


Article Figures & Tables
Figures
- Figure 1:
Study flowchart. Note: VA = Veterans Affairs.
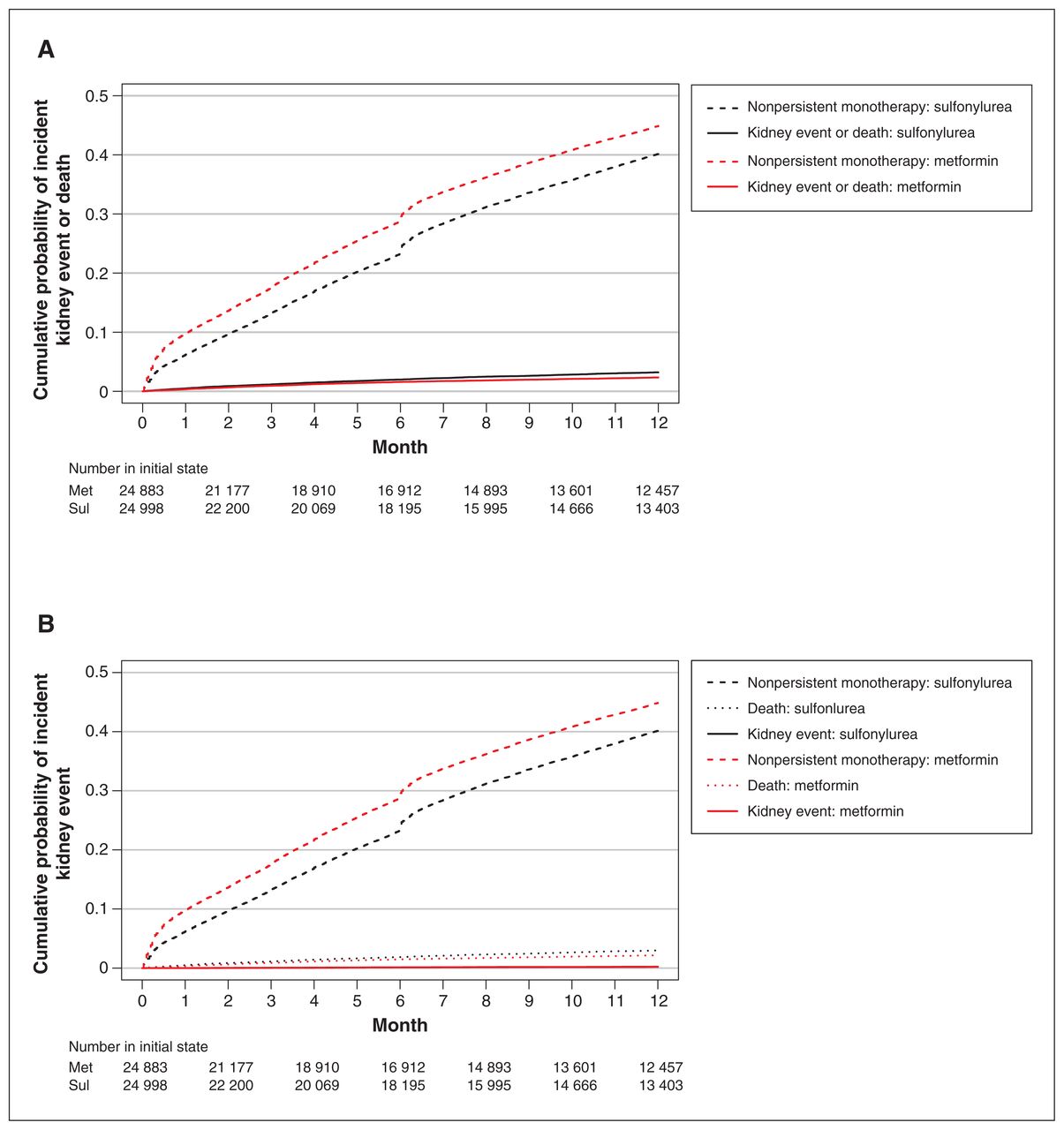
- Figure 2:
Full Aalen–Johansen cumulative probability plot of a kidney event (i.e., 40% decline in estimated glomerular filtration rate or end-stage renal disease) or death (panel A) or of a kidney event (panel B) in the weighted cohort for the first 360 days after reaching an estimated glomerular filtration rate less than 60 mL/min/1.73 m2 by treatment group. Note: Met = metformin, Sul = sulfonylurea.
