


Article Figures & Tables
Figures
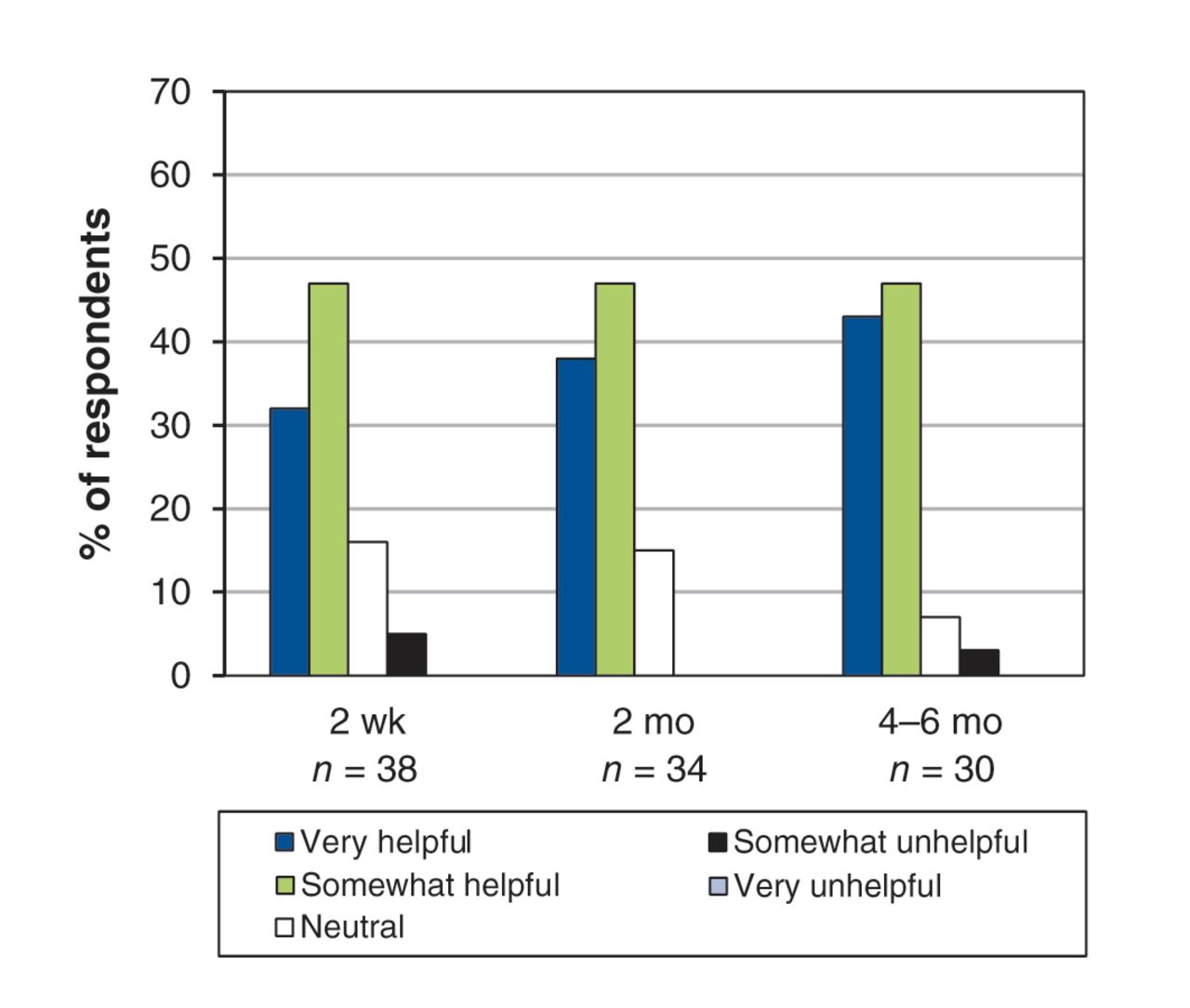
- Figure 1:
Flow of patients through the trial. Overall, 12 patients did not complete the trial (9 dropped out; 3 died); none of the deaths was unexpected or attributed to the use of opioids. (See Appendix 2 for details of attrition, available at www.cmajopen.ca/content/1/1/E27/suppl/DC1.)
