


Abstract
Background: Surgical shutdowns related to the COVID-19 pandemic have resulted in prolonged wait times for nonemergency surgery. We aimed to understand informational needs and generate suggestions on management of the surgical backlog in the context of the ongoing COVID-19 pandemic through focus groups with key stakeholders.
Methods: We performed a qualitative study with focus groups held between Sept. 29 and Nov. 30, 2021, in Ontario, with patients who underwent or were awaiting surgery during the pandemic and their family members, and health care leaders with experience or influence overseeing the delivery of surgical services. We conducted the focus groups virtually; focus groups for patients and family members were conducted separately from health care leaders to ensure participants could speak freely about their experiences. Our goal was to elicit information on the impact of communication about the surgical backlog, how this communication may be improved, and to generate and prioritize suggestions to address the backlog. Data were mapped onto 2 complementary frameworks that categorized approaches to reduction in wait times and strategies to improve health care delivery.
Results: A total of 11 patients and family members and 20 health care leaders (7 nursing surgical directors, 10 surgeons and 3 administrators) participated in 7 focus groups (2 patient and family, and 5 health care leader). Participants reported receiving conflicting information about the surgical backlog. Suggestions for communication about the backlog included unified messaging from a single source with clear language to educate the public. Participants prioritized the following suggestions for surgical recovery: increase supply through focusing on system efficiencies and maintaining or increasing health care personnel; incorporate patient-centred outcomes into triage definitions; and refine strategies for performance management to understand and measure inequities between surgeons and centres, and consider the impact of funding incentives on “nonpriority” procedures.
Interpretation: Patients and their families and health care leaders experienced a lack of communication about the surgical backlog and suggested this information should come from a single source; key suggestions to manage the surgical backlog included a focus on system efficiencies, incorporation of patient-centred outcomes into triage definitions, and improving the measurement of wait times to monitor health system performance. The suggestions generated in this study that may be used to address surgical backlog recovery in the Canadian setting.
The COVID-19 pandemic caused a global disruption to essential care, with profound impacts on wait times for elective (nonemergent) surgery. The true scale of the surgical backlog remains unknown; the Canadian Institute for Health Information reported 560 000 fewer surgeries performed across Canada (excluding Quebec) from March 2020 to June 2021,1 and the Science Table COVID-19 Advisory for Ontario and modelling consensus tables from an equivalent prepandemic calendar time period estimated a backlog of 257 536 cases as of April 2021 in Ontario alone.2 Importantly, available estimates do not encompass upstream effects of diagnostic delay3 and access to care, nor do they consider the number of Canadians on surgical wait lists before the pandemic.4,5 Historic initiatives to reduce surgical wait times have included funding incentives, service expansion and outsourcing, performance management and wait times monitoring for priority procedures.6 Governmental funding has been instituted as a means to address the pandemic-related surgical backlog and ensure provision of care for specific cases (e.g., cancer surgery). However, these incentives may negatively affect patients awaiting certain procedures (e.g., incentives exist for hip and knee surgery but not ankle surgery).7
Strategies to address the surgical backlog must therefore consider inequities that have been built inadvertently into the current system8,9 and further exacerbated by the pandemic. Suggestions to guide equitable surgical recovery in Canada are needed. Engagement of key stakeholders to plan and improve health services, as well as those most affected by surgical cancellation and delays — patients and their families10–13 — is imperative to guide an equitable recovery strategy. Given the need to address the pandemic-induced surgical backlog,7 lack of insight on how to do so6,14–16 and benefits of engaging stakeholders in health system planning,10–13 we aimed to generate suggestions on how to optimize communication and management of the surgical backlog in the context of the ongoing COVID-19 pandemic through focus groups with surgical leaders and patients and their families. This knowledge could be used to inform strategies for surgical backlog recovery in Canada.
