


Abstract
Background Uptake of treatment for hepatitis C virus (HCV) is low in Canada despite its publicly funded health care system. We explored the uptake of HCV treatment within the Canadian Co-infection Cohort to determine if some treatment centres have been more successful than others at starting patients with HIV–HCV coinfection on HCV treatment.
Methods We estimated the variation between 16 centres in the uptake of HCV treatment using a Weibull time-to-event model with adjustment for patient characteristics that are thought likely to influence the uptake of treatment. We asked the principal investigator at each centre about access to hepatitis-related specialists and services and the importance of various criteria when determining if a patient with HIV–HCV coinfection should receive treatment for HCV.
Results Among 681 untreated patients in the Canadian Co-infection Cohort, 163 patients with HIV–HCV coinfection started HCV treatment over a period of 1827 patient-years (9 per 100 patient-years). Even after adjustment for case mix, there was still appreciable variation in treatment uptake between centres, with mean hazard ratios of 0.43 (95% credible interval 0.11–1.3) and 3.6 (95% credible interval 1.7–8.4) for the centres least and most likely to start an average patient with HIV–HCV coinfection on HCV treatment. The most important criteria reported by principal investigators for determining eligibility for treatment were severity of fibrosis, current psychiatric comorbidities, current alcohol intake, past HCV treatment and a history of reinfection with HCV. However, the opinions were wide-ranging: 8 of the 15 criteria elicited both the responses “less important” and “very important.”
Interpretation The magnitude of the centre effects and diverse opinions about the importance of treatment eligibility criteria suggest that provider-related barriers to HCV treatment uptake are as important as patient-related barriers.
The burden of hepatitis C virus (HCV) infection on the Canadian health care system has steadily increased since the 1990s, and it is expected to further increase as patients age.1 In 2007, the prevalence of HCV infection in Canada was estimated to be 0.8%, but it is also estimated that 21% of infected individuals are unaware of their infection.2 Patients with HIV are at a high risk of coinfection because both infections are transmitted by injection drug use, and 20% of patients with HIV also have HCV infection.3 In patients with HIV–HCV coinfection, liver-related and all-cause HCV hospital admissions have increased in Canada by 30% to 40% per year during the decade from 1994 to 2004.1 Curative treatment for HCV is available and cost-effective for patients with or without HIV coinfection;4,5 this treatment greatly reduces the progression to end-stage liver disease, decompensation, transplantation, admission to hospital and death. For coinfected patients, effective treatment for HCV also reduces HIV progression and nonliver-related mortality.6,7 Guidelines recommend that all coinfected patients should be considered for HCV treatment, particularly those with significant liver fibrosis (greater than F2 by Metavir staging on liver biopsy).8,9
Current HCV treatment is complex, difficult to tolerate and requires expert supervision. Uptake of HCV treatment in Canada is low, despite its publicly funded health care system. In particular, uptake is considered unacceptably low among injection drug users, the group among which most new HCV infections arise.10 Two-thirds of injection drug users in Canada are infected with HCV.11,12 In a recent survey, 80% of Canadian physicians who specialize in HCV said that they were not likely to provide HCV treatment to active injection drug users.13 Injection drug users are often considered ineligible for treatment because of poor adherence to care, psychiatric illness or ongoing use of drugs or alcohol.14,15 Even if eligible, patients with HCV may be reluctant to start treatment.16
In the United States, patients are less likely to be offered and to accept HCV treatment if they are older, male, not white, infected with a difficult-to-treat HCV genotype, have psychiatric illness, or if they use drugs or alcohol.17–19 Many studies have evaluated these patient-related barriers to treatment,20,21 which are difficult to overcome. Provider and institutional barriers are also important;17,22 these are perhaps more amenable to intervention. Although having access to an experienced provider is clearly important for the uptake of HCV treatment,17–19 it is not clear what other provider and institutional barriers are involved.
Given that many patients with HIV–HCV coinfection are current or past injection drug users, this subgroup represents a priority for HCV treatment if the risk of transmission is to be reduced and health care costs contained. Thus, a better understanding of provider and institutional barriers to treatment in Canada is required. In this study, we investigated the uptake of HCV treatment within the Canadian Co-infection Cohort to determine if some centres were more successful than others at initiating HCV treatment, and we explored factors that could be associated with differences between centres.