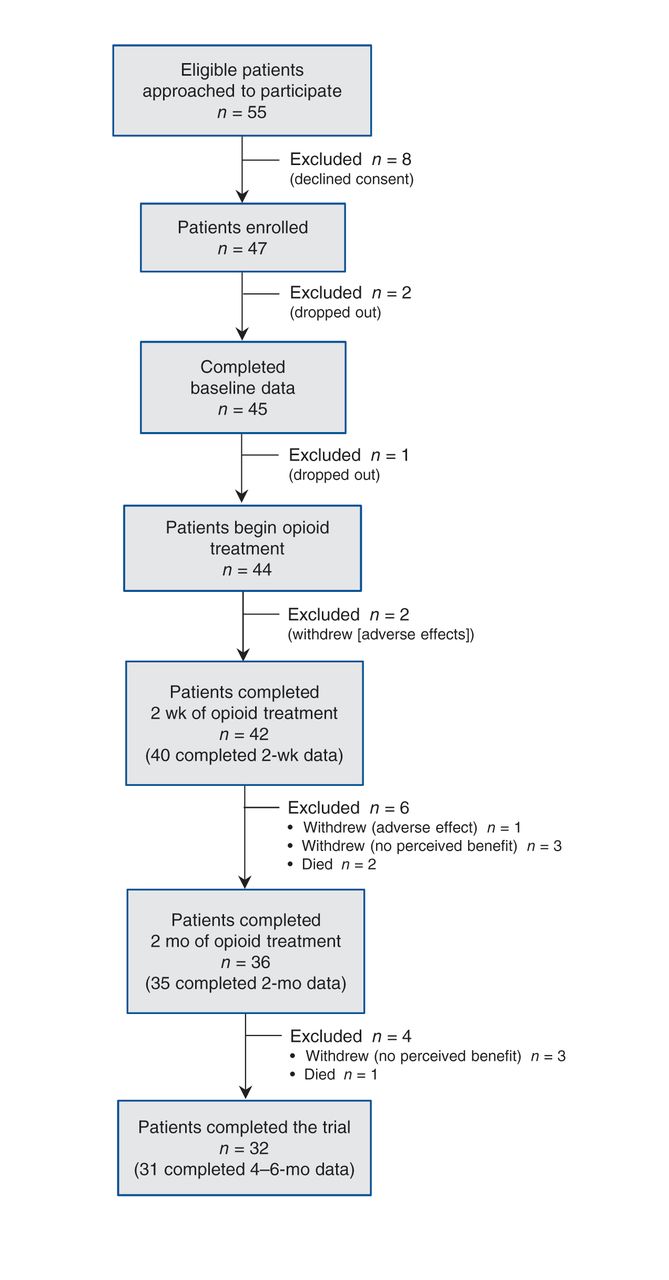
- Figure 2:
Global ratings of “helpfulness” of opioids on 5-point Likert scale.

Tables
Timetable Drug and dosage Dyspnea outcome measure Week 1 At end of week 1, if dyspnea score on Likert scale ≥ 4 (i.e., dyspnea is somewhat intolerable or completely intolerable), then: Day 1, 2 Morphine sulfate 0.5 mg twice daily Day 3, 4 Morphine sulfate 0.5 mg every 4 hours Day 5, 6, 7 Morphine sulfate 1 mg every 4 hours Week 2 Morphine sulfate 2 mg every 4 hours At end of week, if dyspnea score ≥ 4 as above, then: Week 3 Morphine sulfate 3 mg every 4 hours At end of week, if dyspnea score ≥ 4 as above, then: Week 4 Morphine sulfate 5 mg every 4 hours At end of week, if dyspnea score ≥ 4 as above, then: Week 5+ Ongoing titration weekly, with increase of 30%–50% in dose based on severity of dyspnea and adverse effects. If persistent intolerable adverse effects develop, revert to previous tolerated dose and re-evaluate in 48 hours. If adverse effects persist, rotate to hydromorphone or taper dose by 50% per day and stop over 72 hours. Week 6+ Patients who remain on a stable dose of opioid (i.e., have not required titration in the preceding 2 weeks) can switch to a sustained-release preparation. Characteristic No. (%) of patients
n = 45*Sex Female 26 (58) Male 19 (42) Age, yr, median (range) 74 (51–89) Location Nova Scotia 31 (69) New Brunswick 8 (18) Saskatchewan 6 (13) Dyspnea severity MRC 5 37 (82) MRC 4 8 (18) FEV1, % of predicted, mean ± SD (n = 34) 26.8 (8.9) Long-term oxygen use 27 (60) High school education or less 25 (58) Note: MRC = Medical Research Council dyspnea scale, FEV1 = forced expiratory volume in the first second, SD = standard deviation. *Unless stated otherwise.