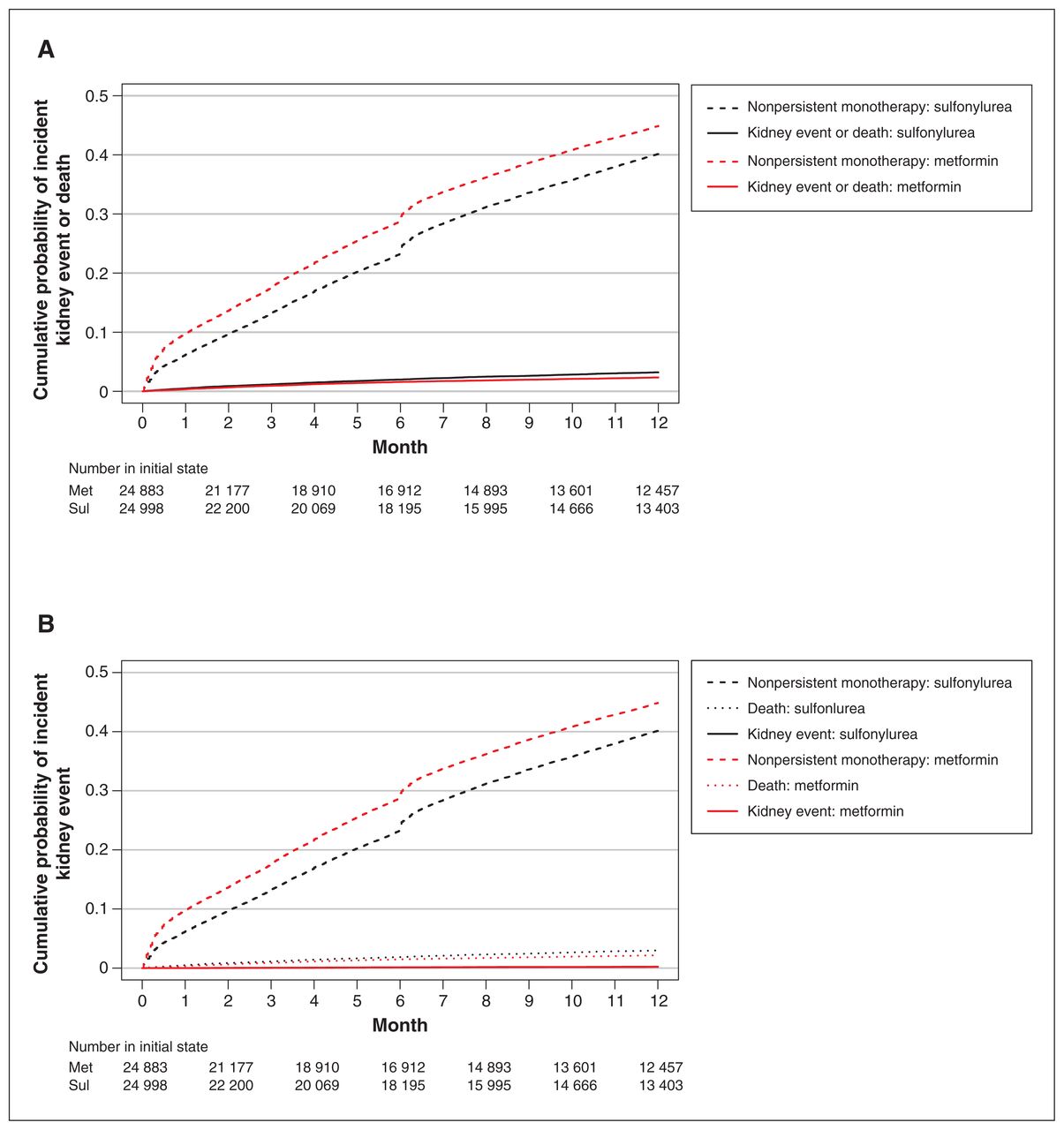
- Figure 3:
Full Aalen–Johansen cumulative probability of a kidney event (i.e., 40% decline in estimated glomerular filtration rate or end-stage renal disease) or death (panel A) or of a kidney event (panel B) in the weighted cohort for those who persisted on their treatment for at least 361 days after reaching an estimated glomerular filtration rate less than 60 mL/min/1.73 m2 by treatment group. Note: Met = metformin, Sul = sulfonylurea.