Methods
The Canadian Co-infection Cohort is a prospective cohort of adult patients infected with both HIV and HCV.23 Patients have been enrolled at 16 centres across Canada since 2003; these centres include university hospitals and community-based clinics in small and large urban areas (Table 1). All eligible patients at each centre were invited to participate. Patients who gave informed consent underwent an initial evaluation followed by study visits every 6 months. At each visit, sociodemographic and behavioural information were self-reported by use of questionnaires; blood was obtained for biochemical, virologic and immunologic analyses; and data about medical treatments and diagnoses were collected by research personnel. The AUDIT-C questionnaire was used to measure alcohol use.24 Research involving this cohort has been approved by the community advisory committee of the Canadian HIV Trials Network and by the institutional ethics boards of all participating centres.
Statistical analysis
We modelled time to uptake of HCV treatment in the cohort of patients not receiving HCV treatment before or at enrolment. We fitted a Weibull time-to-event model with a normally distributed random intercept for each centre in order to estimate the variation in treatment uptake between centres. In this model, we adjusted for patient characteristics that we thought were likely to influence the uptake of treatment; we then ranked the centres according to their success in starting patients on HCV treatment. To allow for differences between centres in their case mix, we adjusted for the following covariates: sex, ethnic background, HCV genotype, and, at cohort enrolment, age, duration of HCV infection, use of combination antiretroviral therapy, CD4 cell count, and self-reported homelessness, psychiatric diagnosis, use of injection drugs, and use of alcohol.17–19 In 2 subsequent analyses, we added additional covariates to the model to allow for differences in treatment uptake between primary and tertiary care centres or between provinces (British Columbia, Ontario and Alberta, Quebec and Nova Scotia). Ontario and Alberta have similar regulations that govern access to HCV treatment, as do Quebec and Nova Scotia. The model was fit in WinBUGS using uninformative prior distributions for each of the model’s parameters: normal distributions with large variance for covariate effects25 and a wide uniform distribution for the standard deviation of centre effects.26
In a sensitivity analysis, we added prior information about centre effects via an informative prior distribution for the effect of each centre. That is, we attempted to provide additional information about these effects, rather than limit the information in our analysis to just the data collected during follow-up. We modelled the probability that patients received HCV treatment before or at enrolment using a log binomial model that included the covariates listed above.27,28 With this model, we estimated the risk in each centre that patients received treatment before or at enrolment relative to the average risk across all centres. We then used these risk ratios to calculate a mean for the prior distribution for each centre effect, rather than assuming a normal distribution with a mean of zero.
To explore possible reasons for differences in the uptake of HCV treatment between centres, we asked the principal investigator at each centre to complete a web-based survey (www.surveymonkey.com). Our survey (Appendix 1, available at www.cmajopen.ca/content/1/3/E106/suppl/DC1) contained questions about access to hepatitis-related specialists and services and the importance of various criteria when determining which patients should undergo HCV treatment. These questions were a subset of questions asked in a study of variation in the use of HCV services in the United Kingdom.29 The original paper-based survey was pilot-tested on clinicians before use; we modified the questions without further testing to make them more suitable for our web-based survey. In particular, we expanded a question about access to tests to include access to transient elastography and to HCV-related specialists (hepatologists, nephrologists, psychiatrists or psychologists, clinical pharmacists, HCV-dedicated nurses or social workers) and services (outreach teams, addiction services, opioid-substitution programs). Transient elastography, a noninvasive ultrasound-based method of measuring liver stiffness,30 is now the standard method for evaluating liver fibrosis because of its simplicity, low cost and greater than 90% positive predictive value for advanced fibrosis.9 We calculated associations between the specialists and services available at each centre and the median centre ranks from our model for the uptake of HCV treatment.