Methods
Study design and setting
We conducted this study in Ontario from Sept. 29 to Nov. 30, 2021. The population of Ontario was estimated to be 14.83 million people in 2021,17 and in the year before the pandemic over 640 000 surgical procedures were performed across the province.18 All nonemergent surgery was temporarily stopped on Mar. 15, 2020, until May 26, 2020, and again on Apr. 19 to May 20, 2021. After both shutdowns, nonemergent surgery was gradually resumed.19
We employed a qualitative approach to explore stakeholder views on managing the surgical backlog.20 We used basic qualitative description, which is not based on and does not generate theory.21,22 This approach is widely used in health services research to gather explicit accounts of lived experience and insight on preferred solutions to problems.23 We conducted focus groups, which can generate richer conversation than 1-on-1 interviews, via interactive, synergistic discussion about complex issues.24 We used the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist to promote explicit and comprehensive reporting.25
Participants and recruitment
We used convenience sampling to recruit health care leaders, patients and their family members for our study. We considered patients who had or were waiting for surgery between March 2020 and the time of recruitment and their family members who were adults aged 18 years or older and living in Ontario to be eligible for the study. Eligible health care leaders were nurses, surgeons and administrators (i.e., chief executive officers) with experience and influence overseeing the organization and delivery of surgical services in Canada. We recruited patients and family advisors through the Public Advisory Council at ICES, which has more than 200 patient subscribers, 26 where the lead authors (D.G. and A.N.S.) are appointed. The coordinator at ICES circulated an email to advisors, instructing them to contact the study coordinator (A.M.S.) if they or someone they knew were interested in participating. We recruited health care leaders from the authors’ professional networks and through snowball sampling to achieve a diverse range of geographic (rural and urban), hospital (tertiary and nontertiary centres) and specialty (among surgeons) perspectives. We aimed to involve a minimum of 30 participants, with 6–8 per focus group.24 Patients and family received a $70 gift card as a thank you for their participation.
Data sources
We developed a semistructured focus group guide (Appendix 1, available at www.cmajopen.ca/content/11/2/E255/suppl/DC1) via research team discussion and additional minor refinements to further clarify questions after the first 2 focus groups. We derived the questions and prompts from the study objectives and 2 complementary frameworks. The Wennberg framework was first developed in 2020 and describes 3 broad categories of approaches for procedure wait time reduction: supply, demand and performance management.6 We chose this framework to describe the characteristics of strategies suggested by participants for addressing the surgical backlog. The Powell framework was first published in 2012 and was rigorously developed based on a systematic review of research on available strategies for improving health care delivery and associated outcomes.27 It includes 71 strategies aimed at different levels (e.g., patient, clinician, organization and health care system). We chose this framework because it offered a comprehensive way to categorize the strategies suggested by participants.27
Data collection
Owing to pandemic restrictions, we conducted virtual focus groups. During the focus groups, the lead authors (D.G. and A.N.S.) delivered a brief presentation of the historical and political context. A third-party professional facilitator posed broad questions, invoking additional prompts as needed: How has COVID-19 affected surgery?; What key messages are you getting about the surgical backlog?; What information should be communicated about the backlog?; and What strategies do you recommend to increase supply, decrease demand and optimize performance management? The focus groups were audio-recorded and transcribed via Zoom, then reviewed by a research assistant (A.S.). Interviews were stopped after we reached informational saturation, assessed by the research team through discussion of themes.
Data analysis
J.R. (MSc-trained research associate) and A.R.G. (PhD-trained senior author with 16 years of qualitative research experience) derived the themes inductively by thematic analysis of the transcripts, using Excel to organize data.28,29 They independently analyzed 1 patient and family and 1 health care leader transcript to identify and code all themes, then compared and discussed themes to create a codebook of themes and exemplar quotes (level 1 coding).30 The research associate (J.R.) analyzed the remaining transcripts according to the codebook. All data were reviewed by A.R.G., who expanded or merged themes as needed to refine the codebook (level 2 coding). Other senior authors (D.G. and A.N.S.) independently reviewed all data to verify the themes. A.R.G. also summarized data in tables, then mapped themes to the Wennberg6 and Powell27 frameworks. For example, some participants suggested shifting certain procedures out of hospital, which we mapped to the “decrease demand” component of the Wennberg framework; and some participants suggested performing local needs assessments, which we mapped to the “plan strategies” element of the Powell framework. This mapping showed structures, processes, desired outcomes and suggested strategies to achieve improved outcomes but also showed gaps viewed by participants as the most important. The entire research team reviewed all data.
