retrospectively from the registry without corroborating chart reviews. Therefore, the potential for miscoding remains, as has been described in relation to registry data.
A weakness of this study is the inability to confirm histologically the definitive HPV status in tumours. Although we included tumour sites with known HPV-association, we may have over- or underestimated the incidence of true HPV-associated cancers.
Other important risk factors, such as smoking, may influence the incidence of various cancers. However, the decreasing incidence of most tobacco-related cancers over the same study period suggests that changes related to smoking are unlikely to account for the rising trends we observed in cancers of the anus and oropharynx. Past behavioural changes, which may be influenced by demographic fluctuations, may also influence exposure to risk factors and the current incidence of various cancers. Our study was not aimed at assessing behavioural changes, nor did we attempt to explore potential underlying causes of the observed rise in incidence of HPV-associated cancers. Certainly, the observation that HPV-associated cancers are on the rise raises the need for more study of behavioural changes that may underlie these trends.
Conclusion
Our findings showed an increase in the incidence of noncervical, HPV-related cancers in Alberta from 1975 to 2009, specifically cancers of the oropharynx and anus. This increase has occurred at a time when cervical cancer incidence in the province has been on the decline, likely in relation to widespread implementation of screening programs. The increases in the incidence of oropharyngeal cancer among younger men and of anal cancer among younger women, although not significant, are disturbing, because there are no screening programs for early detection of either of these cancers. To have a large impact on the prevention of these HPV-associated cancers, vaccination programs should be considered for males as well as females. Both oropharyngeal cancer and anal cancers are associated with substantial morbidity, and their treatment comes at a cost of substantial toxicity; therefore, education and prevention programs, such as the HPV vaccination program launched in Alberta and elsewhere,30 are urgently required.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/2/3/E127/suppl/DC1
Footnotes
-
Competing interests: None declared.
-
Contributors: Lorraine Shack, Harold Lau, Longlong Huang, Corinne Doll and Desirée Hao each contributed to the concept and study design, drafted and revised the paper and approved the final version submitted for publication. All of the authors agree to act as guarantors for this work.
-
Funding: Funded by Joe’s Team Triathlon/Alberta Cancer Foundation (ref. 26133). The study sponsors had no role in the design of the study, the collection, analysis or interpretation of data, the writing of the report or the decision to submit the article for publication.
References
- © 2014 Canadian Medical Association or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.