Results
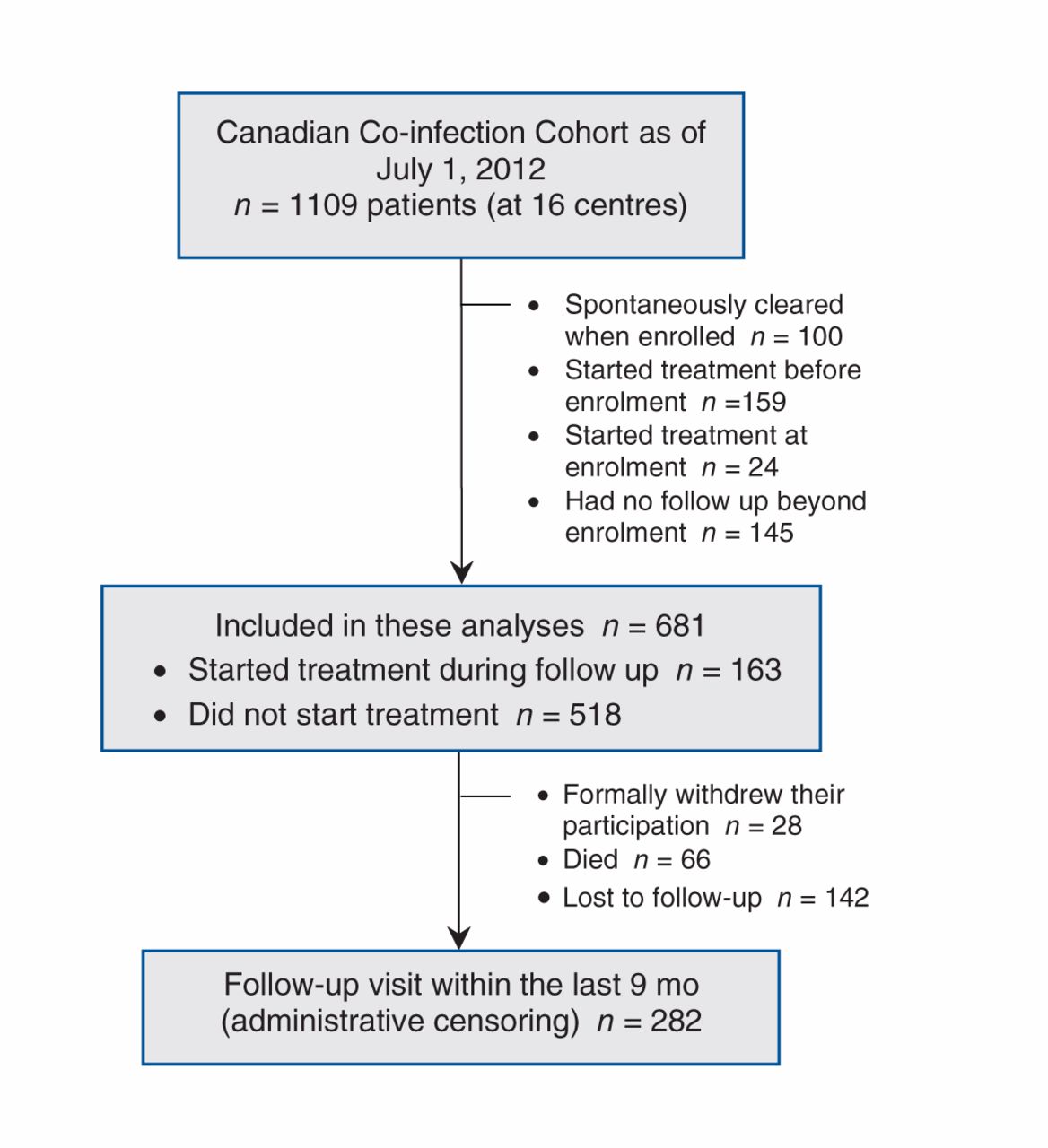
As of July 1, 2012, there were 1109 patients in the cohort; of these, 100 patients had spontaneously cleared HCV when enrolled, 173 patients had started HCV treatment before or at enrolment, and 145 patients had no additional follow-up after enrolment (Figure 1). Of the remaining 681 patients, 163 started HCV treatment over a period of 1827 patient-years (9 patients per 100 years of follow-up). Of the patients who had not started treatment, 94 formally withdrew from the cohort or died; among the remaining 424 patients, 282 (67%) had a follow-up visit within the preceding 9 months.

Flow of patients through the study.
Those who started HCV treatment (either before or at enrolment or during follow-up) were more likely to be infected with HCV genotype 2 or 3 (v. other or unknown genotype) and receiving antiretroviral therapy, and they were less likely to be female, Aboriginal or to report either crack or cocaine use (Table 2). Patients who started HCV treatment had been infected with HCV for a shorter duration but had a higher ratio of aspartate aminotransferase to platelet ratio index (APRI) score, indicating more advanced fibrosis.