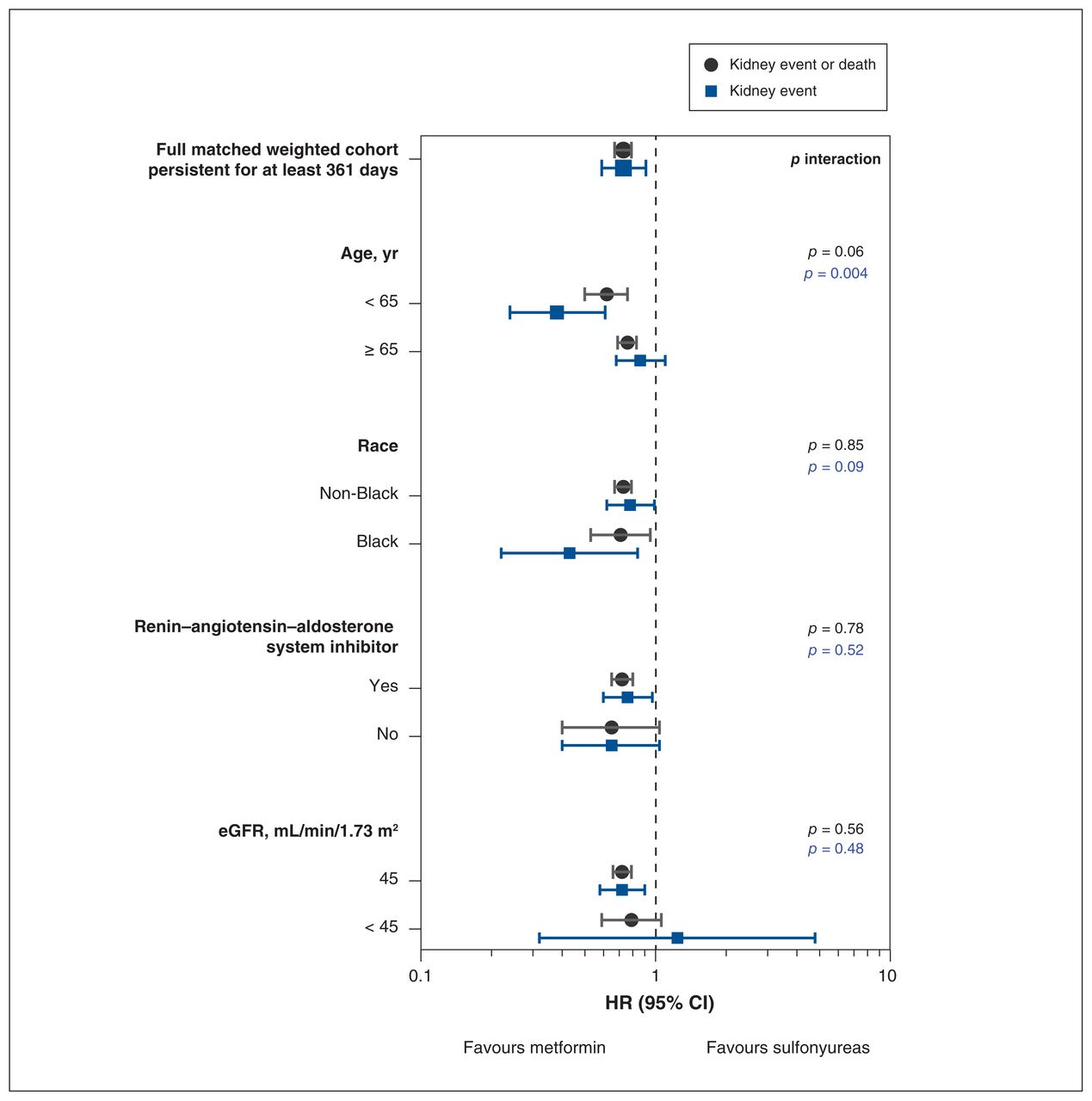
- Figure 4:
Propensity score–weighted hazard ratios (HRs) for the primary and secondary outcomes by subgroup for patients persistent on therapy at 361 days after reaching an estimated glomerular filtration rate (eGFR) less than 60 mL/min/1.73 m2. Note: CI = confidence interval.