Ethics approval
This study was approved by the University of Toronto Research Ethics Board (No. 41329).
Results
We held 7 focus groups (2 patient and family, 5 health care leaders) between Sept. 29 and Nov. 30, 2021, after which informational saturation was reached. Duration of the focus groups ranged from 62 to 102 minutes. Eleven patients and family members and 20 health care leaders participated in focus groups. The health care leaders included 7 nurses in surgical program leadership roles; 10 clinicians or surgeons (otolaryngology, gynecology, vascular, thoracic and general surgery); and 3 nonclinician administrators (Table 1).
Demographic characteristics of focus group participants
We explored 3 main issues: impact of communication about the surgical backlog; suggestions for communication about the surgical backlog; and suggestions for surgical backlog recovery. Key themes for each area of discussion included the lack of information and lack of guidance during the waiting period; the need for a single unified source of information and use of clear language when communicating wait times to the public; and prioritization of system efficiencies and preservation of the workforce, incorporation of patient-centred outcomes into triage definitions and improving reporting of metrics to measure the success of surgical backlog recovery.
Impact of communication about the surgical backlog
The overarching theme from all participants pertained to the lack of information about the surgical backlog, and the lack of guidance for both the public and providers during the waiting period (Table 2). Patients and family described waiting for months with no information about when their procedure might take place and inability to get answers by telephone, email or on hospital websites. This led to frustration, inability to make life or family plans, anxiety and depression as a result of disabling conditions, and concern about disease progression and survival. They experienced anxiety when told that their surgery could be cancelled at any time given the uncertainty and related concern of being forgotten if they were bumped, something that was reported to have happened to some participants. Patients and family received messaging that COVID-19 was prioritized over other conditions and, as a result, experienced guilt if they did get treatment, confusion when they learned that some patients were given treatment and frustration at being considered less important than patients with COVID-19.
Impact of wait times communication themes and quotes
Health care leaders said that the lack of information from government or hospital leadership gave them little time to prepare for ramp-up or shutdown of services, confusion when information was conflicting, a lack of insight on strategies or funding to support government directives and an inability on their part to provide patients with guidance or assurances. Health care leaders were told that rates of procedures were back to normal, although they were still struggling to work through the backlog of surgeries and uncertain about how to prioritize them. Some health care leaders noted that the government was promoting a single or unified approach to managing the backlog but did not view this as feasible given the unique needs and resources of different hospitals and regions.
Suggestions for communication about the surgical backlog
Patients and family had suggestions for the content, mechanism and source through which information should be received; health care leaders primarily focused on the content and mechanism, including the importance of engaging surgeons in system-level decision-making (Table 3).
Suggestions for communication about wait times
Patients and family said that the public should be provided with educational information about the cause of surgical delays so that they could better understand the situation and that management of expectations and information could improve performance from a patient’s perspective. They said that every patient should be privy to regular updates of their position on the wait list. Patients and family also said that any communication mechanism to report wait times would be useful including email, telephone applications, internet patient portals to medical records, other websites or verbal communication from a health care professional. Several patients and family said that information should be conveyed from a single, dedicated system-level group with skill in patient communication. They emphasized that sharing of information must be done in a way to reach vulnerable groups. Patients and family highlighted the need for 2-way communication and for resources they could consult to acquire additional information.