Measure Median (IQR) p value Baseline
n = 452 wk
n = 392 mo
n = 344–6 mo
n = 31Difference between baseline and 4–6 mo
n = 31Health-related quality of life CRQ 3.5 (2.8 to 4.0) 4.2 (3.8 to 4.7) 4.1 (3.6 to 4.8) 4.2 (3.6 to 4.8) 0.6 (0.1 to 1.3) < 0.001 McGill Quality of Life Questionnaire 5.0 (3.0 to 6.0) –* 5.5 (4.0 to 7.5) 5.0 (5.0 to 7.0) 1.0 (0 to 2.0) 0.053 Dyspnea Numerical rating scale 7.0 (5.0 to 8.0) 5.0 (4.0 to 7.0) 5.0 (4.0 to 6.0) 5.0 (4.0 to 6.0) –2.0 (–3.0 to 1.0) 0.02 CRQ-D 2.8 (2.3 to 3.6) 3.9 (3.0 to 4.5) 3.6 (3.0 to 4.2) 3.9 (2.8 to 4.5) 0.6 (0 to 1.4) 0.004 Anxiety and depression HADS–Anxiety 8.0 (6.0 to 10.0) –* 7.0 (3.0 to 9.0) 7.0 (4.0 to 11.0) –1.5 (–3.0 to 1.0) 0.2 HADS–Depression 8.0 (6.0 to 11.0) –* 6.0 (4.0 to 8.0) 7.0 (5.0 to 9.0) –1.0 (–3.0 to 0.0) 0.08 Note: CRQ = Chronic Respiratory Questionnaire, CRQ-D = dyspnea domain of CRQ, HADS = Hospital Anxiety and Depression Scale, IQR = interquartile range. *Not measured at 2 weeks because we did not anticipate any changes in anxiety or depression at this early stage of opioid therapy.
Symptoms NOSE score,* mean ± SD† Baseline
n = 452 wk
n = 392 mo
n = 344–6 mo
n = 31Nausea/vomiting/lack of appetite 2.23 ± 2.89 1.29 ± 2.13 1.62 ± 2.69 1.71 ± 2.24 Fatigue/trouble concentrating/
hallucinations/drowsiness3.15 ± 2.83 2.10 ± 2.73 2.38 ± 2.62 2.97 ± 2.56 Constipation 2.80 ± 2.80 2.92 ± 3.38 3.33 ± 3.21 3.32 ± 3.11 Itching 2.03 ± 2.90 1.23 ± 1.84 1.66 ± 2.27 1.52 ± 2.61 Decreased sexual desire 4.61 ± 4.79 2.22 ± 3.80 2.39 ± 4.15 3.68 ± 4.61 Dry mouth 5.23 ± 3.53 3.31 ± 2.78 4.59 ± 3.17 4.52‡ ± 3.08 Abdominal pain 2.80 ± 3.13 1.36 ± 1.69 1.88 ± 2.48 1.77 ± 2.22 Sweating 1.58 ± 2.05 1.36 ± 1.91 1.33 ± 1.83 1.42 ± 1.95 Headaches/dizziness 2.08 ± 2.41 1.95 ± 2.45 1.76 ± 2.50 1.84 ± 2.37 Urine retention 1.39 ± 2.14 1.21 ± 2.09 1.15 ± 1.86 1.23 ± 1.61 Minimum completion rate for any question, no. (%) 36 (80) 36 (92) 31 (91) 28 (90) Note: SD = standard deviation. *Scores for self-reported adverse effects were derived with use of the NOSE (Numerical Opioid Side Effect) assessment tool; (21) scores range from 0 (not present) to 10 (bad). †Unless stated otherwise. ‡p < 0.05 compared with baseline.
Statement No. (%) of responses* 2 mo
n = 344–6 months
n = 31 (41 responses*)I would strongly prefer to continue on opioids because they provide significant relief from dyspnea 8 (24) 12 (29) I would strongly prefer to continue on opioids because they provide significant improvement in my quality of life 13 (38) 9 (22) I would prefer to continue on opioids because they provide significant relief from dyspnea 1 (3) 7 (17) I would prefer to continue on opioids because they provide significant improvement in my quality of life 8 (24) 10 (24) I do not have any feelings or preferences one way or another for continuing on opioids or not 3 (8) 3 (7) I would prefer to be tapered off opioids 0 0 I would strongly prefer to be tapered off opioids 1 (3) 0 *Some patients provided more than one response.
Statement No. (%) of responses* 2 mo
n = 324–6 months
n = 27 (29 responses*)Opioids continue to provide significant relief from dyspnea with minimal side effects 16 (50) 13 (45) Opioids continue to provide significant relief from dyspnea but with significant side effects 0 2 (7) Opioids continue to provide significant relief from dyspnea but with side effects that are not tolerable 0 0 Opioids are providing some relief from dyspnea and the side effects are tolerable 14 (44) 10 (34) Opioids are providing some relief from dyspnea but the side effects are not tolerable 0 0 Opioids are not providing much relief from dyspnea but the side effects are tolerable 1 (3) 4 (14) Opioids are not providing much relief from dyspnea but the side effects are not tolerable 1 (3) 0 *Some patients provided more than one response.
In this issue

{kind=link}
{kind=link}
Article tools