Tables
- Table 1:
Patient characteristics on index date of kidney function decline and at 361 days after the index date for persistent patients
Characteristic No. (%) of patients in propensity score–weighted cohort at index date* SMD† No. (%) of patients in propensity score–weighted cohort at 361 d SMD† Metformin
n = 24 883Sulfonylureas
n = 24 998Metformin
n = 12 571Sulfonylureas
n = 12 637Age, yr, median (IQR) 70.7 (63.7–78.1) 70.5 (63.7–78.1) 0.001 72.5 (65.4–79.5) 72.2 (65.3–79.4) 0.003 Sex, male 24362 (97.9) 24476 (97.9) 0.001 12334 (98.1) 12406 (98.2) 0.004 Race White 20908 (84.0) 21007 (84.0) 0.002 10918 (86.9) 10982 (86.9) 0.002 Black 3503 (14.1) 3512 (14.0) 1424 (11.3) 1430 (11.3) Other‡ 472 (1.9) 479 (1.9) 229 (1.8) 226 (1.8) Time from cohort entry to kidney threshold, mo, median (IQR) 14.2 (5.9–30.7) 14.3 (6.1–30.9) 0.014 28.4 (18.9–45.4) 28.6 (19.0–45.6) 0.009 Year reached kidney threshold 2002–2003 2815 (11.3) 2808 (11.2) 0.027 1568 (12.5) 1545 (12.2) 0.038 2004–2005 4308 (17.3) 4268 (17.1) 2236 (17.8) 2234 (17.7) 2006–2007 5005 (10.1) 5216 (20.9) 2722 (21.7) 2853 (22.6) 2008–2009 3726 (15.0) 3781(15.1) 1983 (15.8) 1999 (15.8) 2010–2011 3291 (13.2) 3207 (12.8) 1737 (13.8) 1673 (13.2) 2012–2013 2603 (10.5) 2556 (10.2) 1281(10.2) 1254 (9.9) 2014–2015 2164 (8.7) 2181 (8.7) 1038 (8.2) 1076 (8.5) 2016 971 (3.9) 981 (3.9) 5 (0.0) 3 (0.0) Laboratory variables HbA1c, %, median (IQR) 6.5 (6.1–7.1) 6.5 (6.1–7.2) 0.007 6.5 (6.1–7.0) 6.50 (6.0–7.1) 0.007 Missing HbA1C measure 1011 (4.1) 994 (4.0) 0.004 503 (4.0) 488 (3.9) Historical eGFR before kidney threshold, mL/min/1.73 m2, median (IQR)§ 69.3 (64.5–76.6) 69.3 (64.5–76.6) 0.001 – – eGFR at kidney threshold, mL/min/1.73 m2, median (IQR) 55.6 (51.4–58.0) 55.6 (51.4–58.0) 0.002 55.9 (52.2–58.1) 55.8 (52.2–58.2) 0.003 eGFR at 361 days, mL/min/1.73 m2, median (IQR) – – 63.5 (55.8–72.3) 63.7 (55.7–72.3) 0.007 Missing eGFR 293 (1.2) 296 (1.2) 0.001 964 (7.7) 957 (7.6) 0.004 Hemoglobin, g/dL, median (IQR) 14.0 (13.0–15.1) 14.1 (13.0–15.1) 0.003 13.9 (12.9–14.9) 14.0 (12.9–15.0) 0.004 Missing hemoglobin 1507 (6.1) 1503 (6.0) 0.002 777 (6.2) 792 (6.3) 0.003 Low-density lipoprotein, mmol/L, median (IQR) 2.28 (1.81–2.82) 2.28 (1.81–2.82) 0.002 2.18 (1.76–2.64) 2.18 (1.76–2.67) 0.001 Missing low-density lipoprotein measure 779 (3.1) 781 (3.1) < 0.001 310 (2.5) 309 (2.4) 0.004 Microalbumin-to-creatinine ratio stage Normal (< 30 mg/g) 9616 (38.6) 9670 (38.7) 0.003 5261 (41.9) 5305 (42.0) 0.003 Microalbuminuria (30–300 mg/g) 2775 (11.2) 2771.0 (11.1) 1516 (12.1) 1523 (12.1) Macroalbuminuria (> 300 mg/g) 788 (3.2) 781.6 (3.1) 370 (2.9) 373 (3.0) Missing microalbumin-to-creatinine ratio 11703 (47.0) 11775 (47.1) 5424 (43.1) 5436 (43.0) Proteinuria by urinalysis Negative 11736 (47.2) 11787 (47.2) 0.002 6101 (48.5) 6129 (48.5) 0.002 Urine protein trace or 1+ 3533 (14.2) 3561 (14.2) 1700 (13.5) 1711 (13.5) Proteinuria present at 2+ 831 (3.3) 838 (3.4) 330 (2.6) 330 (2.6) Proteinuria present at 3+ or 4+ 336 (1.3) 336 (1.3) 127 (1.0) 126 (1.0) Unknown urine protein measure 8446 (33.9) 8476 (33.9) 4313 (34.3) 4341 (34.4) Clinical variables Systolic blood pressure, mm Hg, median (IQR) 131 (119–142) 131 (119–142) 0.002 132 (120–142) 132 (121–142) 0.005 Diastolic blood pressure, mm Hg, median (IQR) 72 (64–80) 72 (64–80) 0.001 72 (64–79) 72 (64–79) 0.001 BMI, median (IQR) 30.3 (27.0–34.4) 30.3 (27.0–34.3) 0.003 30.2 (27.0–34.2) 30.2 (27.0–34.1) 0.001 Missing BMI measure 4688 (18.8) 4719 (18.9) 0.001 2290 (18.2) 2306 (18.3) 0.003 Baseline comorbidities Malignant disease¶ 2971 (11.9) 2990 (12.0) 0.001 1622 (12.9) 1622 (12.8) 0.002 Liver disease 625 (2.5) 621 (2.5) 0.002 230 (1.8) 229 (1.8) 0.001 HIV 89 (0.4) 90 (0.4) 0.001 39 (0.3) 40 (0.3) 0.001 Congestive heart failure 3051 (12.3) 3071 (12.3) 0.001 1580 (12.6) 1592 (12.6) 0.001 Cardiovascular disease 7935 (31.9) 8006 (32.0) 0.003 3987 (31.7) 4019 (31.8) 0.002 Stroke 831 (3.3) 827 (3.3) 0.002 399 (3.2) 401 (3.2) < 0.01 Transient ischemic attack 322 (1.3) 332 (1.3) 0.003 155 (1.2) 153 (1.2) 0.002 Serious mental illness** 4957 (19.9) 5035 (20.1) 0.005 2401 (19.1) 2430 (19.2) 0.003 Smoking 3045 (12.2) 3068 (12.3) 0.001 1262 (10.0) 1263 (10.0) 0.002 Chronic obstructive pulmonary disease 4284 (17.2) 4321 (17.3) 0.002 2157 (17.2) 2166 (17.1) < 0.01 History of respiratory failure 821 (3.3) 821 (3.3) 0.001 543 (4.3) 533 (4.2) 0.005 History of sepsis 406 (1.6) 414 (1.7) 0.002 291 (2.3) 291 (2.3) 0.001 History of pneumonia 1074 (4.3) 1092 (4.4) 0.003 648 (5.2) 640 (5.1) 0.004 Arrhythmia 4387 (17.6) 4418 (17.7) 0.001 2399 (19.1) 2414 (19.1) < 0.01 Cardiac valve disease 919 (3.7) 929 (3.7) 0.001 497 (4.0) 503 (4.0) 0.002 Parkinson disease 234 (0.9) 237 (0.9) 0.001 162 (1.3) 158 (1.3) 0.003 Urinary tract infection 1055 (4.2) 1067 (4.3) 0.001 640 (5.1) 645 (5.1) 0.001 Osteomyelitis 156 (0.6) 154 (0.6) 0.002 65 (0.5) 64 (0.5) 0.002 Osteoporosis 200 (0.8) 206 (0.8) 0.002 118 (0.9) 115 (0.9) 0.003 Falls 57 (0.2) 59 (0.2) 0.002 59 (0.5) 57 (0.4) 0.003 Fractures 556 (2.2) 556 (2.2) 0.001 315 (2.5) 313 (2.5) 0.002 Amputation 118 (0.5) 123 (0.5) 0.002 55 (0.4) 55 (0.4) 0.001 Retinopathy 286 (1.1) 287 (1.1) < 0.001 117 (0.9) 121 (1.0) 0.003 Use of medications Angiotensin-converting enzyme inhibitors 15958 (64.1) 16080 (64.3) 0.004 7623 (60.6) 7690 (60.9) 0.004 Angiotensin II receptor blockers 2904 (11.7) 2904 (11.6) 0.002 1647 (13.1) 1644 (13.0) 0.003 β-blockers 12699 (51.0) 12770 (51.1) 0.001 6533 (52.0) 6565 (51.9) < 0.01 Calcium-channel blockers 7417 (29.8) 7454 (29.8) < 0.001 3801 (30.2) 3820 (30.2) < 0.01 Thiazide- and potassium-sparing diuretics 10072 (40.5) 10169 (40.7) 0.004 4531 (36.0) 4578 (36.2) 0.004 Loop diuretics 5059 (20.3) 5087 (20.3) < 0.001 2433 (19.4) 2448 (19.4) 0.001 Other antihypertensive medications 6873 (27.6) 6887 (27.6) 0.002 3834 (30.5) 3834 (30.3) 0.003 Statin lipid-lowering drugs 16763 (67.4) 16917 (67.7) 0.007 9059 (72.1) 9119 (72.2) 0.002 Nonstatin lipid-lowering agents 4237 (17.0) 4264 (17.1) 0.001 2275 (18.1) 2280 (18.0) 0.002 Antiarrhythmic drugs, digoxin and inotropes 2313 (9.3) 2321 (9.3) < 0.001 1072 (8.5) 1078 (8.5) < 0.01 Anticoagulant drugs and platelet inhibitors 2578 (10.4) 2588 (10.4) < 0.001 1386 (11.0) 1394 (11.0) < 0.01 Nitrates 3652 (14.7) 3689 (14.8) 0.002 1716 (13.6) 1739 (13.8) 0.003 ASA 5332 (21.4) 5385 (21.5) 0.003 2533 (20.1) 2570 (20.3) 0.005 Non-ASA platelet inhibitors 2643 (10.6) 2660 (10.6) 0.001 1329 (10.6) 1343 (10.6) 0.002 Antipsychotic drugs 1662 (6.7) 1685 (6.7) 0.003 747 (5.9) 745 (5.9) 0.002 Oral glucocorticoids 1823 (7.3) 1845 (7.4) 0.002 894 (7.1) 892 (7.1) 0.002 Indicators of health care use†† Admitted to hospital within year (Veterans Health) 3550 (14.3) 3600 (14.4) 0.004 1510 (12.0) 1538 (12.2) 0.005 Admitted to hospital in 30 days (Veterans Health) 934 (3.8) 953 (3.8) 0.003 188 (1.5) 187 (1.5) 0.001 Admitted to hospital within year (Medicare/Medicaid) 2851 (11.5) 2860 (11.4) < 0.001 1521 (12.1) 1507 (11.9) 0.005 Admitted to hospital in 30 days (Medicare/Medicaid) 450 (1.8) 461 (1.8) 0.003 197 (1.6) 198 (1.6) < 0.01 Medicaid use in previous year 298 (1.2) 307 (1.2) 0.003 143 (1.1) 142 (1.1) 0.001 Medicare use in previous year 9128 (36.7) 9129 (36.5) 0.003 5221 (41.5) 5213 (41.3) 0.006 Nursing home encounter in previous year 97 (0.4) 102 (0.4) 0.003 66 (0.5) 67 (0.5) < 0.01 Medicare Advantage use 3979 (16.0) 3998 (16.0) < 0.001 2498 (19.9) 2517 (19.9) 0.001 Note: ASA = acetylsalicylic acid, BMI = body mass index, eGFR = estimated glomerular filtration rate, IQR = interquartile range, SMD = standardized mean difference.