Health care leaders suggested educating the public to explain why there is a backlog and that clearing it might take years because of the complexity of the problem, and publish wait times, all with the aim of setting realistic expectations. Some health care leaders disagreed, suggesting that doing so would cause panic and result in overloading emergency services. Most health care leaders emphasized the need to refrain from using the word “elective,” a term that minimizes the urgency of some procedures. Most health care leaders highlighted the need to engage surgeons in system-level decision-making, something they did not feel had happened to date, as this may lead to more feasible solutions.
Suggestions for surgical backlog recovery
The participants had many suggestions about strategies for surgical backlog recovery, including prevention of disease requiring surgery, shifting services out of hospital, sending patients to other jurisdictions, increasing the pool of health care professionals, improving or expanding services, wait list management, funding, and learning from other countries and past pandemics (Table 4). There were important differences between the suggestions of patients and family and health care leaders and discussion around specific concerns of some strategies; some of these concerns included maintaining quality of care, burdening other aspects of the health care system (e.g., emergency department) through earlier hospital discharge or shifting surgical services out of hospitals, and maintaining patient and surgeon autonomy (e.g., through centralized referral systems, alternate payment plans to surgeons) (Appendix 2, available at www.cmajopen.ca/content/11/2/E255/suppl/DC1).
Suggestions for strategies to manage wait times
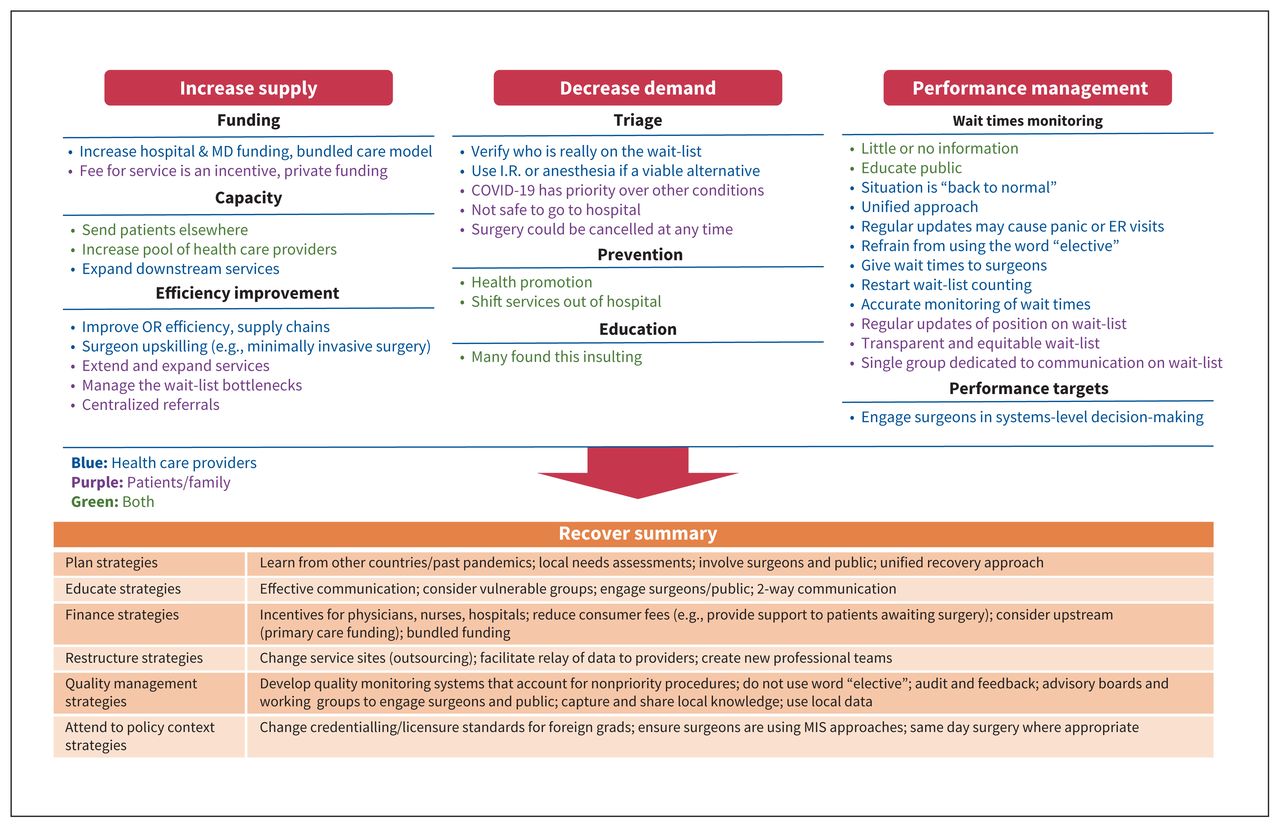
Participants were clear that funding initiatives alone would not address the backlog; 1 participant stated: “You cannot pay your way out of this” [Health care leader 3 (HCL Focus Group 1)]. Within the Wennberg6 framework (Figure 1), most participants felt that the following strategies should be key considerations: first, directing the focus on improving systems efficiencies, such as outsourcing surgeries to ambulatory surgery centres and same-day discharge, were seen as a high priority. Maintaining health care personnel and forward thinking to increase future system capacity was seen as a key priority; this included incentivizing entry into the nursing profession and