In the Weibull model of treatment uptake during follow-up, Aboriginal patients, those infected with HCV for a longer period or who reported the use of crack or cocaine were less likely to start HCV treatment, while those with easier-to-treat HCV genotypes (2 or 3) or higher CD4 cell counts at enrolment were more likely to start HCV treatment (Table 3). Even after adjustment for case mix, there was still appreciable variation in the uptake of treatment between centres (estimated between-centre variance [σ2] = 0.87, 95% credible interval [CI] 0.49–1.5, without informative centre priors), with mean hazard ratios of 0.43 (95% CI 0.11–1.3) and 3.6 (95% CI 1.7–8.4) for the centres least and most likely, respectively, to start the average coinfected patient on HCV treatment. This variation was not reduced by adding informative centre priors to the model (σ2 = 0.90, 95% CI 0.49–1.5) or additional covariates to allow for any differences either between provinces (σ2 = 0.88, 95% CI 0.44–1.6) or between primary and tertiary care centres (σ2 = 0.89, 95% CI 0.49–1.6).
There was considerable uncertainty about which centres were best at starting an average patient on HCV treatment (Figure 2). Adding prior information about centre effects did not reduce the uncertainty in this analysis. However, centres 8 and 15 were particularly effective at starting patients on HCV treatment.
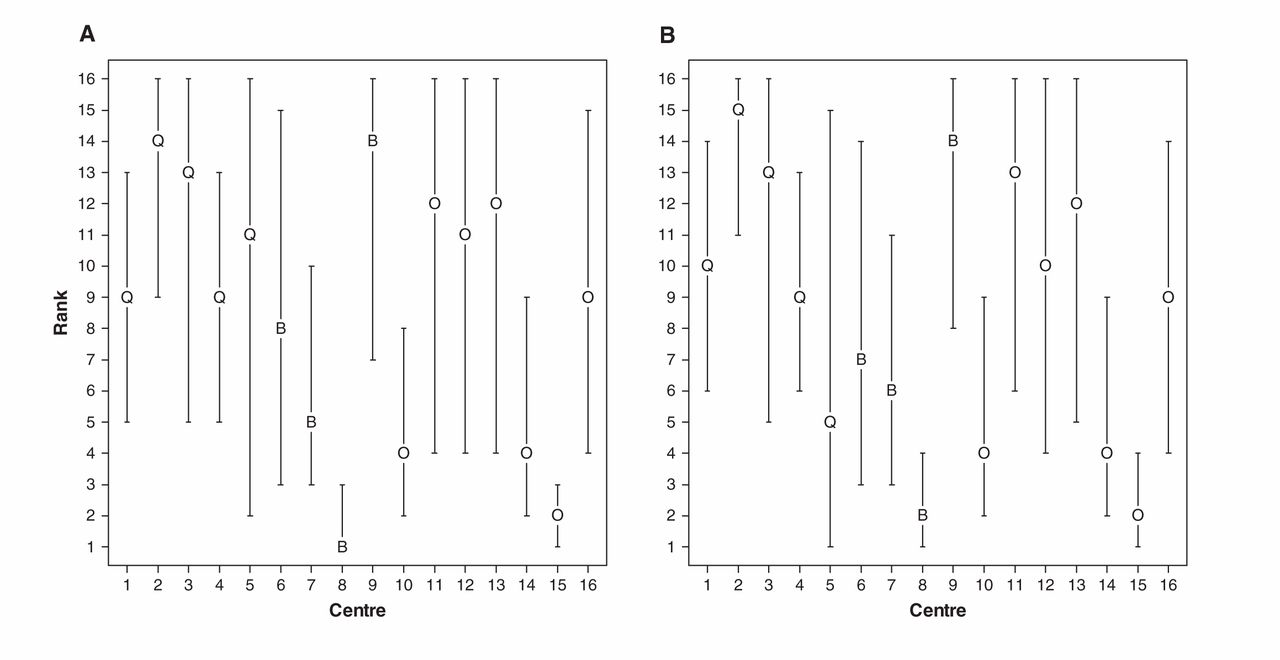
Median rank (95% credible interval) for each of the 16 centres included in the cohort. Rank was ordered from best (1) to worst (16) at starting an average patient on treatment for hepatitis C virus (HCV) during follow-up. There was considerable uncertainty about which centres were best, but centres 8 and 15 appeared particularly effective at starting patients on treatment. The graph on the left shows the centre ranks without informative centre priors. The graph on the right shows the centre ranks when data on HCV treatment before or at enrolment were included in the Weibull time-to-event model as prior information. Including this prior information did not materially reduce the uncertainty about which centres were best starting patients on HCV treatment. Note: B = British Columbia, O = Ontario and Alberta, Q = Quebec and Nova Scotia.