↵* Unless indicated otherwise.
↵† Standardized mean differences are the absolute difference in means or percentage divided by an evenly weighted pooled standard deviation, or the difference between groups in number of standard deviations. In the weighted cohort, all standardized differences were less than 0.01, suggesting there were no important imbalances.
↵‡ Other races include American Indian or Alaska Native, Asian, and Native Hawaiian or Pacific Islander.
↵§ Historical eGFR is the eGFR before the patient met the inclusion criteria of eGFR < 60 mL/min/1.73 m2; eGFR at kidney threshold indicates the eGFR when the patient met the inclusion criteria of eGFR < 60 mL/min/1.73 m2.
↵¶ Malignant disease includes all types of cancer except nonmelanoma skin cancer.
↵** Serious mental illness included schizophrenia, depression, bipolar disorder, dementia and post-traumatic stress disorder.
↵†† The Veterans Health Administration provides health care coverage for those who serve their country through military services. Medicare and Medicaid health services are federal health care programs for eligible people older than 65 years. Medicare Advantage is a Medicare plan offered by private insurers that provides hospital, outpatient and (usually) prescription drug coverage, supplanting benefits under other Medicare plans.
- Table 2:
Rates and hazard ratios for kidney composite outcomes among patients who persisted on metformin or sulfonylurea in matched weighted cohort in first 360 days and from day 361 onward of reaching reduced kidney function threshold*
Outcome irst 360 days 361 days onward Metformin
n = 24 883Sulfonylurea
n = 24 998Metformin
n = 12 571Sulfonylurea
n = 12 637Primary outcome: kidney events or death Number of events 576 786 747 1033 Person-time, yr 17194 18278 28191 28429 Events per 1000 person-years (95% CI) 33.5 (30.9–36.3) 43.0 (40.1–46.0) 26.5 (24.7–28.5) 36.3 (34.2–38.6) PS-weighted HR, unadjusted (95% CI) 0.78 (0.71–0.85) Ref. 0.73 (0.67–0.79) Ref. PS-weighted HR, adjusted* (95% CI) 0.79 (0.72–0.87) Ref. 0.76 (0.70–0.83) Ref. Secondary outcome: kidney events Number of events 49 56 110 149 Person-time, yr 17194 18278 28191 28429 Events rates per 1000 person-years (95% CI) 2.9 (2.2–3.8) 3.1 (2.4–4.0) 3.9 (3.2–4.7) 5.2 (4.5–6.1) PS-weighted HR, unadjusted (95% CI) 0.94 (0.67–1.33) Ref. 0.73 (0.59–0.91) Ref. Secondary outcome: death Number of events 527 730 642 903 Person-time, yr 17201 18300 28240 28717 Events rates per 1000 person-years (95% CI) 30.6 (28.2–33.3) 40 (37.2–42.9) 22.7 (21.0–24.5) 31.5 (29.5–33.5) PS-weighted HR, unadjusted (95% CI) 0.76 (0.69–0.84) Ref. 0.72 (0.66–0.79) Ref. Note: HR = hazard ratio, PS = propensity score, Ref. = reference category.
↵* Cox Proportional Hazards model for time to event. Adjusted for demographics, clinical information derived from the electronic health record, comorbidities, use of medications and health care utilization (see Appendix 1, Supplemental Table 1, available at www.cmajopen.ca/content/11/1/E77/suppl/DC1). All continuous variables were modelled as restricted cubic splines. All covariates in PS model included in the PS-weighted and adjusted model (see Appendix 1, Supplemental Table 1).
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.