increasing the number of operating room technicians and anesthesia assistants within hospitals. Second, incorporating patient-centred outcomes into triage definitions was highlighted to improve equity. Aspects such as time sensitivity and patient discomfort were emphasized rather than simplistic categorizations of “cancer” and “noncancer;” 1 surgeon pointed out that some types of thyroid cancers may safely be delayed without an impact on patient outcome. Third, the current performance management strategies such as reporting of wait times and performance targets for priority procedures were found to be lacking. Inequities in the current system were highlighted and will be further exacerbated if wait times for priority procedures alone are reported. All themes and quotes are included in Appendix 3, available at www.cmajopen.ca/content/11/2/E255/suppl/DC1.
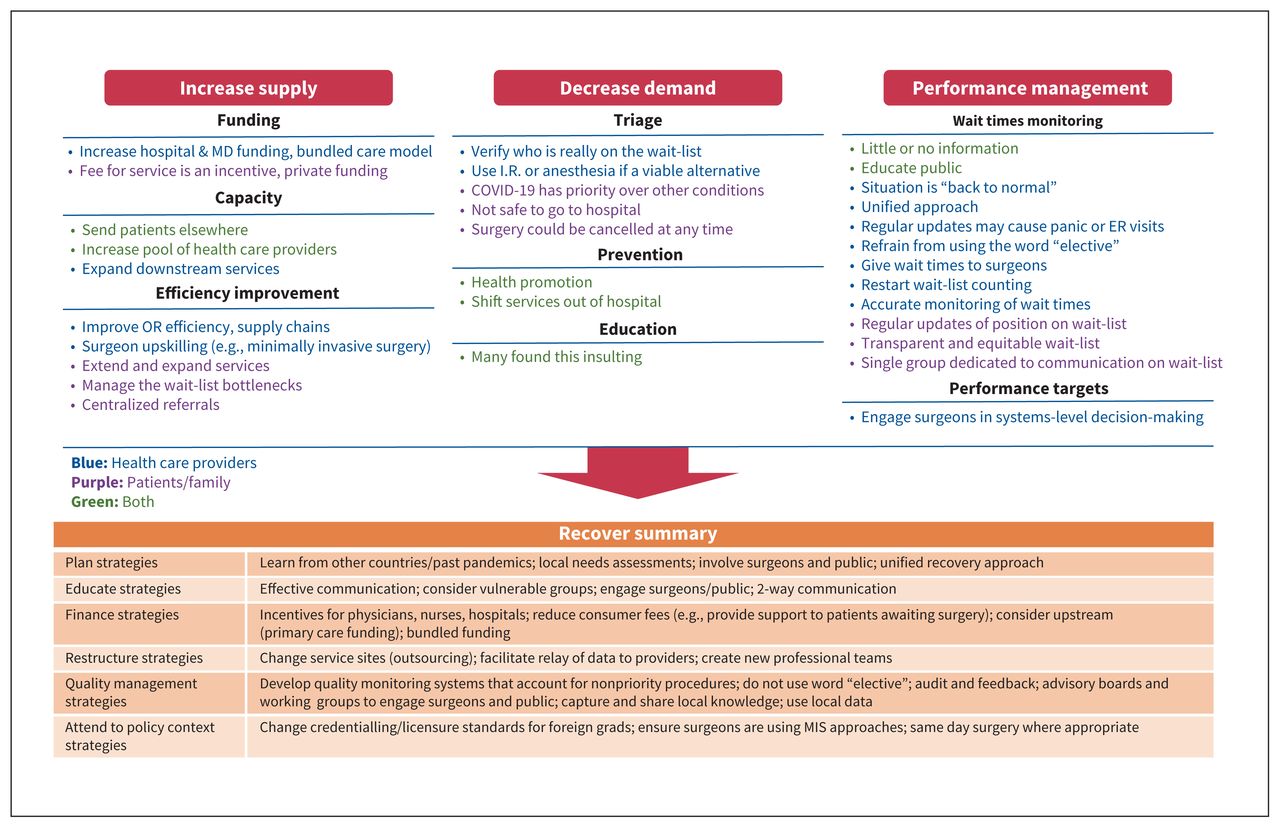
Summary of suggested strategies for surgical backlog recovery. Note: ER = emergency room, IR = interventional radiology, MIS = minimally invasive surgery, OR = operating room.
Interpretation
We conducted focus groups with health care leaders and patients and their families to understand informational needs related to the pandemic-induced surgical backlog, and generate suggestions for improved communication and for an equitable recovery strategy. Participants expressed frustration with the lack of communication related to surgical slowdowns and ramp-ups and information related to an overall recovery plan. Patients and families felt that information was being withheld, whereas health care leaders related that they often received information at the same time as the public. During ramp-ups, health care leaders received messages that procedure rates were “back to normal” but felt that they were still struggling with a substantial backlog. All stakeholders offered suggestions for strategies to improve communication about and mitigate the backlog. Of all these strategies, most participants considered the following to be the most important to pursue: increase supply through focusing on system efficiencies and maintaining or increasing health care personnel; incorporate patient-centred outcomes into triage definitions; and refine strategies for performance management to understand and measure inequities between surgeons and centres.