The principal investigator in each centre reported access to tests for HCV, HCV genotyping and liver biopsy, and to hepatologists and nephrologists in all or nearly all centres (Table 4). Neither transient elastography nor addiction services were always available (Table 1), but these services tended to be available at centres where patients were more likely to start HCV treatment. The most important criteria for principal investigators when determining eligibility for treatment were severity of fibrosis (median score 5 [where 1 = less important, 5 = very important]), presence of current psychiatric comorbidities (4), current alcohol intake (4), past HCV treatment (4), a history of reinfection with HCV (4), HCV genotype (3.5) and current injection drug use (3.5) (Table 5). However, the opinions were wide-ranging, and 8 of the 15 criteria elicited both the responses “less important” and “very important.”
Interpretation
Main findings
We found variation in the uptake of HCV treatment between centres that could not be explained by patient-level differences at each centre. The centre-level effects were considerable, relative to the effects of patient characteristics. In the model without informative centre priors, the mean hazard ratios for the centres least and most likely to start an average HCV–HIV coinfected patient on HCV treatment were 0.43 and 3.6, respectively. These between-centre differences seem independent of province or whether treatment took place in a primary care or tertiary hospital setting.
Transient elastography and addiction services tended to be available in centres where patients were more likely to start HCV treatment. This suggests that access to these services might explain between-centre differences. When we added access to these services to our Weibell model (at the request of a reviewer), the latter had no effect, but adding the former reduced the residual variation in treatment uptake between centres (σ2 = 0.74, 95% CI 0.37–1.4). It is plausible that access to these services promotes treatment uptake, given that the severity of fibrosis and drug and alcohol abuse are seen as important criteria by physicians when determining eligibility for treatment. However, it is just as plausible that diverse opinions about the eligibility of patients for treatment are responsible for the between-centre differences, either through centre treatment policies or individual decision-making.
Comparison with other studies
A previous study in the United States showed that provider differences can be as important as patient differences in explaining variability in the uptake of HCV treatment, with institutional differences being far less important.17 This suggests that most of the differences seen in our study between centres are because of individual decision-making rather than access to specialists and services. At the time of our study, regulations governing access to HCV treatment were more restrictive in some provinces than in others: in BC, regulations require biopsy-proven fibrosis or abnormal hepatic transaminase levels; in Alberta and Ontario, the regulations require evidence of fibrosis; and in Quebec and Nova Scotia, the regulations require only the presence of chronic HCV infection. Hence, in our model, we grouped a centre in Alberta with centres in Ontario, and a centre in Nova Scotia with centres in Quebec. In theory, the trend away from federal health care administration could increase disparity in the access to health services between provinces.31,32 The restrictive policies in some provinces have been cited as a barrier to HCV treatment by patients and providers.33 Although we found no evidence of provincial effects in our data, our estimates were not precise enough to rule out such effects.
Limitations
Incomplete adjustment for case mix could lead to an overestimate of the variation between centres. However, our model included covariates for most of the criteria thought to be important by the principal investigators when determining eligibility for treatment. We did not directly adjust for the severity of fibrosis: transient elastography was not routinely used during follow-up (and was not available in some centres), and liver biopsy is impractical in routine care. Instead, we adjusted for the duration of HCV infection because this is a rough proxy for the severity of fibrosis and might, therefore, be expected to influence whether a patients starts treatment. Differences between centres in the rate or characteristics of patients lost to follow-up could lead to an underestimate of the variation between centres (e.g., if patients lost to follow-up were less likely to start treatment). Although it is clear that there are differences between centres in the uptake of treatment, there is considerable uncertainty in the ranking of centres based on their success at starting patients on HCV treatment. Including information about treatment uptake before or at cohort enrolment did not reduce this uncertainty. As a result, our estimates of associations between access to specialists and services and centre rankings are approximate. However, access to transient elastography and addiction services could simply be characteristics of centres where patients are started on treatment, rather than services that encourage treatment uptake if provided.
We did not survey all clinicians working at each centre, and between-centre differences could be due, at least in part, to different levels of clinical experience at each centre or different physician workloads. Web surveys are a relatively quick and anonymous method of data collection, and this can influence responses.34 Our survey did not explore all aspects of clinical decision-making; therefore, its results are exploratory and should be interpreted with caution. Our results may not apply in other settings: for example, in our study, women were less likely than men to start HCV treatment, but in a study of (mostly male) American war veterans, men were less likely than women to start HCV treatment.19 Treatment success is ultimately measured by the rate at which patients achieve a sustained viral response after treatment and not by the rate at which patients start treatment. Nevertheless, a necessary first step to improving treatment success in patients with HIV–HCV coinfection is to convince patients and providers to attempt treatment.