Wennberg categorized initiatives that have been implemented successfully in the Canadian setting through increased supply, decreased demand and performance management.6 When “increase supply” initiatives were discussed with the participants, it was acknowledged that the surgical backlog could not be addressed in a silo. Upstream effects, such as provision or increasing the supply of health care workers and support for primary care screening, and downstream effects, such as support for increased surgical volume (e.g., postoperative nursing care, programs to support same-day discharge) were discussed. A successfully implemented strategy to increase supply before the pandemic was moving low-risk procedures out of urban centres to community-based clinics and rural hospitals.6 Since the burden of COVID-19 disease was greater in urban centres, a strategy like this would free capacity for high-risk procedures in tertiary care centres.31 A similar strategy was proposed in the United Kingdom, where local and regional centres that were relatively protected from the disease burden of COVID-19 disease burden would provide ongoing surgical care.32 These types of strategies are important to develop to maintain surgical care in the future, for subsequent COVID-19 outbreaks.33 The importance of maintaining equity in access across demographics and specialties is a key consideration of any potential strategy.32,34 Single-entry models and team-based care have also been proposed to ensure an equitable recovery strategy,8 as well as the development of tools to estimate wait times within groups based on available resources.35
Strategies that patients and family were least accepting of were those related to decreasing demand.6 They felt that nonemergent surgery and prevention strategies had been triaged behind COVID-19 throughout the pandemic, and the necessity of surgical care was being discounted. Performance management, which encompasses monitoring of wait times and performance targets, is an important aspect of recovery, but participants expressed concern over how this information was made available and how it affected other cases (e.g., while targets for priority procedures may be met, “nonpriority” procedures continued to wait). Health care leaders discussed that the current provincial monitoring of wait times did not adequately reflect their experience and were not adequately disseminated; for example, wait times for individual surgeons should be available to their hospital or division leads to understand inequities within departments that may be mitigated to lessen the impact on patients.