Conclusion
Effective treatment is now available for HCV; such treatment will become even more effective when combined with new direct-acting antivirals. Increased uptake of treatment by patients with HIV–HCV coinfection is essential to reduce the transmission of HCV and to contain future health care costs.35 Programs designed to increase the uptake of HCV treatment among injection drug users are being introduced in Canada,36 although it is not clear how best to improve the unacceptably low rate of uptake in this key patient population.13 Community-based primary care, peer support groups and multidisciplinary care are all approaches that may help.37–39 Patient-related barriers to treatment uptake are important but difficult to overcome. Our results suggest that provider-related barriers are as important as patient-related ones — the magnitude of the centre effects in our study is surprising, as are the diverse opinions held by our principal investigators about the importance of eligibility criteria for treatment. (All but 2 principal investigators had more than 10 years’ experience in clinical practice.) Training and continuing medical education programs have been recommended to widen the pool of clinicians comfortable treating HCV,40 but even specialists can be reluctant to provide treatment to injection drug users.13 Qualitative research is needed to explore whether certain patients would receive HCV treatment in some centres but not in others and, if so, why that is the case. Our results also suggest that there is an urgent need for updated HCV treatment and management guidelines for patients with HIV–HCV coinfection, and that these guidelines need to be disseminated to and adopted by both primary care givers and consultants.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/1/3/E106/suppl/DC1
Acknowledgements
The authors thank Alexandre Schnubb, Allyson Ion, Brenda Beckthold, Elaine Fernandez, Evelyn Maan, Heather Haldane, Jonathan Edwin, Judy Latendre-Paquette, Laura Puri, Nancy McFarland, Renée Pugsley, Anja McNeil and Warmond Chan for their assistance with study coordination, participant recruitment and care.
Footnotes
-
Competing interests: Curtis Cooper has served as a consultant for Merck and Vertex Pharmaceuticals. He has received grants from Merck and Abbot and has received payment for lectures from Merck and Roche. Mark Hull has served as a consultant for Merck, Vertex Pharmaceuticals, Pfizer, Viiv Healthcare and Ortho-Jansen. He has received grants from the National Institute on Drug Abuse, and he has received payment for lectures from Merck and Ortho-Janssen. Sharon Walmsley is a board member and has served as a consultant for Abbott, Merck, Janssen Therapeutics, Gilead, Viiv Healthcare and Bristol-Myers Squibb. She holds grants from Viiv Healthcare and Merck and has received payment for lectures from Abbott, Merck, Janssen Therapeutics, Gilead and Bristol-Myers Squibb. She has received paid travel expenses from Viiv Healthcare, Abbott and Merck. Marina Klein has served as a consultant for GlaxoSmithKline and Viiv Healthcare. She holds grants from Merck. She has received payment for lectures from Bristol-Myers Squibb, GlaxoSmithKline and Viiv Healthcare. She has received payment for developing educational presentations from Gilead, GlaxoSmithKline and Viiv Healthcare. No competing interests declared by Jim Young, Marin Potter, Joseph Cox, John Gill.
-
Contributors: Jim Young, Martin Potter, Joseph Cox and Marina Klein contributed to the study design. Martin Potter was responsible for the survey design. Martin Potter, Joseph Cox, Curtis Cooper, John Gill, Mark Hull, Sharon Walmsley and Marina Klein collected the data. Jim Young is the study guarantor and was responsible for data analysis. Jim Young and Marina Klein drafted the manuscript, which was revised by Martin Potter, Joseph Cox, Curtis Cooper, John Gill, Mark Hull and Sharon Walmsley. All authors approved the final version submitted for publication.
-
Funding: This study was funded by the Fonds de recherche en santé du Québec, Réseau SIDA/maladies infectieuses (FRQS), the Canadian Institutes of Health Research (grant no. MOP-79529) and the CIHR Canadian HIV Trials Network (CTN222). Dr. Marina Klein is supported by a “Chercheur-boursiers cliniciens senior” career award from FRQS.
References
- © 2013 Canadian Medical Association or its licensors
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.