Policy strategies must consider local contextual factors and the disproportionate impact of the pandemic on some regions and hospitals. Therefore, future directions of this research will include a larger number of stakeholders from across Canada. Involvement of patients and family in our study raised several important issues that may also be considered to support those affected by the backlog; for example, patients understood that prolonged waits cannot be changed in many instances, but they suggested that provincially insured access to physiotherapy and other resources may be helpful for symptom management during the wait. We did not identify any previous studies that consulted patients and their families about strategies to manage surgical wait times. Although all of the systems complexities of surgical wait times may not be apparent to the public, it was apparent to them that the system is not equitable; transparent processes and communication was a key concern expressed by patients and family. Unified messaging from a single source and involvement of patients and professionals in shaping the recovery plan would increase transparency, particularly as we experience subsequent waves of the COVID-19 pandemic.
We used rigorous qualitative methods and complied with qualitative reporting criteria. Our findings are strengthened by the good congruence between patients and family and health care leaders who were interviewed.
Limitations
Our study is limited by the population interviewed, specifically people in health care leadership positions and patients who had or were awaiting surgery in Ontario and their families. Our convenience sampling strategy aimed to recruit a diverse sample of people who could speak to strategies to manage the backlog; however, not all regions and hospitals were equally affected by the pandemic, and, therefore, there are other perspectives that were not captured. In future research, we will aim to involve more stakeholders in ranking the most important recovery strategies. Finally, the suggestions represent the perspectives of patients and family and health care leaders but may not reflect the perspectives of other key stakeholders (e.g., policy-makers); other effective organizational strategies may not have been discussed.
Conclusion
We identified priority strategies for improving communication about and management of the surgical backlog through focus groups with key stakeholders. Improving equity through incorporating patient-centred outcomes into case prioritization definitions, maintaining health care personnel, and improving system efficiencies and monitoring with publicly available local data were identified as priority areas. Future work includes a Delphi consensus with a larger group of stakeholders to prioritize these suggestions. These strategies are applicable across Canada for managing the pandemic-induced surgical backlog.
Acknowledgements
The authors thank the ICES Public Advisory Council and the ICES Public Engagement Mailing List for assisting in patient recruitment, and the patients and family members and health care leaders that generously gave their time to participate in this study. The authors thank Karyn Dumble from The Monarch Park Group for facilitating the focus groups.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Andrea Simpson and David Gomez contributed equally. Andrea Simpson and Anna Gagliardi drafted the manuscript. Andrea Simpson, David Gomez, Anna Gagliardi, Jessica Ramlakhan, Anne Sorvari and Alawia Sherif acquired the data. Anna Gagliardi and Jessica Ramlakhan performed the data analysis. Andrea Simpson, Anna Gagliardi, Nancy Baxter, David Urbach and Elizabeth Miazga interpretated the data. All of the authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by the Research Innovation Council of the St. Michael’s Hospital Foundation (David Gomez). Andrea Simpson has received salary support for research from the Chair in Women’s Health, St. Michael’s Hospital.
Data sharing: Data are available upon reasonable request. The data that support the findings of this study are available on request from the corresponding author, Andrea Simpson. The data are not publicly available because they contain information that could compromise the privacy of research participants.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and Ministry of Long-Term Care (MLTC). The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES, or the Ontario MOH or MLTC is intended or should be inferred.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/2/E255/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.